{"title":"Leuprolide治疗后乳腺癌患者垂体卒中1例报告。","authors":"Jungbin Lee, Sun-Chul Hwang, Sung-Tae Park","doi":"10.14791/btrt.2023.0006","DOIUrl":null,"url":null,"abstract":"<p><p>Pituitary apoplexy (PA) is a clinical syndrome resulting from sudden hemorrhage and/or infarction of the pituitary gland. Recent reports documented the development of PA secondary to treatment with gonadotropin-releasing hormone (GnRH) agonists for prostate cancer. A 52-year-old woman visited our emergency room with a severe headache, occurred 1 day prior. She underwent breast-conserving surgery for breast cancer 1 month prior. She was currently undergoing radiation and hormone therapy, consisting of leuprorelin. Brain contrast-enhanced MRI revealed a pituitary adenoma with internal hemorrhage in the sellar and suprasellar areas. Pachymeningeal enhancement was observed along the retroclival and bilateral frontal areas. The patient was diagnosed with PA and aseptic meningitis. The patient underwent total excision via transsphenoidal surgery 8 days after admission. The patient was pathologically diagnosed with a pituitary adenoma with necrosis. On immunochemical staining, the tumor was positive for follicle-stimulating hormone. The follow-up MRI revealed no evidence of residual tumor or an improved pachymeningeal enhancement. She is currently undergoing follow-up at the neurosurgery and endocrinology outpatient departments with no noted complications. In breast cancer patients receiving GnRH agonist therapy, PA may be rare complication.</p>","PeriodicalId":72453,"journal":{"name":"Brain tumor research and treatment","volume":"11 2","pages":"153-157"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d0/16/btrt-11-153.PMC10172007.pdf","citationCount":"0","resultStr":"{\"title\":\"Pituitary Apoplexy After Leuprolide Therapy in a Breast Cancer Patient: A Case Report.\",\"authors\":\"Jungbin Lee, Sun-Chul Hwang, Sung-Tae Park\",\"doi\":\"10.14791/btrt.2023.0006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Pituitary apoplexy (PA) is a clinical syndrome resulting from sudden hemorrhage and/or infarction of the pituitary gland. Recent reports documented the development of PA secondary to treatment with gonadotropin-releasing hormone (GnRH) agonists for prostate cancer. A 52-year-old woman visited our emergency room with a severe headache, occurred 1 day prior. She underwent breast-conserving surgery for breast cancer 1 month prior. She was currently undergoing radiation and hormone therapy, consisting of leuprorelin. Brain contrast-enhanced MRI revealed a pituitary adenoma with internal hemorrhage in the sellar and suprasellar areas. Pachymeningeal enhancement was observed along the retroclival and bilateral frontal areas. The patient was diagnosed with PA and aseptic meningitis. The patient underwent total excision via transsphenoidal surgery 8 days after admission. The patient was pathologically diagnosed with a pituitary adenoma with necrosis. On immunochemical staining, the tumor was positive for follicle-stimulating hormone. The follow-up MRI revealed no evidence of residual tumor or an improved pachymeningeal enhancement. She is currently undergoing follow-up at the neurosurgery and endocrinology outpatient departments with no noted complications. In breast cancer patients receiving GnRH agonist therapy, PA may be rare complication.</p>\",\"PeriodicalId\":72453,\"journal\":{\"name\":\"Brain tumor research and treatment\",\"volume\":\"11 2\",\"pages\":\"153-157\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d0/16/btrt-11-153.PMC10172007.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain tumor research and treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14791/btrt.2023.0006\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain tumor research and treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14791/btrt.2023.0006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Pituitary Apoplexy After Leuprolide Therapy in a Breast Cancer Patient: A Case Report.
