Shinichiro Masuda, Patrick W Serruys, Shigetaka Kageyama, Nozomi Kotoku, Kai Ninomiya, Scot Garg, Alan Soo, Marie-Angele Morel, John D Puskas, Jagat Narula, Ulrich Schneider, Torsten Doenst, Kaoru Tanaka, Johan de Mey, Mark La Meir, Antonio L Bartorelli, Saima Mushtaq, Giulio Pompilio, Daniele Andreini, Yoshinobu Onuma
{"title":"基于SYNTAX评分2020的治疗建议,该评分来源于冠状动脉计算机断层摄影血管造影和有创冠状动脉造影。","authors":"Shinichiro Masuda, Patrick W Serruys, Shigetaka Kageyama, Nozomi Kotoku, Kai Ninomiya, Scot Garg, Alan Soo, Marie-Angele Morel, John D Puskas, Jagat Narula, Ulrich Schneider, Torsten Doenst, Kaoru Tanaka, Johan de Mey, Mark La Meir, Antonio L Bartorelli, Saima Mushtaq, Giulio Pompilio, Daniele Andreini, Yoshinobu Onuma","doi":"10.1007/s10554-023-02884-0","DOIUrl":null,"url":null,"abstract":"<p><p>The diagnostic performance of the SYNTAX score 2020 (SS-2020) when calculated using CCTA remains unknown. This study aimed to compare treatment recommendations based on the SS-2020 derived from coronary computed tomography angiography (CCTA) versus invasive coronary angiography (ICA). This interim analysis included 57 of the planned 114 patients with de-novo three-vessel disease, with or without left main coronary artery disease, enrolled in the ongoing FASTTRACK CABG trial. The anatomical SYNTAX scores derived from ICA or CCTA were evaluated by two separate teams of blinded core-lab analysts. Treatment recommendations were based on a maximal individual absolute risk difference in all-cause mortality between percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) of 4.5% ([predicted PCI mortality] - [predicted CABG mortality]). The level of agreement was evaluated with Bland-Altman plots and Cohen's Kappa. The mean age was 66.2 ± 9.2 years and 89.5% of patients were male. Mean anatomical SYNTAX scores derived from ICA and CCTA were 35.1 ± 11.5 and 35.6 ± 11.4 (p = 0.751), respectively. The Bland-Altman analysis showed mean differences of - 0.26 and - 0.93, with standard deviation of 3.69 and 5.23, for 5- and 10-year all-cause mortality, respectively. The concordance in recommended treatment for 5- and 10-year mortalities were 84.2% (48/57 patients) and 80.7% (46/57 patients), with Cohen's κ coefficients of 0.672 and 0.551. There was moderate to substantial agreement between treatment recommendations based on the SS-2020 derived using CCTA and ICA, suggesting that CCTA could be used as an alternative to ICA when making decisions regarding the modality of revascularization.</p>","PeriodicalId":50332,"journal":{"name":"International Journal of Cardiovascular Imaging","volume":" ","pages":"1795-1804"},"PeriodicalIF":1.5000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10519866/pdf/","citationCount":"1","resultStr":"{\"title\":\"Treatment recommendation based on SYNTAX score 2020 derived from coronary computed tomography angiography and invasive coronary angiography.\",\"authors\":\"Shinichiro Masuda, Patrick W Serruys, Shigetaka Kageyama, Nozomi Kotoku, Kai Ninomiya, Scot Garg, Alan Soo, Marie-Angele Morel, John D Puskas, Jagat Narula, Ulrich Schneider, Torsten Doenst, Kaoru Tanaka, Johan de Mey, Mark La Meir, Antonio L Bartorelli, Saima Mushtaq, Giulio Pompilio, Daniele Andreini, Yoshinobu Onuma\",\"doi\":\"10.1007/s10554-023-02884-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The diagnostic performance of the SYNTAX score 2020 (SS-2020) when calculated using CCTA remains unknown. This study aimed to compare treatment recommendations based on the SS-2020 derived from coronary computed tomography angiography (CCTA) versus invasive coronary angiography (ICA). This interim analysis included 57 of the planned 114 patients with de-novo three-vessel disease, with or without left main coronary artery disease, enrolled in the ongoing FASTTRACK CABG trial. The anatomical SYNTAX scores derived from ICA or CCTA were evaluated by two separate teams of blinded core-lab analysts. Treatment recommendations were based on a maximal individual absolute risk difference in all-cause mortality between percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) of 4.5% ([predicted PCI mortality] - [predicted CABG mortality]). The level of agreement was evaluated with Bland-Altman plots and Cohen's Kappa. The mean age was 66.2 ± 9.2 years and 89.5% of patients were male. Mean anatomical SYNTAX scores derived from ICA and CCTA were 35.1 ± 11.5 and 35.6 ± 11.4 (p = 0.751), respectively. The Bland-Altman analysis showed mean differences of - 0.26 and - 0.93, with standard deviation of 3.69 and 5.23, for 5- and 10-year all-cause mortality, respectively. The concordance in recommended treatment for 5- and 10-year mortalities were 84.2% (48/57 patients) and 80.7% (46/57 patients), with Cohen's κ coefficients of 0.672 and 0.551. There was moderate to substantial agreement between treatment recommendations based on the SS-2020 derived using CCTA and ICA, suggesting that CCTA could be used as an alternative to ICA when making decisions regarding the modality of revascularization.</p>\",\"PeriodicalId\":50332,\"journal\":{\"name\":\"International Journal of Cardiovascular Imaging\",\"volume\":\" \",\"pages\":\"1795-1804\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10519866/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Cardiovascular Imaging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10554-023-02884-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiovascular Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10554-023-02884-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/27 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Treatment recommendation based on SYNTAX score 2020 derived from coronary computed tomography angiography and invasive coronary angiography.
