Casey L Johnson, William Woodward, Annabelle McCourt, Cameron Dockerill, Samuel Krasner, Mark Monaghan, Roxy Senior, Daniel X Augustine, Maria Paton, Jamie O'Driscoll, David Oxborough, Keith Pearce, Shaun Robinson, James Willis, Rajan Sharma, Apostolos Tsiachristas, Paul Leeson
{"title":"英国压力超声心动图后的真实世界医院费用:来自EVAREST/BSE-NSTEP多中心研究的成本研究","authors":"Casey L Johnson, William Woodward, Annabelle McCourt, Cameron Dockerill, Samuel Krasner, Mark Monaghan, Roxy Senior, Daniel X Augustine, Maria Paton, Jamie O'Driscoll, David Oxborough, Keith Pearce, Shaun Robinson, James Willis, Rajan Sharma, Apostolos Tsiachristas, Paul Leeson","doi":"10.1186/s44156-023-00020-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Stress echocardiography is widely used to detect coronary artery disease, but little evidence on downstream hospital costs in real-world practice is available. We examined how stress echocardiography accuracy and downstream hospital costs vary across NHS hospitals and identified key factors that affect costs to help inform future clinical planning and guidelines.</p><p><strong>Methods: </strong>Data on 7636 patients recruited from 31 NHS hospitals within the UK between 2014 and 2020 as part of EVAREST/BSE-NSTEP clinical study, were used. Data included all diagnostic tests, procedures, and hospital admissions for 12 months after a stress echocardiogram and were costed using the NHS national unit costs. A decision tree was built to illustrate the clinical pathway and estimate average downstream hospital costs. Multi-level regression analysis was performed to identify variation in accuracy and costs at both patient, procedural, and hospital level. Linear regression and extrapolation were used to estimate annual hospital cost-savings associated with increasing predictive accuracy at hospital and national level.</p><p><strong>Results: </strong>Stress echocardiography accuracy varied with patient, hospital and operator characteristics. Hypertension, presence of wall motion abnormalities and higher number of hospital cardiology outpatient attendances annually reduced accuracy, adjusted odds ratio of 0.78 (95% CI 0.65 to 0.93), 0.27 (95% CI 0.15 to 0.48), 0.99 (95% CI 0.98 to 0.99) respectively, whereas a prior myocardial infarction, angiotensin receptor blocker medication, and greater operator experience increased accuracy, adjusted odds ratio of 1.77 (95% CI 1.34 to 2.33), 1.64 (95% CI 1.22 to 2.22), and 1.06 (95% CI 1.02 to 1.09) respectively. Average downstream costs were £646 per patient (SD 1796) with significant variation across hospitals. The average downstream costs between the 31 hospitals varied from £384-1730 per patient. False positive and false negative tests were associated with average downstream costs of £1446 (SD £601) and £4192 (SD 3332) respectively, driven by increased non-elective hospital admissions, adjusted odds ratio 2.48 (95% CI 1.08 to 5.66), 21.06 (95% CI 10.41 to 42.59) respectively. We estimated that an increase in accuracy by 1 percentage point could save the NHS in the UK £3.2 million annually.</p><p><strong>Conclusion: </strong>This study provides real-world evidence of downstream costs associated with stress echocardiography practice in the UK and estimates how improvements in accuracy could impact healthcare expenditure in the NHS. A real-world downstream costing approach could be adopted more widely in evaluation of imaging tests and interventions to reflect actual value for money and support realistic planning.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"10 1","pages":"8"},"PeriodicalIF":2.4000,"publicationDate":"2023-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10230715/pdf/","citationCount":"1","resultStr":"{\"title\":\"Real world hospital costs following stress echocardiography in the UK: a costing study from the EVAREST/BSE-NSTEP multi-entre study.\",\"authors\":\"Casey L Johnson, William Woodward, Annabelle McCourt, Cameron Dockerill, Samuel Krasner, Mark Monaghan, Roxy Senior, Daniel X Augustine, Maria Paton, Jamie O'Driscoll, David Oxborough, Keith Pearce, Shaun Robinson, James Willis, Rajan Sharma, Apostolos Tsiachristas, Paul Leeson\",\"doi\":\"10.1186/s44156-023-00020-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Stress echocardiography is widely used to detect coronary artery disease, but little evidence on downstream hospital costs in real-world practice is available. We examined how stress echocardiography accuracy and downstream hospital costs vary across NHS hospitals and identified key factors that affect costs to help inform future clinical planning and guidelines.