{"title":"预测阻塞性冠状动脉疾病患者4年预后的心血管风险评分的比较与优化","authors":"Taichun Qiu, Chunxiao Liang, Bing Ming, Gaoyuan Liu, Furong Zhang, Ruxue Zeng, Dongmei Xie, Qing Zou","doi":"10.2147/TCRM.S404351","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>How well cardiovascular risk models perform in selected atherosclerosis patients for predicting outcomes is unknown. We sought to compare the performance of cardiovascular risk models (Framingham, Globorisk, SCORE2 & SCORE2-OP, and an updated new model) in predicting the 4-year outcome of patients with obstructive coronary artery disease (CAD).</p><p><strong>Methods: </strong>Patients with suspected CAD who underwent coronary computed tomography angiography (CCTA) were recruited. Obstructive CAD was defined from CCTA as ≥ 50% stenosis. Computed tomography images, the scores of the cardiovascular risk models, and 4-year composite endpoints were assessed. Whether the patients underwent revascularization within 60 days after CCTA was also recorded. Multivariate regression analysis and receiver operating characteristics (ROC) curve analysis were performed.</p><p><strong>Results: </strong>A total of 95 patients (mean age: 69.5 ± 10.33 years; 69 males) with obstructive CAD were included in this study. After the ROC analysis, the Framingham, Globorisk, SCORE2 & SCORE2-OP risk score showed prediction values with AUC 0.628 (95% CI: 0.532-0.725), 0.647 (95% CI: 0.542-0.742), 0.684 (95% CI: 0.581-0.776), respectively. Multivariate regression analysis showed that, among the three risk models, only SCORE2 & SCORE2-OP risk score was associated with composite endpoints (hazard ratio: 1.050; 95% CI: 1.021-1.079; <i>p</i> = 0.001) after adjusting for confounding factors. The AUC of the new risk model by combing SCORE2 & SCORE2-OP risk score with revascularization and the number of obstructive vessels in predicting composite endpoints reached 0.898 (95% CI: 0.819-0.951).</p><p><strong>Conclusion: </strong>The SCORE2 & SCORE2-OP risk score combined with the number of obstructive vessels and revascularization is predictive for adverse outcomes in patients with obstructive CAD.</p>","PeriodicalId":48769,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"19 ","pages":"319-328"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/46/tcrm-19-319.PMC10082600.pdf","citationCount":"0","resultStr":"{\"title\":\"Comparison and Optimization of Cardiovascular Risk Scores in Predicting the 4-Year Outcome of Patients with Obstructive Coronary Arteries Disease.\",\"authors\":\"Taichun Qiu, Chunxiao Liang, Bing Ming, Gaoyuan Liu, Furong Zhang, Ruxue Zeng, Dongmei Xie, Qing Zou\",\"doi\":\"10.2147/TCRM.S404351\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>How well cardiovascular risk models perform in selected atherosclerosis patients for predicting outcomes is unknown. We sought to compare the performance of cardiovascular risk models (Framingham, Globorisk, SCORE2 & SCORE2-OP, and an updated new model) in predicting the 4-year outcome of patients with obstructive coronary artery disease (CAD).</p><p><strong>Methods: </strong>Patients with suspected CAD who underwent coronary computed tomography angiography (CCTA) were recruited. Obstructive CAD was defined from CCTA as ≥ 50% stenosis. Computed tomography images, the scores of the cardiovascular risk models, and 4-year composite endpoints were assessed. Whether the patients underwent revascularization within 60 days after CCTA was also recorded. Multivariate regression analysis and receiver operating characteristics (ROC) curve analysis were performed.</p><p><strong>Results: </strong>A total of 95 patients (mean age: 69.5 ± 10.33 years; 69 males) with obstructive CAD were included in this study. After the ROC analysis, the Framingham, Globorisk, SCORE2 & SCORE2-OP risk score showed prediction values with AUC 0.628 (95% CI: 0.532-0.725), 0.647 (95% CI: 0.542-0.742), 0.684 (95% CI: 0.581-0.776), respectively. Multivariate regression analysis showed that, among the three risk models, only SCORE2 & SCORE2-OP risk score was associated with composite endpoints (hazard ratio: 1.050; 95% CI: 1.021-1.079; <i>p</i> = 0.001) after adjusting for confounding factors. The AUC of the new risk model by combing SCORE2 & SCORE2-OP risk score with revascularization and the number of obstructive vessels in predicting composite endpoints reached 0.898 (95% CI: 0.819-0.951).</p><p><strong>Conclusion: </strong>The SCORE2 & SCORE2-OP risk score combined with the number of obstructive vessels and revascularization is predictive for adverse outcomes in patients with obstructive CAD.</p>\",\"PeriodicalId\":48769,\"journal\":{\"name\":\"Therapeutics and Clinical Risk Management\",\"volume\":\"19 \",\"pages\":\"319-328\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/46/tcrm-19-319.PMC10082600.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutics and Clinical Risk Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/TCRM.S404351\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S404351","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Comparison and Optimization of Cardiovascular Risk Scores in Predicting the 4-Year Outcome of Patients with Obstructive Coronary Arteries Disease.
