Kristóf Levente Korpás, Lívia Beke, Dániel Varga, László Bidiga, Gábor Méhes, Sarolta Molnár
{"title":"通过广泛的前列腺活检取样可以提高分级组的准确性,但与前列腺切除术标本取样或免疫组织化学的使用无关。","authors":"Kristóf Levente Korpás, Lívia Beke, Dániel Varga, László Bidiga, Gábor Méhes, Sarolta Molnár","doi":"10.3389/pore.2023.1611157","DOIUrl":null,"url":null,"abstract":"<p><p>Assessing the accurate Grade Group of a prostate needle biopsy specimen is essential for choosing the adequate therapeutic modality for prostate cancer patients. However, it is well-known that biopsy Grade Group tends to up- or downgrade significantly at radical prostatectomy. We aimed to investigate the correlation between accuracy and biopsy core number, performed immunohistochemical staining (IHC) or prostatectomy specimen sampling, with the latest also being correlated with higher detection rates of adverse pathological features, e.g., positive surgical margins, higher pathological stage or presence of perineural invasion (PnI status). The study cohort consisted of 315 consecutive patients diagnosed with prostate adenocarcinoma via transrectal ultrasound-guided needle biopsy who later underwent radical prostatectomy. We grouped and compared patients based on Grade Group accuracy, presence of IHC on biopsy, margin status, pathological stage, and PnI status. Inter-observer reproducibility was also calculated. Statistical analyzes included ANOVA, Tukey's multiple comparisons <i>post hoc</i> test, Chi-squared test, and Fleiss kappa statistics. Undergraded cases harboured a significantly lower number of biopsy cores (<i>p</i> < 0.05), than accurately graded cases. Using IHC did not affect grading accuracy significantly, nor did the number of slides from prostatectomy specimens. The mean number of slides was virtually identical when margin status, pathological stage and PnI status of prostatectomy specimens were compared. Inter-observer reproducibility at our institute was calculated as fair (overall kappa = 0.29). Grade Group accuracy is significantly improved by obtaining more cores at biopsy but is unrelated to performed IHC. The extent of sampling prostatectomy specimens, however, did not affect accuracy and failed to significantly improve detection of adverse pathological features.</p>","PeriodicalId":19981,"journal":{"name":"Pathology & Oncology Research","volume":"29 ","pages":"1611157"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10319996/pdf/","citationCount":"0","resultStr":"{\"title\":\"Grade Group accuracy is improved by extensive prostate biopsy sampling, but unrelated to prostatectomy specimen sampling or use of immunohistochemistry.\",\"authors\":\"Kristóf Levente Korpás, Lívia Beke, Dániel Varga, László Bidiga, Gábor Méhes, Sarolta Molnár\",\"doi\":\"10.3389/pore.2023.1611157\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Assessing the accurate Grade Group of a prostate needle biopsy specimen is essential for choosing the adequate therapeutic modality for prostate cancer patients. However, it is well-known that biopsy Grade Group tends to up- or downgrade significantly at radical prostatectomy. We aimed to investigate the correlation between accuracy and biopsy core number, performed immunohistochemical staining (IHC) or prostatectomy specimen sampling, with the latest also being correlated with higher detection rates of adverse pathological features, e.g., positive surgical margins, higher pathological stage or presence of perineural invasion (PnI status). The study cohort consisted of 315 consecutive patients diagnosed with prostate adenocarcinoma via transrectal ultrasound-guided needle biopsy who later underwent radical prostatectomy. We grouped and compared patients based on Grade Group accuracy, presence of IHC on biopsy, margin status, pathological stage, and PnI status. Inter-observer reproducibility was also calculated. Statistical analyzes included ANOVA, Tukey's multiple comparisons <i>post hoc</i> test, Chi-squared test, and Fleiss kappa statistics. Undergraded cases harboured a significantly lower number of biopsy cores (<i>p</i> < 0.05), than accurately graded cases. Using IHC did not affect grading accuracy significantly, nor did the number of slides from prostatectomy specimens. The mean number of slides was virtually identical when margin status, pathological stage and PnI status of prostatectomy specimens were compared. Inter-observer reproducibility at our institute was calculated as fair (overall kappa = 0.29). Grade Group accuracy is significantly improved by obtaining more cores at biopsy but is unrelated to performed IHC. The extent of sampling prostatectomy specimens, however, did not affect accuracy and failed to significantly improve detection of adverse pathological features.</p>\",\"PeriodicalId\":19981,\"journal\":{\"name\":\"Pathology & Oncology Research\",\"volume\":\"29 \",\"pages\":\"1611157\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10319996/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pathology & Oncology Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/pore.2023.1611157\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pathology & Oncology Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/pore.2023.1611157","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Grade Group accuracy is improved by extensive prostate biopsy sampling, but unrelated to prostatectomy specimen sampling or use of immunohistochemistry.