</p><p><strong>Methods: </strong>Data on 7636 patients recruited from 31 NHS hospitals within the UK between 2014 and 2020 as part of EVAREST/BSE-NSTEP clinical study, were used. Data included all diagnostic tests, procedures, and hospital admissions for 12 months after a stress echocardiogram and were costed using the NHS national unit costs. A decision tree was built to illustrate the clinical pathway and estimate average downstream hospital costs. Multi-level regression analysis was performed to identify variation in accuracy and costs at both patient, procedural, and hospital level. Linear regression and extrapolation were used to estimate annual hospital cost-savings associated with increasing predictive accuracy at hospital and national level.</p><p><strong>Results: </strong>Stress echocardiography accuracy varied with patient, hospital and operator characteristics. Hypertension, presence of wall motion abnormalities and higher number of hospital cardiology outpatient attendances annually reduced accuracy, adjusted odds ratio of 0.78 (95% CI 0.65 to 0.93), 0.27 (95% CI 0.15 to 0.48), 0.99 (95% CI 0.98 to 0.99) respectively, whereas a prior myocardial infarction, angiotensin receptor blocker medication, and greater operator experience increased accuracy, adjusted odds ratio of 1.77 (95% CI 1.34 to 2.33), 1.64 (95% CI 1.22 to 2.22), and 1.06 (95% CI 1.02 to 1.09) respectively. Average downstream costs were £646 per patient (SD 1796) with significant variation across hospitals. The average downstream costs between the 31 hospitals varied from £384-1730 per patient. False positive and false negative tests were associated with average downstream costs of £1446 (SD £601) and £4192 (SD 3332) respectively, driven by increased non-elective hospital admissions, adjusted odds ratio 2.48 (95% CI 1.08 to 5.66), 21.06 (95% CI 10.41 to 42.59) respectively. We estimated that an increase in accuracy by 1 percentage point could save the NHS in the UK £3.2 million annually.</p><p><strong>Conclusion: </strong>This study provides real-world evidence of downstream costs associated with stress echocardiography practice in the UK and estimates how improvements in accuracy could impact healthcare expenditure in the NHS. A real-world downstream costing approach could be adopted more widely in evaluation of imaging tests and interventions to reflect actual value for money and support realistic planning.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"10 1\",\"pages\":\"8\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2023-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10230715/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-023-00020-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-023-00020-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
背景:应激超声心动图被广泛用于检测冠状动脉疾病,但在现实世界的实践中,关于下游医院费用的证据很少。我们研究了压力超声心动图准确性和下游医院成本在NHS医院之间的差异,并确定了影响成本的关键因素,以帮助告知未来的临床计划和指南。方法:2014年至2020年间,作为EVAREST/BSE-NSTEP临床研究的一部分,从英国31家NHS医院招募了7636名患者的数据。数据包括所有诊断测试、程序和应激超声心动图后12个月的住院情况,并使用NHS国家单位成本进行成本计算。建立决策树来说明临床路径和估计平均下游医院成本。进行多水平回归分析,以确定在患者、程序和医院水平上准确性和成本的变化。使用线性回归和外推法来估计与医院和国家一级预测准确性提高相关的年度医院成本节约。结果:应激超声心动图的准确性随患者、医院和操作人员的不同而不同。高血压、壁运动异常的存在和每年较多的医院心脏病门诊人数降低了准确性,调整优势比分别为0.78 (95% CI 0.65至0.93)、0.27 (95% CI 0.15至0.48)、0.99 (95% CI 0.98至0.99),而既往心肌梗死、血管紧张素受体阻滞剂用药和更丰富的操作经验提高了准确性,调整优势比分别为1.77 (95% CI 1.34至2.33)、1.64 (95% CI 1.22至2.22)。和1.06 (95% CI 1.02 ~ 1.09)。平均下游成本为每位患者646英镑(SD 1796),各医院差异显著。31家医院的平均下游费用从每位患者384-1730英镑不等。假阳性和假阴性检测分别与平均下游成本1446英镑(标准差为601英镑)和4192英镑(标准差为3332英镑)相关,这是由于非选择性住院人数增加所致,调整优势比分别为2.48 (95% CI 1.08至5.66)和21.06 (95% CI 10.41至42.59)。我们估计,准确率提高1个百分点,每年可以为英国国民健康保险制度节省320万英镑。结论:本研究提供了与英国应激超声心动图实践相关的下游成本的真实证据,并估计了准确性的提高如何影响NHS的医疗保健支出。在评价成像测试和干预措施时,可以更广泛地采用实际的下游成本计算方法,以反映实际的资金价值并支持现实的规划。
Real world hospital costs following stress echocardiography in the UK: a costing study from the EVAREST/BSE-NSTEP multi-entre study.
Background: Stress echocardiography is widely used to detect coronary artery disease, but little evidence on downstream hospital costs in real-world practice is available. We examined how stress echocardiography accuracy and downstream hospital costs vary across NHS hospitals and identified key factors that affect costs to help inform future clinical planning and guidelines.
