Nizar Hakam, Nassib Abou Heidar, Jose El-Asmar, Mark Khauli, Jad Degheili, Mouhamad Al-Moussawy, Rami Nasr, Albert El-Hajj, Wassim Wazzan, Muhammad Bulbul, Raja B Khauli
{"title":"肾细胞癌部分切除与根治性切除的比较分析:在保留肾单位的高阶段疾病中,肿瘤安全性是否受到损害?","authors":"Nizar Hakam, Nassib Abou Heidar, Jose El-Asmar, Mark Khauli, Jad Degheili, Mouhamad Al-Moussawy, Rami Nasr, Albert El-Hajj, Wassim Wazzan, Muhammad Bulbul, Raja B Khauli","doi":"10.4103/ua.ua_98_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Over the past 20 years, the utility of partial nephrectomy (PN), compared to radical nephrectomy (RN), for the management of localized renal cell carcinoma (RCC) has progressively increased, particularly for larger and more complex masses. We sought to compare the recurrence-free survival (RFS) outcomes of PN versus RN in a single-institution cohort.</p><p><strong>Methods: </strong>Between 2002 and 2017, 228 patients underwent RN or PN for lcT1a-T2b, N0M0 RCC at a single tertiary referral center, performed by five surgeons. The clinical end point result was (local or distant) RFS. Univariate and multivariate (cox regression) models were used to evaluate the association between type of surgery (PN vs. RN) and RFS, in the overall cohort and in a subgroup of patients with cT1b.</p><p><strong>Results: </strong>The median age was 59 (interquartile range [IQR] 48-66), and the median tumor size was 4.5 cm (IQR 3-7). There were 1<b>28</b> PN and 10<b>0</b> RN. Over a median follow-up of 4.2 years (IQR 2.2-6.9), the Kaplan-Meier analysis showed no significant RFS difference between PN and RN (logrank <i>P</i> = 0.53). On multivariate analysis, pathologic stage ≥T2a, Fuhrman Grade ≥3, and chromophobe histology were associated with a worse RFS. PN was not significantly associated with diminished RFS (Hazard ratio [HR] 1.78, 95% confidence interval [CI] 0.74-4.3, <i>P</i> = 0.199) in the overall cohort compared to RN. However, in the cT1b subgroup, PN was associated with a significant increase in recurrence compared to RN (HR = 12.4, 95% CI 1.45-133.4, <i>P</i> = 0.038).</p><p><strong>Conclusions: </strong>Our institutional data highlight the possibility of compromise in RFS for clinically localized RCC treated with PN compared to RN, particularly for larger and more complex masses. These data raise concern, especially in light of the nonproven association of survival benefit of PN over RN, warranting future randomized prospective studies for further evaluation.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"15 2","pages":"226-231"},"PeriodicalIF":0.8000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fd/2c/UA-15-226.PMC10252787.pdf","citationCount":"0","resultStr":"{\"title\":\"Comparative analysis of partial versus radical nephrectomy for renal cell carcinoma: Is oncologic safety compromised during nephron sparing in higher stage disease?\",\"authors\":\"Nizar Hakam, Nassib Abou Heidar, Jose El-Asmar, Mark Khauli, Jad Degheili, Mouhamad Al-Moussawy, Rami Nasr, Albert El-Hajj, Wassim Wazzan, Muhammad Bulbul, Raja B Khauli\",\"doi\":\"10.4103/ua.ua_98_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Over the past 20 years, the utility of partial nephrectomy (PN), compared to radical nephrectomy (RN), for the management of localized renal cell carcinoma (RCC) has progressively increased, particularly for larger and more complex masses. We sought to compare the recurrence-free survival (RFS) outcomes of PN versus RN in a single-institution cohort.</p><p><strong>Methods: </strong>Between 2002 and 2017, 228 patients underwent RN or PN for lcT1a-T2b, N0M0 RCC at a single tertiary referral center, performed by five surgeons. The clinical end point result was (local or distant) RFS. Univariate and multivariate (cox regression) models were used to evaluate the association between type of surgery (PN vs. RN) and RFS, in the overall cohort and in a subgroup of patients with cT1b.</p><p><strong>Results: </strong>The median age was 59 (interquartile range [IQR] 48-66), and the median tumor size was 4.5 cm (IQR 3-7). There were 1<b>28</b> PN and 10<b>0</b> RN. Over a median follow-up of 4.2 years (IQR 2.2-6.9), the Kaplan-Meier analysis showed no significant RFS difference between PN and RN (logrank <i>P</i> = 0.53). On multivariate analysis, pathologic stage ≥T2a, Fuhrman Grade ≥3, and chromophobe histology were associated with a worse RFS. PN was not significantly associated with diminished RFS (Hazard ratio [HR] 1.78, 95% confidence interval [CI] 0.74-4.3, <i>P</i> = 0.199) in the overall cohort compared to RN. However, in the cT1b subgroup, PN was associated with a significant increase in recurrence compared to RN (HR = 12.4, 95% CI 1.45-133.4, <i>P</i> = 0.038).</p><p><strong>Conclusions: </strong>Our institutional data highlight the possibility of compromise in RFS for clinically localized RCC treated with PN compared to RN, particularly for larger and more complex masses. These data raise concern, especially in light of the nonproven association of survival benefit of PN over RN, warranting future randomized prospective studies for further evaluation.</p>\",\"PeriodicalId\":23633,\"journal\":{\"name\":\"Urology Annals\",\"volume\":\"15 2\",\"pages\":\"226-231\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fd/2c/UA-15-226.PMC10252787.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urology Annals\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ua.ua_98_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/2/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_98_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/14 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Comparative analysis of partial versus radical nephrectomy for renal cell carcinoma: Is oncologic safety compromised during nephron sparing in higher stage disease?
