{"title":"富马酸替诺福韦二氧吡酯肾毒性和肾功能恢复的发生率及危险因素:一项医院病例-对照研究","authors":"Sirikan Srisopa, Akarawat Kornjirakasemsan, Pornpit Treebupachatsakul, Paveena Sonthisombat","doi":"10.3947/ic.2023.0001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The incidence of tenofovir disoproxil fumarate (TDF)-induced nephrotoxicity ranges from 15.8 to 19.3 percent. Following cessation of TDF, approximately one-half of patients with nephrotoxicity regained full renal functions. This study aimed to determine the incidence and risk factors for nephrotoxicity, as well as the complete recovery of renal function, in human immunodeficiency virus (HIV)-infected patients receiving TDF regimens.</p><p><strong>Materials and methods: </strong>This was a retrospective case-control study of HIV-positive patients who received TDF regimens from 2 tertiary hospitals between 2012 and 2018. Signs of TDF-induced renal dysfunction, defined as having estimated glomerular filtration rate (eGFR) decline of greater than 25%, and proximal renal tubulopathy (PRT) were followed for 48 months. After discontinuing TDF due to nephrotoxicity, the renal parameters of patients were monitored for 48 months. Univariate and multivariate regression analyses were used to determine the factors associated with TDF-induced nephrotoxicity and renal function recovery.</p><p><strong>Results: </strong>Twelve percent of 3,214 TDF-treated patients were diagnosed with renal dysfunction, whereas 303 patients (15.20%) were diagnosed with PRT. TDF-induced renal dysfunction was associated with older age (odds ratio [OR] = 2.851), smoking (OR = 1.972), and TDF use for more than 3 years (OR 1.928). Receiving trimethoprim-sulfamethoxazole (TMP/SMX) or nonsteroidal anti-inflammatory drugs (NSAIDs) and being elderly were associated with PRT (OR = 4.727, 4.313, and 3.357, respectively). Following the discontinuation of TDF, 12.96% of patients regained full renal function. Elderly patients and those taking renin-angiotensin-aldosterone system (RAAS) inhibitors or protease inhibitors (PIs) had a lower likelihood of full recovery (OR = 0.811, 0.793, 0.582, respectively). One-third experienced PRT recovery, whereas RAAS inhibitors use, old age, and receiving PIs decreased the likelihood of PRT recovery (OR = 0.709, 0.504, 0.311, respectively). TDF cessation at an eGFR greater than 60 mL/min/1.73 m² increased the likelihood of renal function recovery and PRT by 4.07 and 2.11 times, respectively.</p><p><strong>Conclusion: </strong>Twelve percent and 15 percent of patients receiving TDF developed renal dysfunction and PRT, respectively. Age, TMP/SMX, NSAIDs, and long-term TDF exposure were independent risk factors for TDF-induced nephrotoxicity. Thirteen and thirty-three percent of patients with renal dysfunction and PRT recovered from their conditions, respectively. The discontinuation of TDF at an eGFR greater than 60 mL/min/1.73 m² was advantageous for the recovery of renal function and PRT.</p>","PeriodicalId":51616,"journal":{"name":"Infection and Chemotherapy","volume":"55 2","pages":"226-236"},"PeriodicalIF":2.9000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/de/ic-55-226.PMC10323539.pdf","citationCount":"1","resultStr":"{\"title\":\"Incidence and Risk Factors of Tenofovir Disoproxil Fumarate Induced Nephrotoxicity and Renal Function Recovery, a Hospital Case-Control Study.\",\"authors\":\"Sirikan Srisopa, Akarawat Kornjirakasemsan, Pornpit Treebupachatsakul, Paveena Sonthisombat\",\"doi\":\"10.3947/ic.2023.0001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The incidence of tenofovir disoproxil fumarate (TDF)-induced nephrotoxicity ranges from 15.8 to 19.3 percent. Following cessation of TDF, approximately one-half of patients with nephrotoxicity regained full renal functions. This study aimed to determine the incidence and risk factors for nephrotoxicity, as well as the complete recovery of renal function, in human immunodeficiency virus (HIV)-infected patients receiving TDF regimens.