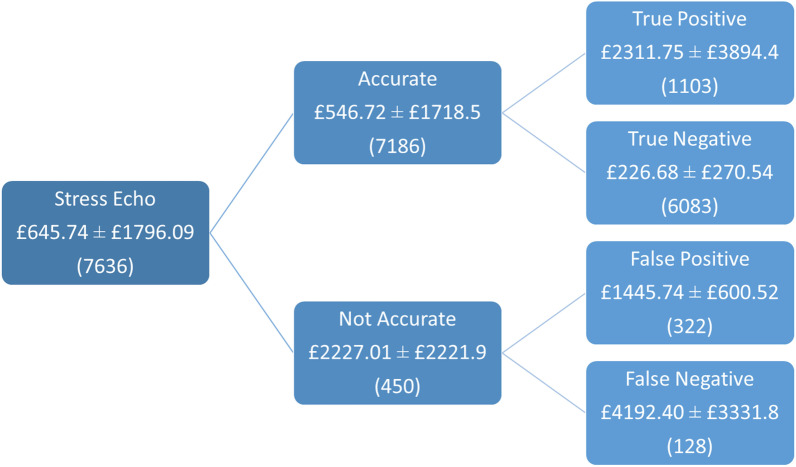
Methods: Data on 7636 patients recruited from 31 NHS hospitals within the UK between 2014 and 2020 as part of EVAREST/BSE-NSTEP clinical study, were used. Data included all diagnostic tests, procedures, and hospital admissions for 12 months after a stress echocardiogram and were costed using the NHS national unit costs. A decision tree was built to illustrate the clinical pathway and estimate average downstream hospital costs. Multi-level regression analysis was performed to identify variation in accuracy and costs at both patient, procedural, and hospital level. Linear regression and extrapolation were used to estimate annual hospital cost-savings associated with increasing predictive accuracy at hospital and national level.
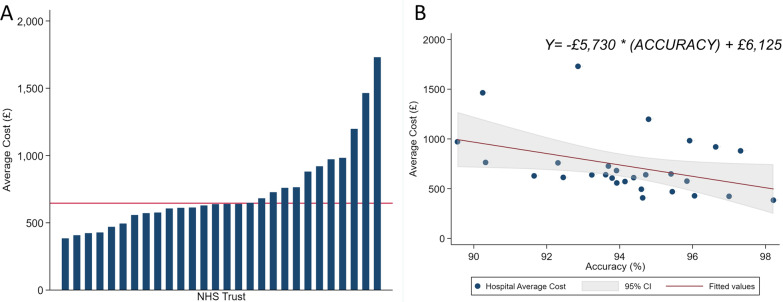
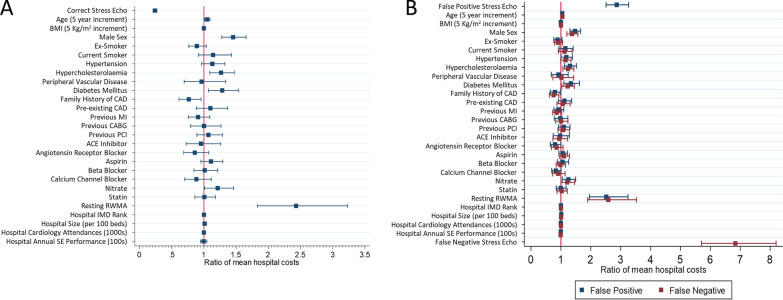
Results: Stress echocardiography accuracy varied with patient, hospital and operator characteristics. Hypertension, presence of wall motion abnormalities and higher number of hospital cardiology outpatient attendances annually reduced accuracy, adjusted odds ratio of 0.78 (95% CI 0.65 to 0.93), 0.27 (95% CI 0.15 to 0.48), 0.99 (95% CI 0.98 to 0.99) respectively, whereas a prior myocardial infarction, angiotensin receptor blocker medication, and greater operator experience increased accuracy, adjusted odds ratio of 1.77 (95% CI 1.34 to 2.33), 1.64 (95% CI 1.22 to 2.22), and 1.06 (95% CI 1.02 to 1.09) respectively. Average downstream costs were £646 per patient (SD 1796) with significant variation across hospitals. The average downstream costs between the 31 hospitals varied from £384-1730 per patient. False positive and false negative tests were associated with average downstream costs of £1446 (SD £601) and £4192 (SD 3332) respectively, driven by increased non-elective hospital admissions, adjusted odds ratio 2.48 (95% CI 1.08 to 5.66), 21.06 (95% CI 10.41 to 42.59) respectively. We estimated that an increase in accuracy by 1 percentage point could save the NHS in the UK £3.2 million annually.
Conclusion: This study provides real-world evidence of downstream costs associated with stress echocardiography practice in the UK and estimates how improvements in accuracy could impact healthcare expenditure in the NHS. A real-world downstream costing approach could be adopted more widely in evaluation of imaging tests and interventions to reflect actual value for money and support realistic planning.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
