{"title":"二维散斑跟踪超声心动图估计心力衰竭患者左心室激活序列。","authors":"Hideyuki Hara, Tazuru Igarashi, Toyoji Kaida, Masami Murakami, Hiroshi Ito, Shinichi Niwano, Junya Ako","doi":"10.1007/s10554-023-02834-w","DOIUrl":null,"url":null,"abstract":"<p><p>Evaluation of longitudinal strain (LS) from two-dimensional echocardiography is useful for global and regional left ventricular (LV) dysfunction assessment. We determined whether the LS reflects contraction process in patients with asynchronous LV activation. We studied 144 patients with an ejection fraction ≤ 35%, who had left bundle branch block (LBBB, n = 42), right ventricular apical (RVA) pacing (n = 34), LV basal- or mid-lateral pacing (n = 23), and no conduction block (Narrow-QRS, n = 45). LS distribution maps were constructed using 3 standard apical views. The times from the QRS onset-to-early systolic positive peak (Q-EPpeak) and late systolic negative peak (Q-LNpeak) were measured to determine the beginning and end of contractions in each segment. Negative strain in LBBB initially appeared in the septum and basal-lateral contracted late. In RVA and LV pacing, the contracted area enlarged centrifugally from the pacing site. Narrow-QRS showed few regional differences in strain during the systolic period. The Q-EPpeak and Q-LNpeak exhibited similar sequences characterized by septum to basal-lateral via the apical regions in LBBB, apical to basal regions in RVA pacing, and lateral to a relatively large delayed contracted area between the apical- and basal-septum in LV pacing. Differences in Q-LNpeaks between the apical and basal segments in delayed contracted wall were 107 ± 30 ms in LBBB, 133 ± 46 ms in RVA pacing, and 37 ± 20 ms in LV pacing (p < 0.05, between QRS groups). Specific LV contraction processes were demonstrated by evaluating the LS distribution and time-to-peak strain. These evaluations may have potential to estimate the activation sequence in patients with asynchronous LV activation.</p>","PeriodicalId":50332,"journal":{"name":"International Journal of Cardiovascular Imaging","volume":"39 7","pages":"1251-1262"},"PeriodicalIF":1.5000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10250274/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimation of left ventricular activation sequence in patients with heart failure using two-dimensional speckle tracking echocardiography.\",\"authors\":\"Hideyuki Hara, Tazuru Igarashi, Toyoji Kaida, Masami Murakami, Hiroshi Ito, Shinichi Niwano, Junya Ako\",\"doi\":\"10.1007/s10554-023-02834-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Evaluation of longitudinal strain (LS) from two-dimensional echocardiography is useful for global and regional left ventricular (LV) dysfunction assessment. We determined whether the LS reflects contraction process in patients with asynchronous