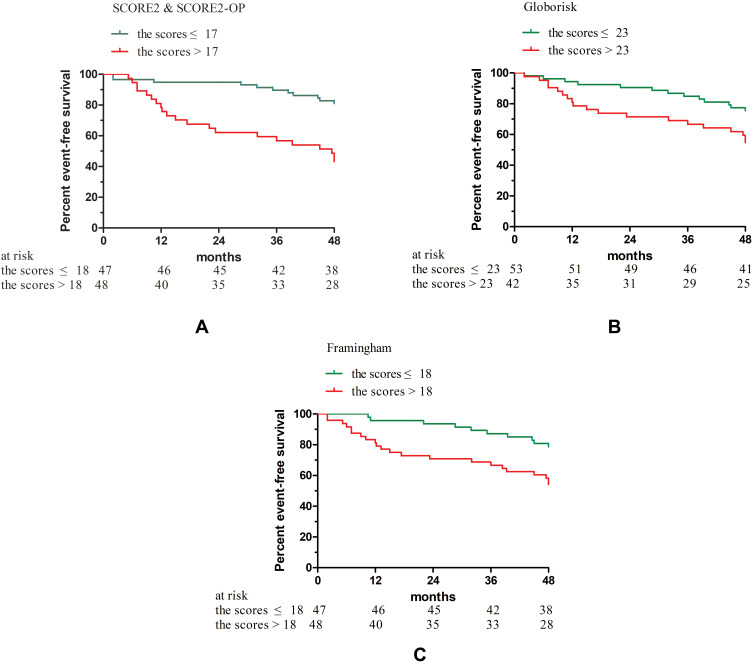
Objective: How well cardiovascular risk models perform in selected atherosclerosis patients for predicting outcomes is unknown. We sought to compare the performance of cardiovascular risk models (Framingham, Globorisk, SCORE2 & SCORE2-OP, and an updated new model) in predicting the 4-year outcome of patients with obstructive coronary artery disease (CAD).
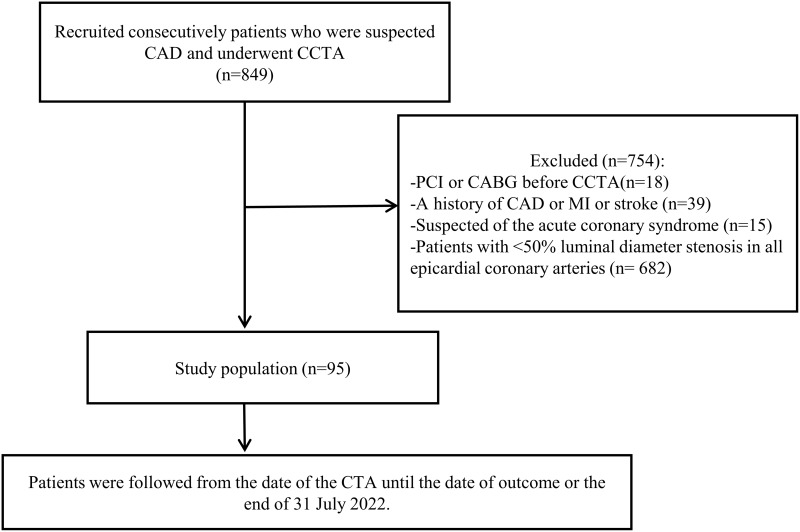
Methods: Patients with suspected CAD who underwent coronary computed tomography angiography (CCTA) were recruited. Obstructive CAD was defined from CCTA as ≥ 50% stenosis. Computed tomography images, the scores of the cardiovascular risk models, and 4-year composite endpoints were assessed. Whether the patients underwent revascularization within 60 days after CCTA was also recorded. Multivariate regression analysis and receiver operating characteristics (ROC) curve analysis were performed.
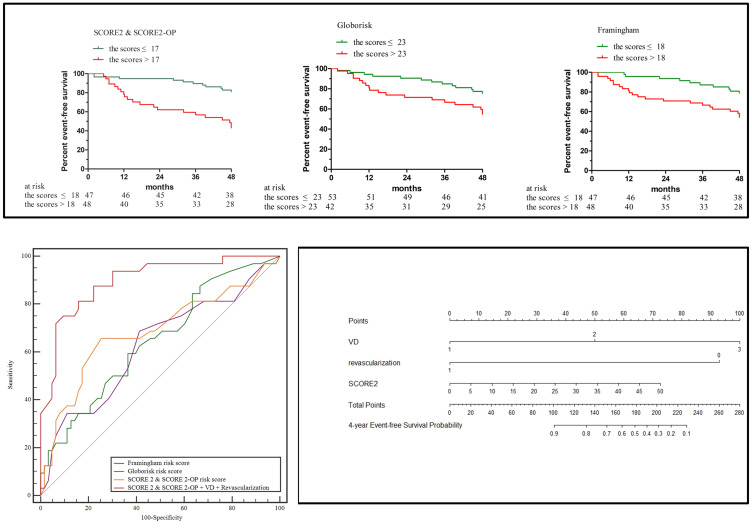
Results: A total of 95 patients (mean age: 69.5 ± 10.33 years; 69 males) with obstructive CAD were included in this study. After the ROC analysis, the Framingham, Globorisk, SCORE2 & SCORE2-OP risk score showed prediction values with AUC 0.628 (95% CI: 0.532-0.725), 0.647 (95% CI: 0.542-0.742), 0.684 (95% CI: 0.581-0.776), respectively. Multivariate regression analysis showed that, among the three risk models, only SCORE2 & SCORE2-OP risk score was associated with composite endpoints (hazard ratio: 1.050; 95% CI: 1.021-1.079; p = 0.001) after adjusting for confounding factors. The AUC of the new risk model by combing SCORE2 & SCORE2-OP risk score with revascularization and the number of obstructive vessels in predicting composite endpoints reached 0.898 (95% CI: 0.819-0.951).
Conclusion: The SCORE2 & SCORE2-OP risk score combined with the number of obstructive vessels and revascularization is predictive for adverse outcomes in patients with obstructive CAD.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