Objectives: Over the past 20 years, the utility of partial nephrectomy (PN), compared to radical nephrectomy (RN), for the management of localized renal cell carcinoma (RCC) has progressively increased, particularly for larger and more complex masses. We sought to compare the recurrence-free survival (RFS) outcomes of PN versus RN in a single-institution cohort.
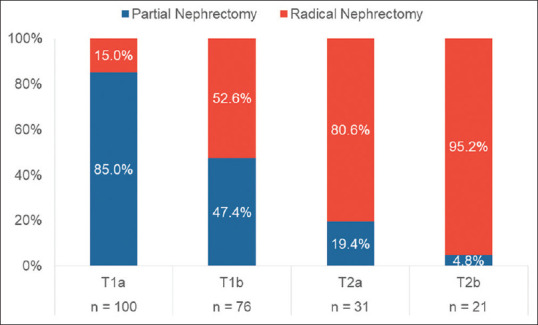
Methods: Between 2002 and 2017, 228 patients underwent RN or PN for lcT1a-T2b, N0M0 RCC at a single tertiary referral center, performed by five surgeons. The clinical end point result was (local or distant) RFS. Univariate and multivariate (cox regression) models were used to evaluate the association between type of surgery (PN vs. RN) and RFS, in the overall cohort and in a subgroup of patients with cT1b.
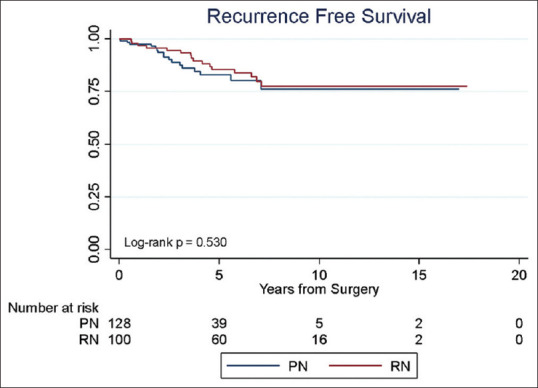
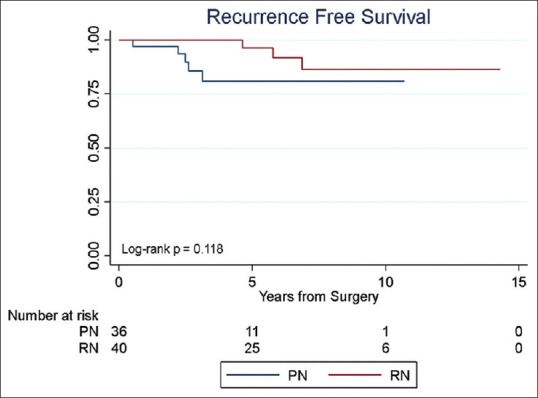
Results: The median age was 59 (interquartile range [IQR] 48-66), and the median tumor size was 4.5 cm (IQR 3-7). There were 128 PN and 100 RN. Over a median follow-up of 4.2 years (IQR 2.2-6.9), the Kaplan-Meier analysis showed no significant RFS difference between PN and RN (logrank P = 0.53). On multivariate analysis, pathologic stage ≥T2a, Fuhrman Grade ≥3, and chromophobe histology were associated with a worse RFS. PN was not significantly associated with diminished RFS (Hazard ratio [HR] 1.78, 95% confidence interval [CI] 0.74-4.3, P = 0.199) in the overall cohort compared to RN. However, in the cT1b subgroup, PN was associated with a significant increase in recurrence compared to RN (HR = 12.4, 95% CI 1.45-133.4, P = 0.038).
Conclusions: Our institutional data highlight the possibility of compromise in RFS for clinically localized RCC treated with PN compared to RN, particularly for larger and more complex masses. These data raise concern, especially in light of the nonproven association of survival benefit of PN over RN, warranting future randomized prospective studies for further evaluation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
