Ioannis D Kostakis, Nikolaos Dimitrokallis, Satheesh Iype
{"title":"米兰标准范围内肝硬化肝细胞癌患者肝移植前桥接局部治疗:一项系统综述和荟萃分析。","authors":"Ioannis D Kostakis, Nikolaos Dimitrokallis, Satheesh Iype","doi":"10.20524/aog.2023.0812","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We performed a meta-analysis to assess the benefit of bridging locoregional treatment (LRT) before liver transplantation for cirrhotic patients with hepatocellular carcinoma (HCC) already within the Milan criteria at diagnosis.</p><p><strong>Methods: </strong>We included original studies with HCC cases within the Milan criteria at diagnosis, comparing patients with and without bridging LRT before liver transplantation.</p><p><strong>Results: </strong>Twenty-six retrospective original studies were included. Out of the 9068 patients within the Milan criteria, 6435 (71%) received bridging LRT and 2633 (29%) did not. The most frequent LRTs were transarterial chemoembolization, radiofrequency ablation, and microwave ablation. Most of the patient and tumor characteristics were similar between the 2 groups. Maximum tumor diameter on scans was slightly larger in the LRT arm (mean difference: 0.36 cm, 95% confidence interval [CI] 0.11-0.61; <i>I</i><sup>2</sup>=79%). The LRT group also had multifocal disease slightly more frequently (risk ratio [RR] 1.21, 95%CI 1.04-1.41; <i>I</i><sup>2</sup>=0%) and disease extent outside the Milan criteria (RR 1.3, 95%CI 1.03-1.66; <i>I</i><sup>2</sup>=0%) on pathological examination of explanted livers. There was no difference between the 2 arms in the waiting time for transplant, dropout rates, disease-free survival at 1, 3, 5 years after transplant, or overall survival at 3 and 5 years after transplant. However, cases with LRT had better overall survival at 1 year after transplant (hazard ratio 0.54, 95%CI 0.35-0.86; <i>I</i><sup>2</sup>=0%).</p><p><strong>Conclusions: </strong>The precise benefit of bridging LRT for cirrhotic patients with HCC within the Milan criteria at diagnosis is unclear. There may be an advantage regarding short-term overall survival after liver transplantation.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"36 4","pages":"449-458"},"PeriodicalIF":2.2000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/9d/AnnGastroenterol-36-449.PMC10304529.pdf","citationCount":"0","resultStr":"{\"title\":\"Bridging locoregional treatment prior to liver transplantation for cirrhotic patients with hepatocellular carcinoma within the Milan criteria: a systematic review and meta-analysis.\",\"authors\":\"Ioannis D Kostakis, Nikolaos Dimitrokallis, Satheesh Iype\",\"doi\":\"10.20524/aog.2023.0812\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We performed a meta-analysis to assess the benefit of bridging locoregional treatment (LRT) before liver transplantation for cirrhotic patients with hepatocellular carcinoma (HCC) already within the Milan criteria at diagnosis.</p><p><strong>Methods: </strong>We included original studies with HCC cases within the Milan criteria at diagnosis, comparing patients with and without bridging LRT before liver transplantation.</p><p><strong>Results: </strong>Twenty-six retrospective original studies were included. Out of the 9068 patients within the Milan criteria, 6435 (71%) received bridging LRT and 2633 (29%) did not. The most frequent LRTs were transarterial chemoembolization, radiofrequency ablation, and microwave ablation. Most of the patient and tumor characteristics were similar between the 2 groups. Maximum tumor diameter on scans was slightly larger in the LRT arm (mean difference: 0.36 cm, 95% confidence interval [CI] 0.11-0.61; <i>I</i><sup>2</sup>=79%). The LRT group also had multifocal disease slightly more frequently (risk ratio [RR] 1.21, 95%CI 1.04-1.41; <i>I</i><sup>2</sup>=0%) and disease extent outside the Milan criteria (RR 1.3, 95%CI 1.03-1.66; <i>I</i><sup>2</sup>=0%) on pathological examination of explanted livers. There was no difference between the 2 arms in the waiting time for transplant, dropout rates, disease-free survival at 1, 3, 5 years after transplant, or overall survival at 3 and 5 years after transplant. However, cases with LRT had better overall survival at 1 year after transplant (hazard ratio 0.54, 95%CI 0.35-0.86; <i>I</i><sup>2</sup>=0%).</p><p><strong>Conclusions: </strong>The precise benefit of bridging LRT for cirrhotic patients with HCC within the Milan criteria at diagnosis is unclear. There may be an advantage regarding short-term overall survival after liver transplantation.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"36 4\",\"pages\":\"449-458\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/9d/AnnGastroenterol-36-449.PMC10304529.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2023.0812\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2023.0812","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Bridging locoregional treatment prior to liver transplantation for cirrhotic patients with hepatocellular carcinoma within the Milan criteria: a systematic review and meta-analysis.
