Medhat Gamal, Ahmed Hasanin, Nada Adly, Maha Mostafa, Ahmed M Yonis, Ashraf Rady, Nasr M Abdallah, Mohammed Ibrahim, Mohamed Elsayad
{"title":"热成像预测锁骨上臂丛神经阻滞失败:一项前瞻性观察研究。","authors":"Medhat Gamal, Ahmed Hasanin, Nada Adly, Maha Mostafa, Ahmed M Yonis, Ashraf Rady, Nasr M Abdallah, Mohammed Ibrahim, Mohamed Elsayad","doi":"10.2147/LRA.S406057","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Successful brachial plexus blockade produces sympathetic blockade, resulting in increased skin temperature in the blocked segments. This study aimed to evaluate the accuracy of infrared thermography in predicting failed segmental supraclavicular brachial plexus block.</p><p><strong>Methods: </strong>This prospective observational study included adult patients undergoing upper-limb surgery under supraclavicular brachial plexus block. Sensation was evaluated at the dermatomal distribution of the ulnar, median, and radial nerves. Block failure was defined as absence of complete sensory loss 30 min after block completion. Skin temperature was evaluated by infrared thermography at the dermatomal supply of the ulnar, median, and radial nerves at baseline, 5, 10, 15, and 20 min after block completion. The temperature change from the baseline measurement was calculated for each time point. Outcomes were the ability of temperature change at each site to predict failed block of the corresponding nerve using area under receiver-operating characteristic curve (AUC) analysis.</p><p><strong>Results: </strong>Eighty patients were available for the final analysis. The AUC (95% confidence interval [CI]) for the ability of temperature change at 5 min to predict failed ulnar, median, and radial nerve block was 0.79 (0.68-0.87), 0.77 (0.67-0.86), and 0.79 (0.69-0.88). The AUC (95% CI) increased progressively and reached its maximum values at 15 min (ulnar nerve 0.98 [0.92-1.00], median nerve 0.97 [0.90-0.99], radial nerve 0.96 [0.89-0.99]) with negative predictive value of 100%.</p><p><strong>Conclusion: </strong>Infrared thermography of different skin segments provides an accurate tool for predicting failed supraclavicular brachial plexus block. Increased skin temperature at each segment can exclude block failure in the corresponding nerve with 100% accuracy.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"71-80"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/99/71/lra-16-71.PMC10263017.pdf","citationCount":"0","resultStr":"{\"title\":\"Thermal Imaging to Predict Failed Supraclavicular Brachial Plexus Block: A Prospective Observational Study.\",\"authors\":\"Medhat Gamal, Ahmed Hasanin, Nada Adly, Maha Mostafa, Ahmed M Yonis, Ashraf Rady, Nasr M Abdallah, Mohammed Ibrahim, Mohamed Elsayad\",\"doi\":\"10.2147/LRA.S406057\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Successful brachial plexus blockade produces sympathetic blockade, resulting in increased skin temperature in the blocked segments. This study aimed to evaluate the accuracy of infrared thermography in predicting failed segmental supraclavicular brachial plexus block.</p><p><strong>Methods: </strong>This prospective observational study included adult patients undergoing upper-limb surgery under supraclavicular brachial plexus block. Sensation was evaluated at the dermatomal distribution of the ulnar, median, and radial nerves. Block failure was defined as absence of complete sensory loss 30 min after block completion. Skin temperature was evaluated by infrared thermography at the dermatomal supply of the ulnar, median, and radial nerves at baseline, 5, 10, 15, and 20 min after block completion. The temperature change from the baseline measurement was calculated for each time point. Outcomes were the ability of temperature change at each site to predict failed block of the corresponding nerve using area under receiver-operating characteristic curve (AUC) analysis.</p><p><strong>Results: </strong>Eighty patients were available for the final analysis. The AUC (95% confidence interval [CI]) for the ability of temperature change at 5 min to predict failed ulnar, median, and radial nerve block was 0.79 (0.68-0.87), 0.77 (0.67-0.86), and 0.79 (0.69-0.88). The AUC (95% CI) increased progressively and reached its maximum values at 15 min (ulnar nerve 0.98 [0.92-1.00], median nerve 0.97 [0.90-0.99], radial nerve 0.96 [0.89-0.99]) with negative predictive value of 100%.</p><p><strong>Conclusion: </strong>Infrared thermography of different skin segments provides an accurate tool for predicting failed supraclavicular brachial plexus block. Increased skin temperature at each segment can exclude block failure in the corresponding nerve with 100% accuracy.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\"16 \",\"pages\":\"71-80\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/99/71/lra-16-71.PMC10263017.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S406057\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S406057","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Thermal Imaging to Predict Failed Supraclavicular Brachial Plexus Block: A Prospective Observational Study.
Background: Successful brachial plexus blockade produces sympathetic blockade, resulting in increased skin temperature in the blocked segments. This study aimed to evaluate the accuracy of infrared thermography in predicting failed segmental supraclavicular brachial plexus block.