</p><p><strong>Materials and methods: </strong>This was a retrospective case-control study of HIV-positive patients who received TDF regimens from 2 tertiary hospitals between 2012 and 2018. Signs of TDF-induced renal dysfunction, defined as having estimated glomerular filtration rate (eGFR) decline of greater than 25%, and proximal renal tubulopathy (PRT) were followed for 48 months. After discontinuing TDF due to nephrotoxicity, the renal parameters of patients were monitored for 48 months. Univariate and multivariate regression analyses were used to determine the factors associated with TDF-induced nephrotoxicity and renal function recovery.</p><p><strong>Results: </strong>Twelve percent of 3,214 TDF-treated patients were diagnosed with renal dysfunction, whereas 303 patients (15.20%) were diagnosed with PRT. TDF-induced renal dysfunction was associated with older age (odds ratio [OR] = 2.851), smoking (OR = 1.972), and TDF use for more than 3 years (OR 1.928). Receiving trimethoprim-sulfamethoxazole (TMP/SMX) or nonsteroidal anti-inflammatory drugs (NSAIDs) and being elderly were associated with PRT (OR = 4.727, 4.313, and 3.357, respectively). Following the discontinuation of TDF, 12.96% of patients regained full renal function. Elderly patients and those taking renin-angiotensin-aldosterone system (RAAS) inhibitors or protease inhibitors (PIs) had a lower likelihood of full recovery (OR = 0.811, 0.793, 0.582, respectively). One-third experienced PRT recovery, whereas RAAS inhibitors use, old age, and receiving PIs decreased the likelihood of PRT recovery (OR = 0.709, 0.504, 0.311, respectively). TDF cessation at an eGFR greater than 60 mL/min/1.73 m² increased the likelihood of renal function recovery and PRT by 4.07 and 2.11 times, respectively.</p><p><strong>Conclusion: </strong>Twelve percent and 15 percent of patients receiving TDF developed renal dysfunction and PRT, respectively. Age, TMP/SMX, NSAIDs, and long-term TDF exposure were independent risk factors for TDF-induced nephrotoxicity. Thirteen and thirty-three percent of patients with renal dysfunction and PRT recovered from their conditions, respectively. The discontinuation of TDF at an eGFR greater than 60 mL/min/1.73 m² was advantageous for the recovery of renal function and PRT.</p>\",\"PeriodicalId\":51616,\"journal\":{\"name\":\"Infection and Chemotherapy\",\"volume\":\"55 2\",\"pages\":\"226-236\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/de/ic-55-226.PMC10323539.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infection and Chemotherapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3947/ic.2023.0001\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection and Chemotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3947/ic.2023.0001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Incidence and Risk Factors of Tenofovir Disoproxil Fumarate Induced Nephrotoxicity and Renal Function Recovery, a Hospital Case-Control Study.
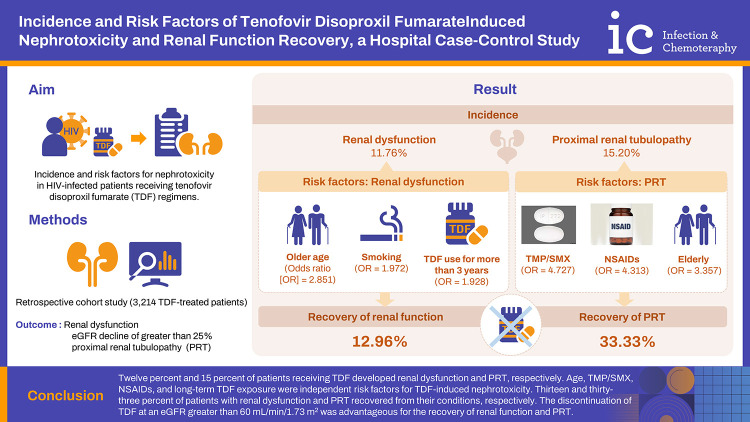
Background: The incidence of tenofovir disoproxil fumarate (TDF)-induced nephrotoxicity ranges from 15.8 to 19.3 percent. Following cessation of TDF, approximately one-half of patients with nephrotoxicity regained full renal functions. This study aimed to determine the incidence and risk factors for nephrotoxicity, as well as the complete recovery of renal function, in human immunodeficiency virus (HIV)-infected patients receiving TDF regimens.