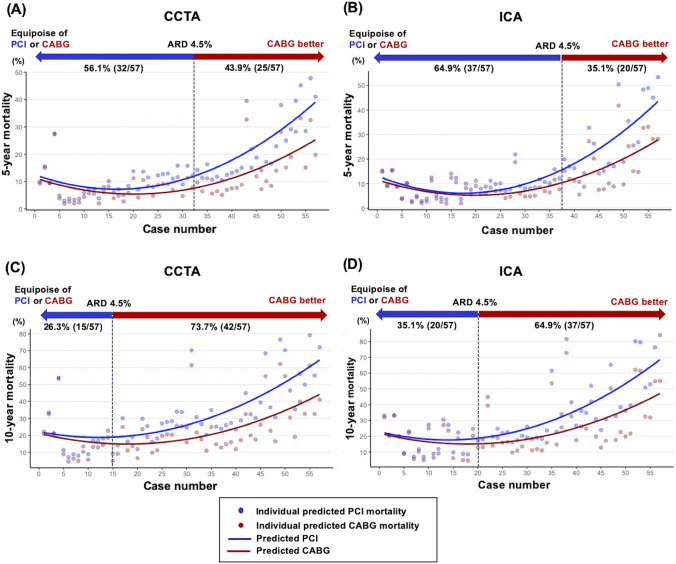
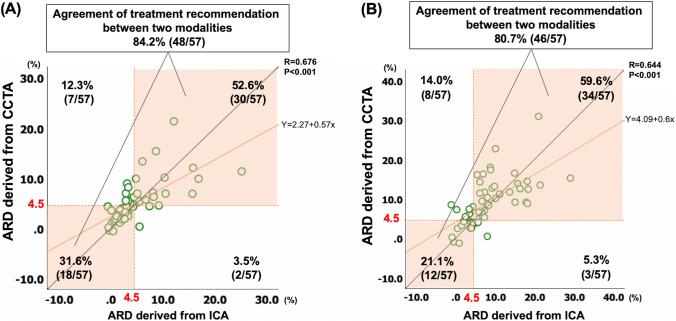
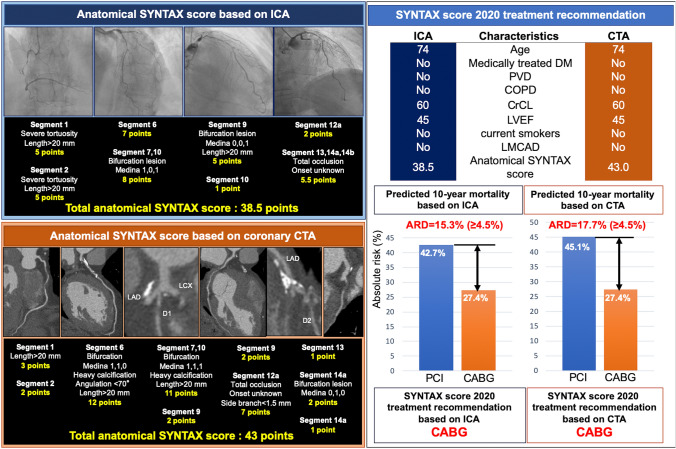
The diagnostic performance of the SYNTAX score 2020 (SS-2020) when calculated using CCTA remains unknown. This study aimed to compare treatment recommendations based on the SS-2020 derived from coronary computed tomography angiography (CCTA) versus invasive coronary angiography (ICA). This interim analysis included 57 of the planned 114 patients with de-novo three-vessel disease, with or without left main coronary artery disease, enrolled in the ongoing FASTTRACK CABG trial. The anatomical SYNTAX scores derived from ICA or CCTA were evaluated by two separate teams of blinded core-lab analysts. Treatment recommendations were based on a maximal individual absolute risk difference in all-cause mortality between percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) of 4.5% ([predicted PCI mortality] - [predicted CABG mortality]). The level of agreement was evaluated with Bland-Altman plots and Cohen's Kappa. The mean age was 66.2 ± 9.2 years and 89.5% of patients were male. Mean anatomical SYNTAX scores derived from ICA and CCTA were 35.1 ± 11.5 and 35.6 ± 11.4 (p = 0.751), respectively. The Bland-Altman analysis showed mean differences of - 0.26 and - 0.93, with standard deviation of 3.69 and 5.23, for 5- and 10-year all-cause mortality, respectively. The concordance in recommended treatment for 5- and 10-year mortalities were 84.2% (48/57 patients) and 80.7% (46/57 patients), with Cohen's κ coefficients of 0.672 and 0.551. There was moderate to substantial agreement between treatment recommendations based on the SS-2020 derived using CCTA and ICA, suggesting that CCTA could be used as an alternative to ICA when making decisions regarding the modality of revascularization.
期刊介绍:
The International Journal of Cardiovascular Imaging publishes technical and clinical communications (original articles, review articles and editorial comments) associated with cardiovascular diseases. The technical communications include the research, development and evaluation of novel imaging methods in the various imaging domains. These domains include magnetic resonance imaging, computed tomography, X-ray imaging, intravascular imaging, and applications in nuclear cardiology and echocardiography, and any combination of these techniques. Of particular interest are topics in medical image processing and image-guided interventions. Clinical applications of such imaging techniques include improved diagnostic approaches, treatment , prognosis and follow-up of cardiovascular patients. Topics include: multi-center or larger individual studies dealing with risk stratification and imaging utilization, applications for better characterization of cardiovascular diseases, and assessment of the efficacy of new drugs and interventional devices.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