LV activation. We studied 144 patients with an ejection fraction ≤ 35%, who had left bundle branch block (LBBB, n = 42), right ventricular apical (RVA) pacing (n = 34), LV basal- or mid-lateral pacing (n = 23), and no conduction block (Narrow-QRS, n = 45). LS distribution maps were constructed using 3 standard apical views. The times from the QRS onset-to-early systolic positive peak (Q-EPpeak) and late systolic negative peak (Q-LNpeak) were measured to determine the beginning and end of contractions in each segment. Negative strain in LBBB initially appeared in the septum and basal-lateral contracted late. In RVA and LV pacing, the contracted area enlarged centrifugally from the pacing site. Narrow-QRS showed few regional differences in strain during the systolic period. The Q-EPpeak and Q-LNpeak exhibited similar sequences characterized by septum to basal-lateral via the apical regions in LBBB, apical to basal regions in RVA pacing, and lateral to a relatively large delayed contracted area between the apical- and basal-septum in LV pacing. Differences in Q-LNpeaks between the apical and basal segments in delayed contracted wall were 107 ± 30 ms in LBBB, 133 ± 46 ms in RVA pacing, and 37 ± 20 ms in LV pacing (p < 0.05, between QRS groups). Specific LV contraction processes were demonstrated by evaluating the LS distribution and time-to-peak strain. These evaluations may have potential to estimate the activation sequence in patients with asynchronous LV activation.</p>\",\"PeriodicalId\":50332,\"journal\":{\"name\":\"International Journal of Cardiovascular Imaging\",\"volume\":\"39 7\",\"pages\":\"1251-1262\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10250274/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Cardiovascular Imaging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10554-023-02834-w\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiovascular Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10554-023-02834-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
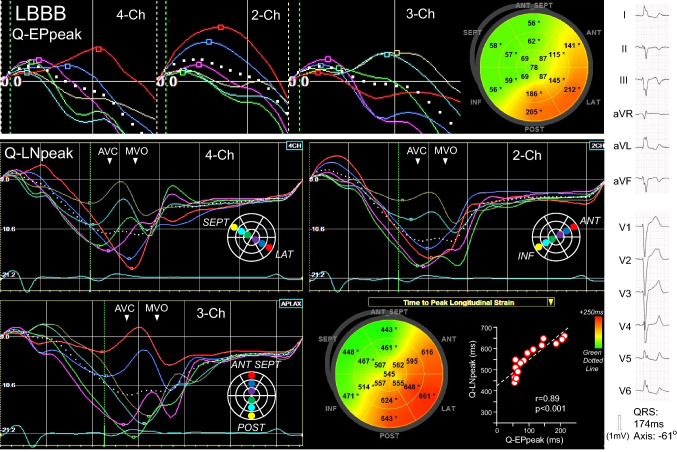
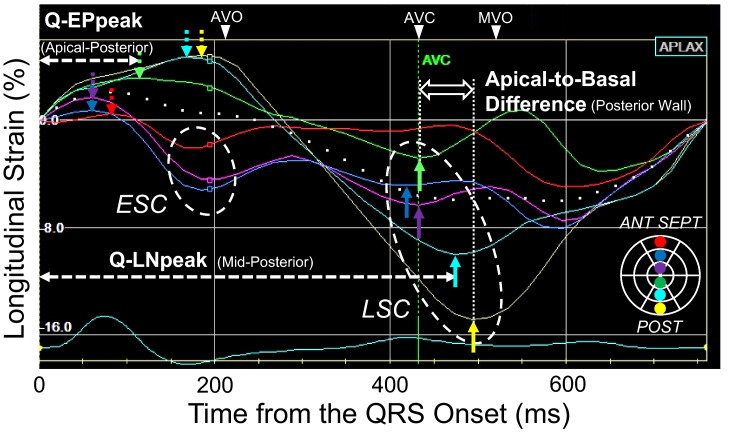
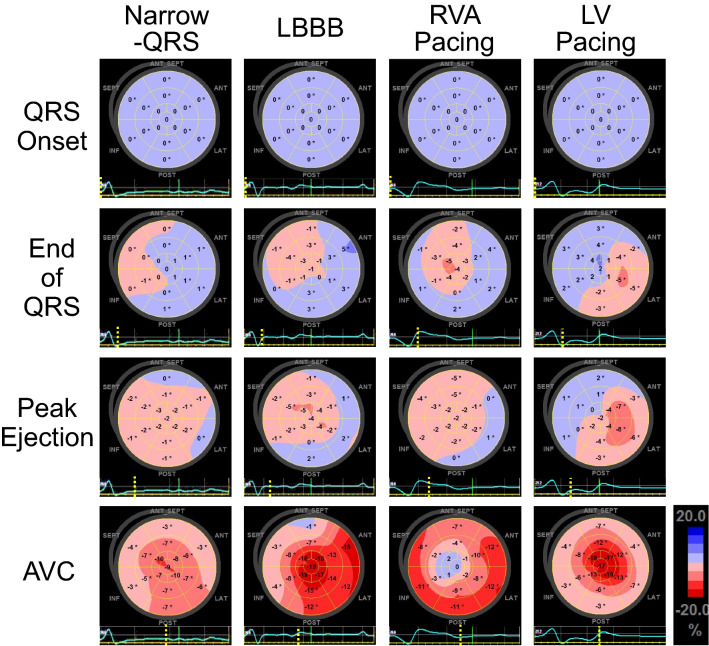
二维超声心动图纵向应变(LS)的评估对整体和局部左室功能障碍的评估是有用的。我们确定了左室非同步激活患者的LS是否反映了收缩过程。我们研究了144例射血分数≤35%的患者,他们分别有左束支阻滞(LBBB, n = 42)、右心室心尖起搏(RVA, n = 34)、左室基底或中侧起搏(n = 23)和无传导阻滞(Narrow-QRS, n = 45)。利用3个标准顶点视图构建LS分布图。测定从QRS发作到收缩期早期正峰(Q-EPpeak)和收缩期晚期负峰(Q-LNpeak)的时间,确定各节段收缩的开始和结束。LBBB负应变最初出现在中隔,基底-外侧收缩较晚。在RVA和LV起搏时,收缩面积从起搏部位离心扩大。窄qrs显示收缩期应变的区域差异不大。Q-EPpeak和Q-LNpeak表现出相似的序列特征,即LBBB的室间隔通过根尖区至基底外侧,RVA起搏的根尖至基底区,左室起搏的根尖和基底间隔之间有一个相对较大的延迟收缩区。延迟收缩壁尖段与基段q - lnpeak的差异分别为:LBBB组107±30 ms, RVA起搏组133±46 ms, LV起搏组37±20 ms (p < 0.05)
Estimation of left ventricular activation sequence in patients with heart failure using two-dimensional speckle tracking echocardiography.