Background: We performed a meta-analysis to assess the benefit of bridging locoregional treatment (LRT) before liver transplantation for cirrhotic patients with hepatocellular carcinoma (HCC) already within the Milan criteria at diagnosis.
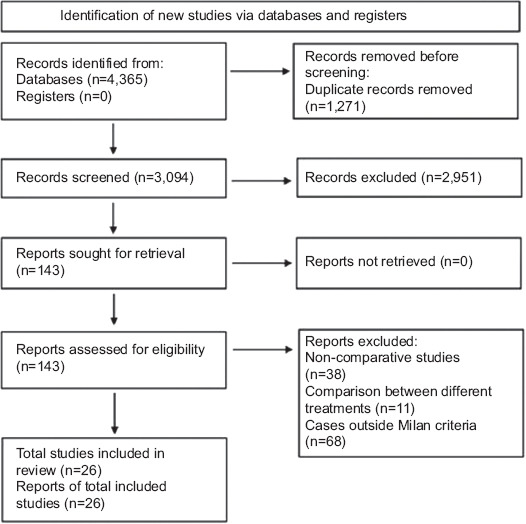
Methods: We included original studies with HCC cases within the Milan criteria at diagnosis, comparing patients with and without bridging LRT before liver transplantation.
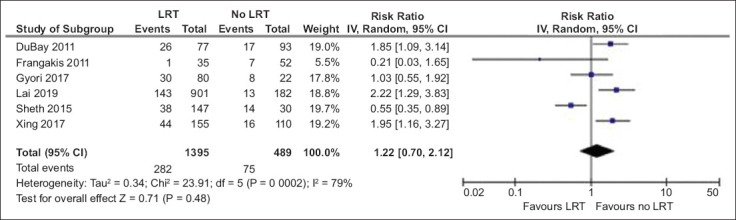
Results: Twenty-six retrospective original studies were included. Out of the 9068 patients within the Milan criteria, 6435 (71%) received bridging LRT and 2633 (29%) did not. The most frequent LRTs were transarterial chemoembolization, radiofrequency ablation, and microwave ablation. Most of the patient and tumor characteristics were similar between the 2 groups. Maximum tumor diameter on scans was slightly larger in the LRT arm (mean difference: 0.36 cm, 95% confidence interval [CI] 0.11-0.61; I2=79%). The LRT group also had multifocal disease slightly more frequently (risk ratio [RR] 1.21, 95%CI 1.04-1.41; I2=0%) and disease extent outside the Milan criteria (RR 1.3, 95%CI 1.03-1.66; I2=0%) on pathological examination of explanted livers. There was no difference between the 2 arms in the waiting time for transplant, dropout rates, disease-free survival at 1, 3, 5 years after transplant, or overall survival at 3 and 5 years after transplant. However, cases with LRT had better overall survival at 1 year after transplant (hazard ratio 0.54, 95%CI 0.35-0.86; I2=0%).
Conclusions: The precise benefit of bridging LRT for cirrhotic patients with HCC within the Milan criteria at diagnosis is unclear. There may be an advantage regarding short-term overall survival after liver transplantation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
