Naoya Nagaya , Kevin J. Chua , Joshua Sterling , Shigeo Horie , Isaac Y. Kim
{"title":"延长与标准盆腔淋巴结清扫术的3年生化复发率无差异","authors":"Naoya Nagaya , Kevin J. Chua , Joshua Sterling , Shigeo Horie , Isaac Y. Kim","doi":"10.1016/j.prnil.2022.12.005","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>extended pelvic lymph node dissection (ePLND) increases the detection rate of lymph node positive prostate cancer compared to a standard pelvic lymph node dissection (sPLND). However, improvement of patient outcomes remains questionable. Here we report and compare 3-year postoperative PSA recurrence rates between patients that underwent sPLND versus ePLND at the time of prostatectomy.</p></div><div><h3>Methods</h3><p>162 patients received a sPLND (which involvedremoval of periprostatic, external iliac, and obturator lymph nodes bilaterally), and 142 patients received an ePLND (which involved removal of periprostatic, external iliac, obturator, hypogastric, and common iliac nodes bilaterally). Decision to undergo ePLND versus sPLND at our institution was changed in 2016 based on the National Comprehensive Cancer Network guideline. The median follow-up time was 7 and 3 years for sPLND and ePLND patients, respectively. All node-positive patients were offered adjuvant radiotherapy. Kaplan–Meier analysis was carried out to assess the impact of a PLND on early postoperative PSA progression-free survival. Subgroup analyses were done for node-negative and node-positive patients, as well as Gleason score.</p></div><div><h3>Results</h3><p>Gleason score and T stage were not significantly different between patients who received an ePLND and sPLND. The pN1 rate for ePLND and sPLND were 20% (28/142) and 6% (10/162), respectively. There was no difference in the use of adjuvant treatments in the pN0 patients. Significantly, more ePLND pN1 patients received adjuvant androgen deprivation therapy (25/28 vs. 5/10 <em>P</em> = 0.012) and radiation (27/28 vs. 4/10 <em>P</em> = 0.002). Yet, no difference in biochemical recurrence between ePLND and sPLND was observed (<em>P</em> = 0.44). This remained true in subgroup analyses of node-positive (<em>P</em> = 0.26), node-negative (<em>P</em> = 0.78), Gleason Score 6–7 (<em>P</em> = 0.51), and Gleason Score 8–10 (<em>P</em> = 0.77).</p></div><div><h3>Conclusions</h3><p>PLND provided no additional therapeutic benefit, even though ePLND patients were significantly more likely to have node-positive disease and undergo adjuvant treatment, compared to a sPLND.</p></div>","PeriodicalId":20845,"journal":{"name":"Prostate International","volume":"11 2","pages":"Pages 107-112"},"PeriodicalIF":2.6000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b8/dd/main.PMC10318318.pdf","citationCount":"0","resultStr":"{\"title\":\"Extended versus standard pelvic lymph node dissection yields no difference in 3-year biochemical recurrence rates\",\"authors\":\"Naoya Nagaya , Kevin J. Chua , Joshua Sterling , Shigeo Horie , Isaac Y. Kim\",\"doi\":\"10.1016/j.prnil.2022.12.005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>extended pelvic lymph node dissection (ePLND) increases the detection rate of lymph node positive prostate cancer compared to a standard pelvic lymph node dissection (sPLND). However, improvement of patient outcomes remains questionable. Here we report and compare 3-year postoperative PSA recurrence rates between patients that underwent sPLND versus ePLND at the time of prostatectomy.</p></div><div><h3>Methods</h3><p>162 patients received a sPLND (which involvedremoval of periprostatic, external iliac, and obturator lymph nodes bilaterally), and 142 patients received an ePLND (which involved removal of periprostatic, external iliac, obturator, hypogastric, and common iliac nodes bilaterally). Decision to undergo ePLND versus sPLND at our institution was changed in 2016 based on the National Comprehensive Cancer Network guideline. The median follow-up time was 7 and 3 years for sPLND and ePLND patients, respectively. All node-positive patients were offered adjuvant radiotherapy. Kaplan–Meier analysis was carried out to assess the impact of a PLND on early postoperative PSA progression-free survival. Subgroup analyses were done for node-negative and node-positive patients, as well as Gleason score.