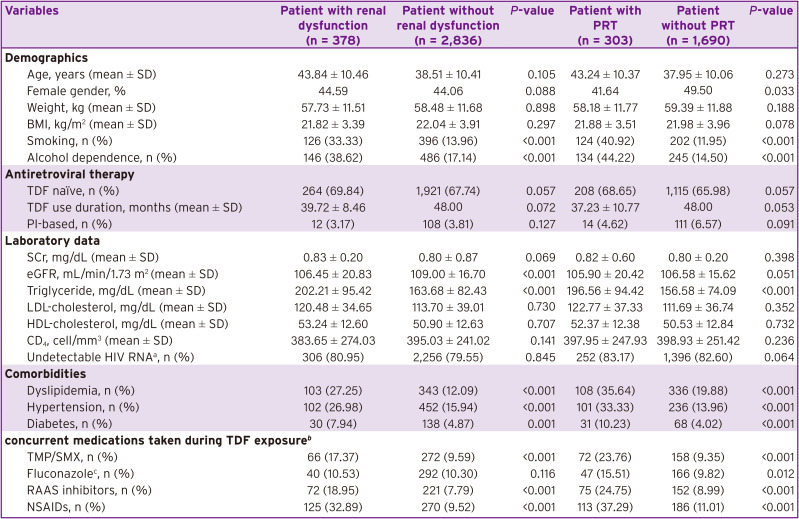
Materials and methods: This was a retrospective case-control study of HIV-positive patients who received TDF regimens from 2 tertiary hospitals between 2012 and 2018. Signs of TDF-induced renal dysfunction, defined as having estimated glomerular filtration rate (eGFR) decline of greater than 25%, and proximal renal tubulopathy (PRT) were followed for 48 months. After discontinuing TDF due to nephrotoxicity, the renal parameters of patients were monitored for 48 months. Univariate and multivariate regression analyses were used to determine the factors associated with TDF-induced nephrotoxicity and renal function recovery.
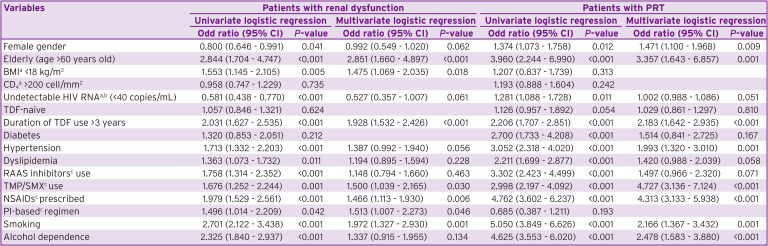
Results: Twelve percent of 3,214 TDF-treated patients were diagnosed with renal dysfunction, whereas 303 patients (15.20%) were diagnosed with PRT. TDF-induced renal dysfunction was associated with older age (odds ratio [OR] = 2.851), smoking (OR = 1.972), and TDF use for more than 3 years (OR 1.928). Receiving trimethoprim-sulfamethoxazole (TMP/SMX) or nonsteroidal anti-inflammatory drugs (NSAIDs) and being elderly were associated with PRT (OR = 4.727, 4.313, and 3.357, respectively). Following the discontinuation of TDF, 12.96% of patients regained full renal function. Elderly patients and those taking renin-angiotensin-aldosterone system (RAAS) inhibitors or protease inhibitors (PIs) had a lower likelihood of full recovery (OR = 0.811, 0.793, 0.582, respectively). One-third experienced PRT recovery, whereas RAAS inhibitors use, old age, and receiving PIs decreased the likelihood of PRT recovery (OR = 0.709, 0.504, 0.311, respectively). TDF cessation at an eGFR greater than 60 mL/min/1.73 m² increased the likelihood of renal function recovery and PRT by 4.07 and 2.11 times, respectively.
Conclusion: Twelve percent and 15 percent of patients receiving TDF developed renal dysfunction and PRT, respectively. Age, TMP/SMX, NSAIDs, and long-term TDF exposure were independent risk factors for TDF-induced nephrotoxicity. Thirteen and thirty-three percent of patients with renal dysfunction and PRT recovered from their conditions, respectively. The discontinuation of TDF at an eGFR greater than 60 mL/min/1.73 m² was advantageous for the recovery of renal function and PRT.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