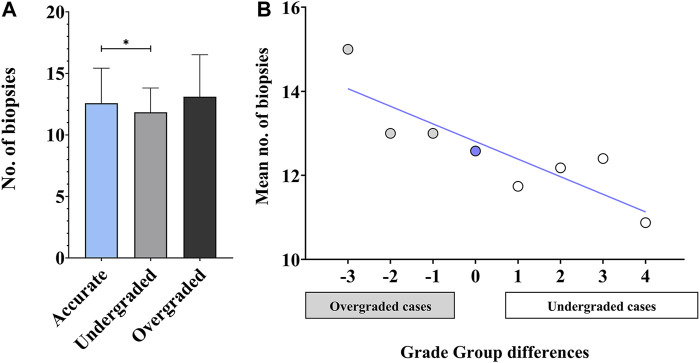
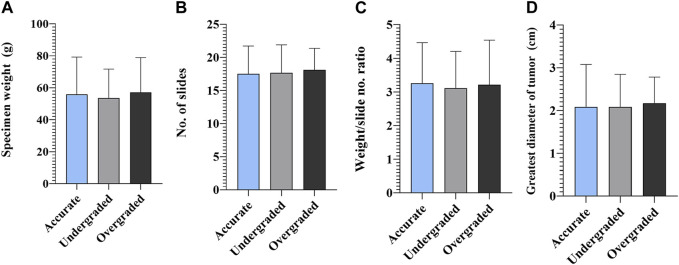
Assessing the accurate Grade Group of a prostate needle biopsy specimen is essential for choosing the adequate therapeutic modality for prostate cancer patients. However, it is well-known that biopsy Grade Group tends to up- or downgrade significantly at radical prostatectomy. We aimed to investigate the correlation between accuracy and biopsy core number, performed immunohistochemical staining (IHC) or prostatectomy specimen sampling, with the latest also being correlated with higher detection rates of adverse pathological features, e.g., positive surgical margins, higher pathological stage or presence of perineural invasion (PnI status). The study cohort consisted of 315 consecutive patients diagnosed with prostate adenocarcinoma via transrectal ultrasound-guided needle biopsy who later underwent radical prostatectomy. We grouped and compared patients based on Grade Group accuracy, presence of IHC on biopsy, margin status, pathological stage, and PnI status. Inter-observer reproducibility was also calculated. Statistical analyzes included ANOVA, Tukey's multiple comparisons post hoc test, Chi-squared test, and Fleiss kappa statistics. Undergraded cases harboured a significantly lower number of biopsy cores (p < 0.05), than accurately graded cases. Using IHC did not affect grading accuracy significantly, nor did the number of slides from prostatectomy specimens. The mean number of slides was virtually identical when margin status, pathological stage and PnI status of prostatectomy specimens were compared. Inter-observer reproducibility at our institute was calculated as fair (overall kappa = 0.29). Grade Group accuracy is significantly improved by obtaining more cores at biopsy but is unrelated to performed IHC. The extent of sampling prostatectomy specimens, however, did not affect accuracy and failed to significantly improve detection of adverse pathological features.
期刊介绍:
Pathology & Oncology Research (POR) is an interdisciplinary Journal at the interface of pathology and oncology including the preclinical and translational research, diagnostics and therapy. Furthermore, POR is an international forum for the rapid communication of reviews, original research, critical and topical reports with excellence and novelty. Published quarterly, POR is dedicated to keeping scientists informed of developments on the selected biomedical fields bridging the gap between basic research and clinical medicine. It is a special aim for POR to promote pathological and oncological publishing activity of colleagues in the Central and East European region. The journal will be of interest to pathologists, and a broad range of experimental and clinical oncologists, and related experts. POR is supported by an acknowledged international advisory board and the Arányi Fundation for modern pathology.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