</p></div><div><h3>Results</h3><p>Gleason score and T stage were not significantly different between patients who received an ePLND and sPLND. The pN1 rate for ePLND and sPLND were 20% (28/142) and 6% (10/162), respectively. There was no difference in the use of adjuvant treatments in the pN0 patients. Significantly, more ePLND pN1 patients received adjuvant androgen deprivation therapy (25/28 vs. 5/10 <em>P</em> = 0.012) and radiation (27/28 vs. 4/10 <em>P</em> = 0.002). Yet, no difference in biochemical recurrence between ePLND and sPLND was observed (<em>P</em> = 0.44). This remained true in subgroup analyses of node-positive (<em>P</em> = 0.26), node-negative (<em>P</em> = 0.78), Gleason Score 6–7 (<em>P</em> = 0.51), and Gleason Score 8–10 (<em>P</em> = 0.77).</p></div><div><h3>Conclusions</h3><p>PLND provided no additional therapeutic benefit, even though ePLND patients were significantly more likely to have node-positive disease and undergo adjuvant treatment, compared to a sPLND.</p></div>\",\"PeriodicalId\":20845,\"journal\":{\"name\":\"Prostate International\",\"volume\":\"11 2\",\"pages\":\"Pages 107-112\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b8/dd/main.PMC10318318.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Prostate International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2287888222000812\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/12/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate International","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2287888222000812","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Extended versus standard pelvic lymph node dissection yields no difference in 3-year biochemical recurrence rates
Background
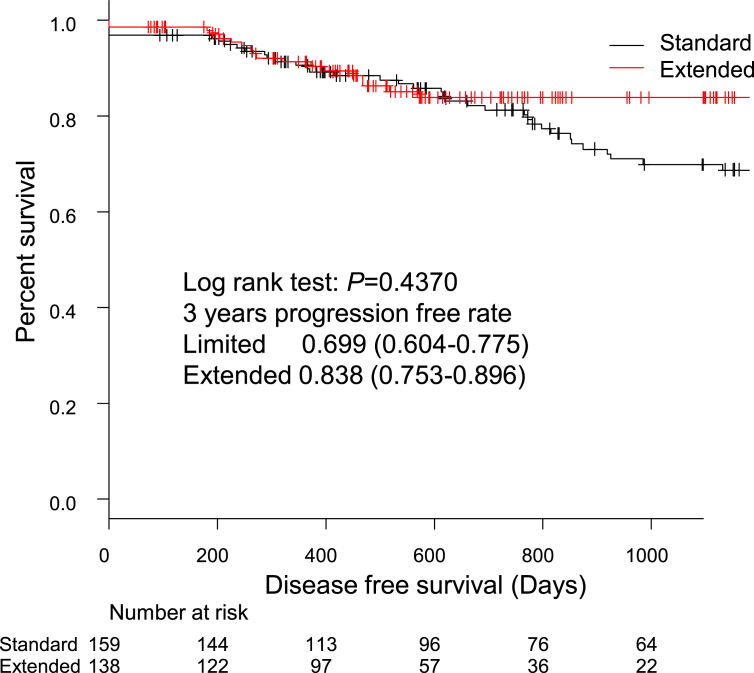
extended pelvic lymph node dissection (ePLND) increases the detection rate of lymph node positive prostate cancer compared to a standard pelvic lymph node dissection (sPLND). However, improvement of patient outcomes remains questionable. Here we report and compare 3-year postoperative PSA recurrence rates between patients that underwent sPLND versus ePLND at the time of prostatectomy.
Methods
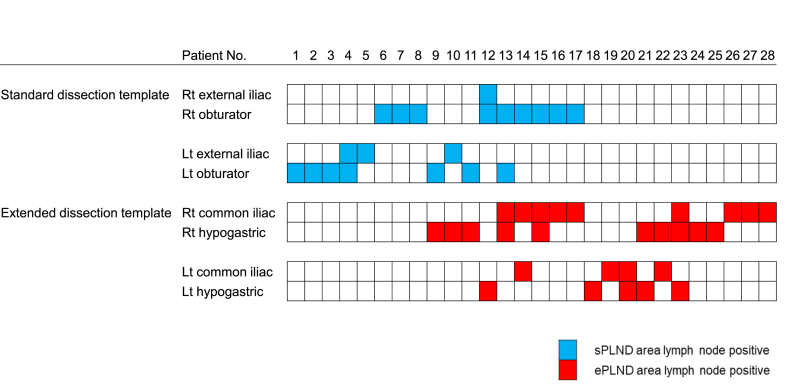
162 patients received a sPLND (which involvedremoval of periprostatic, external iliac, and obturator lymph nodes bilaterally), and 142 patients received an ePLND (which involved removal of periprostatic, external iliac, obturator, hypogastric, and common iliac nodes bilaterally). Decision to undergo ePLND versus sPLND at our institution was changed in 2016 based on the National Comprehensive Cancer Network guideline. The median follow-up time was 7 and 3 years for sPLND and ePLND patients, respectively. All node-positive patients were offered adjuvant radiotherapy. Kaplan–Meier analysis was carried out to assess the impact of a PLND on early postoperative PSA progression-free survival. Subgroup analyses were done for node-negative and node-positive patients, as well as Gleason score.
Results
Gleason score and T stage were not significantly different between patients who received an ePLND and sPLND. The pN1 rate for ePLND and sPLND were 20% (28/142) and 6% (10/162), respectively. There was no difference in the use of adjuvant treatments in the pN0 patients. Significantly, more ePLND pN1 patients received adjuvant androgen deprivation therapy (25/28 vs. 5/10 P = 0.012) and radiation (27/28 vs. 4/10 P = 0.002). Yet, no difference in biochemical recurrence between ePLND and sPLND was observed (P = 0.44). This remained true in subgroup analyses of node-positive (P = 0.26), node-negative (P = 0.78), Gleason Score 6–7 (P = 0.51), and Gleason Score 8–10 (P = 0.77).
Conclusions
PLND provided no additional therapeutic benefit, even though ePLND patients were significantly more likely to have node-positive disease and undergo adjuvant treatment, compared to a sPLND.
期刊介绍:
Prostate International (Prostate Int, PI), the official English-language journal of Asian Pacific Prostate Society (APPS), is an international peer-reviewed academic journal dedicated to basic and clinical studies on prostate cancer, benign prostatic hyperplasia, prostatitis, and ...




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