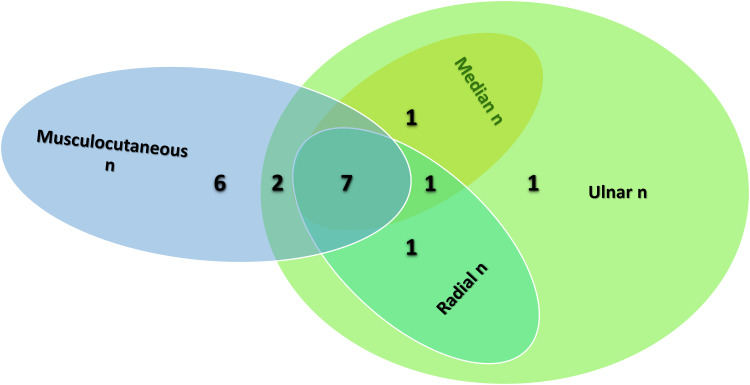
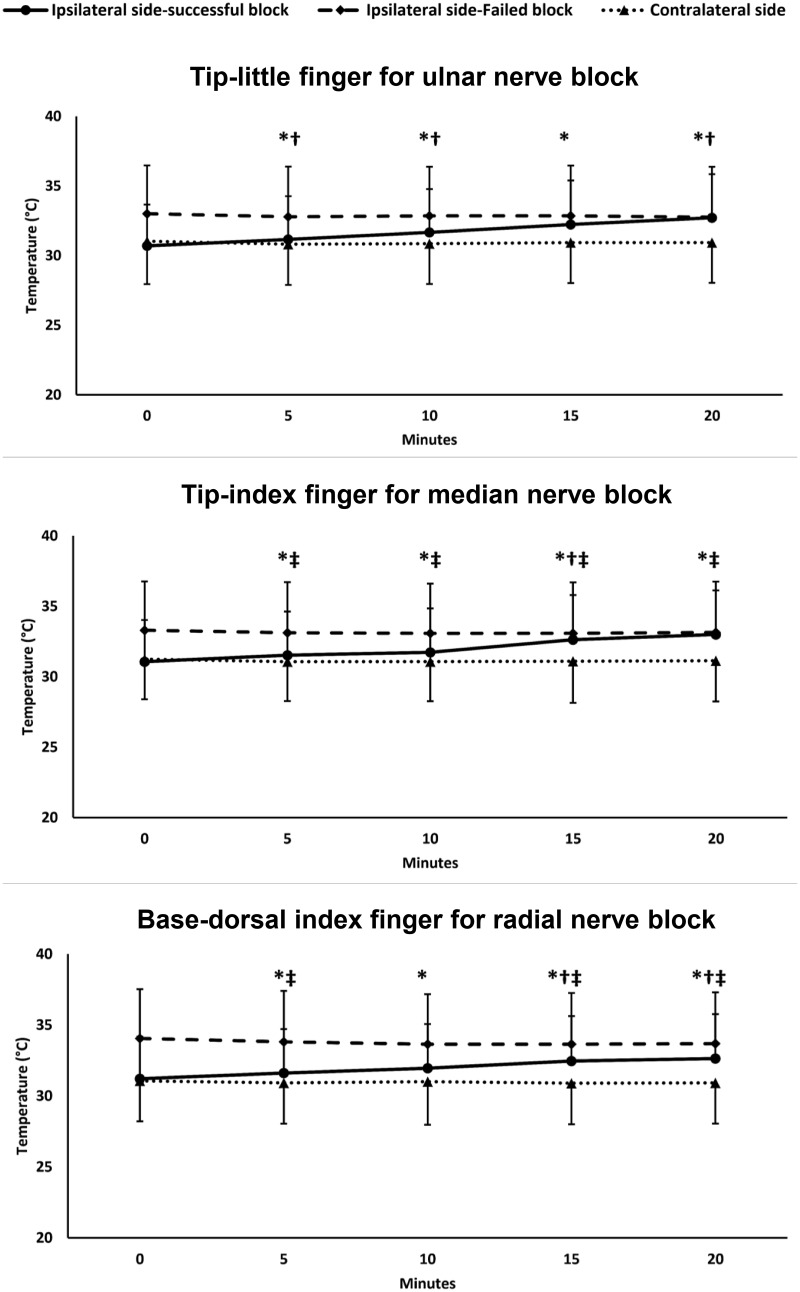
Methods: This prospective observational study included adult patients undergoing upper-limb surgery under supraclavicular brachial plexus block. Sensation was evaluated at the dermatomal distribution of the ulnar, median, and radial nerves. Block failure was defined as absence of complete sensory loss 30 min after block completion. Skin temperature was evaluated by infrared thermography at the dermatomal supply of the ulnar, median, and radial nerves at baseline, 5, 10, 15, and 20 min after block completion. The temperature change from the baseline measurement was calculated for each time point. Outcomes were the ability of temperature change at each site to predict failed block of the corresponding nerve using area under receiver-operating characteristic curve (AUC) analysis.
Results: Eighty patients were available for the final analysis. The AUC (95% confidence interval [CI]) for the ability of temperature change at 5 min to predict failed ulnar, median, and radial nerve block was 0.79 (0.68-0.87), 0.77 (0.67-0.86), and 0.79 (0.69-0.88). The AUC (95% CI) increased progressively and reached its maximum values at 15 min (ulnar nerve 0.98 [0.92-1.00], median nerve 0.97 [0.90-0.99], radial nerve 0.96 [0.89-0.99]) with negative predictive value of 100%.
Conclusion: Infrared thermography of different skin segments provides an accurate tool for predicting failed supraclavicular brachial plexus block. Increased skin temperature at each segment can exclude block failure in the corresponding nerve with 100% accuracy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