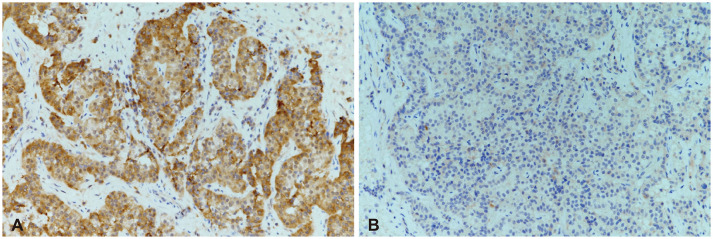
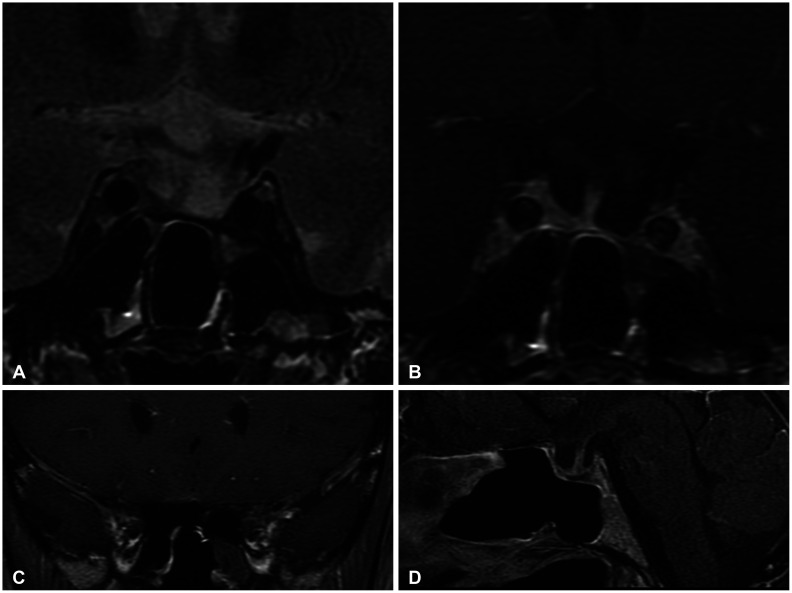
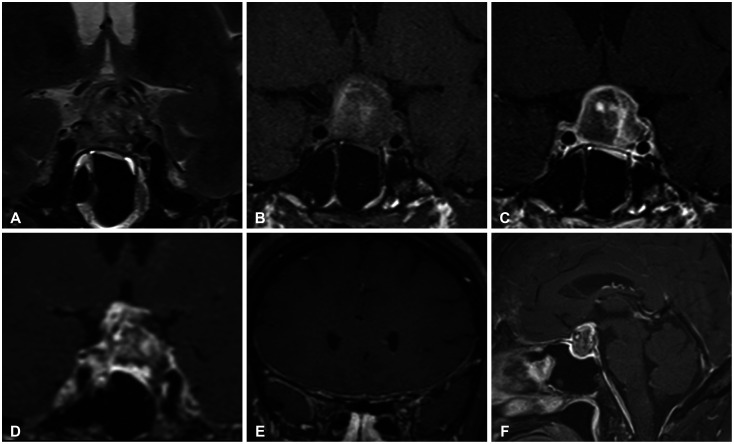
Pituitary apoplexy (PA) is a clinical syndrome resulting from sudden hemorrhage and/or infarction of the pituitary gland. Recent reports documented the development of PA secondary to treatment with gonadotropin-releasing hormone (GnRH) agonists for prostate cancer. A 52-year-old woman visited our emergency room with a severe headache, occurred 1 day prior. She underwent breast-conserving surgery for breast cancer 1 month prior. She was currently undergoing radiation and hormone therapy, consisting of leuprorelin. Brain contrast-enhanced MRI revealed a pituitary adenoma with internal hemorrhage in the sellar and suprasellar areas. Pachymeningeal enhancement was observed along the retroclival and bilateral frontal areas. The patient was diagnosed with PA and aseptic meningitis. The patient underwent total excision via transsphenoidal surgery 8 days after admission. The patient was pathologically diagnosed with a pituitary adenoma with necrosis. On immunochemical staining, the tumor was positive for follicle-stimulating hormone. The follow-up MRI revealed no evidence of residual tumor or an improved pachymeningeal enhancement. She is currently undergoing follow-up at the neurosurgery and endocrinology outpatient departments with no noted complications. In breast cancer patients receiving GnRH agonist therapy, PA may be rare complication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