Evaluation of longitudinal strain (LS) from two-dimensional echocardiography is useful for global and regional left ventricular (LV) dysfunction assessment. We determined whether the LS reflects contraction process in patients with asynchronous LV activation. We studied 144 patients with an ejection fraction ≤ 35%, who had left bundle branch block (LBBB, n = 42), right ventricular apical (RVA) pacing (n = 34), LV basal- or mid-lateral pacing (n = 23), and no conduction block (Narrow-QRS, n = 45). LS distribution maps were constructed using 3 standard apical views. The times from the QRS onset-to-early systolic positive peak (Q-EPpeak) and late systolic negative peak (Q-LNpeak) were measured to determine the beginning and end of contractions in each segment. Negative strain in LBBB initially appeared in the septum and basal-lateral contracted late. In RVA and LV pacing, the contracted area enlarged centrifugally from the pacing site. Narrow-QRS showed few regional differences in strain during the systolic period. The Q-EPpeak and Q-LNpeak exhibited similar sequences characterized by septum to basal-lateral via the apical regions in LBBB, apical to basal regions in RVA pacing, and lateral to a relatively large delayed contracted area between the apical- and basal-septum in LV pacing. Differences in Q-LNpeaks between the apical and basal segments in delayed contracted wall were 107 ± 30 ms in LBBB, 133 ± 46 ms in RVA pacing, and 37 ± 20 ms in LV pacing (p < 0.05, between QRS groups). Specific LV contraction processes were demonstrated by evaluating the LS distribution and time-to-peak strain. These evaluations may have potential to estimate the activation sequence in patients with asynchronous LV activation.
期刊介绍:
The International Journal of Cardiovascular Imaging publishes technical and clinical communications (original articles, review articles and editorial comments) associated with cardiovascular diseases. The technical communications include the research, development and evaluation of novel imaging methods in the various imaging domains. These domains include magnetic resonance imaging, computed tomography, X-ray imaging, intravascular imaging, and applications in nuclear cardiology and echocardiography, and any combination of these techniques. Of particular interest are topics in medical image processing and image-guided interventions. Clinical applications of such imaging techniques include improved diagnostic approaches, treatment , prognosis and follow-up of cardiovascular patients. Topics include: multi-center or larger individual studies dealing with risk stratification and imaging utilization, applications for better characterization of cardiovascular diseases, and assessment of the efficacy of new drugs and interventional devices.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
