Khiem T Vu, Rachel M Wolfe, Jonathan E Lambird, Danielle L V Maracaja
{"title":"一例伴有异常骨髓肉芽肿的VEXAS综合征:诊断困境。","authors":"Khiem T Vu, Rachel M Wolfe, Jonathan E Lambird, Danielle L V Maracaja","doi":"10.1186/s41927-023-00343-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>VEXAS is a recently described inflammatory disease caused by mutations in the UBA1 gene. Symptoms are diverse and include fevers, cartilaginous inflammation, lung inflammation, vasculitis, neutrophilic dermatoses, and macrocytic anemia. Cytoplasmic inclusions in myeloid and erythroid progenitors in the bone marrow are a hallmark feature. Here we report the first case of VEXAS with non-caseating granulomas in the bone marrow.</p><p><strong>Case presentation: </strong>A 62-year-old Asian male presented with fevers, erythema nodosum, inflammatory arthritis, and periorbital inflammation. Labs were significant for persistently elevated inflammatory markers and macrocytic anemia. Over the years his symptoms and inflammatory markers only improved with glucocorticoids and recurred when prednisone dose was lowered below 15-20 mg daily. He underwent bone marrow biopsy showing non-caseating granulomas and PET scan showing hilar/mediastinal lymphadenopathy. He was initially diagnosed with IgG4-related disease (treated with rituximab) and later sarcoidosis (treated with infliximab). After failing these agents, the possibility of VEXAS was considered and later confirmed by molecular testing.</p><p><strong>Conclusions: </strong>To the best of our knowledge, this is the first observation of non-caseating granulomas in VEXAS, a cautionary reminder of its non-specificity since misinterpretation can lead to diagnostic delay. VEXAS should be in the differential in patients with symptoms of chronic inflammation responding positively to steroids (but not to B-cell depletion or TNF inhibition), which is in line with previous literature.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"7 1","pages":"18"},"PeriodicalIF":2.5000,"publicationDate":"2023-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332027/pdf/","citationCount":"0","resultStr":"{\"title\":\"A case of VEXAS syndrome presenting with unusual bone marrow granulomas: a diagnostic dilemma.\",\"authors\":\"Khiem T Vu, Rachel M Wolfe, Jonathan E Lambird, Danielle L V Maracaja\",\"doi\":\"10.1186/s41927-023-00343-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>VEXAS is a recently described inflammatory disease caused by mutations in the UBA1 gene. Symptoms are diverse and include fevers, cartilaginous inflammation, lung inflammation, vasculitis, neutrophilic dermatoses, and macrocytic anemia. Cytoplasmic inclusions in myeloid and erythroid progenitors in the bone marrow are a hallmark feature. Here we report the first case of VEXAS with non-caseating granulomas in the bone marrow.</p><p><strong>Case presentation: </strong>A 62-year-old Asian male presented with fevers, erythema nodosum, inflammatory arthritis, and periorbital inflammation. Labs were significant for persistently elevated inflammatory markers and macrocytic anemia. Over the years his symptoms and inflammatory markers only improved with glucocorticoids and recurred when prednisone dose was lowered below 15-20 mg daily. He underwent bone marrow biopsy showing non-caseating granulomas and PET scan showing hilar/mediastinal lymphadenopathy. He was initially diagnosed with IgG4-related disease (treated with rituximab) and later sarcoidosis (treated with infliximab). After failing these agents, the possibility of VEXAS was considered and later confirmed by molecular testing.</p><p><strong>Conclusions: </strong>To the best of our knowledge, this is the first observation of non-caseating granulomas in VEXAS, a cautionary reminder of its non-specificity since misinterpretation can lead to diagnostic delay. VEXAS should be in the differential in patients with symptoms of chronic inflammation responding positively to steroids (but not to B-cell depletion or TNF inhibition), which is in line with previous literature.</p>\",\"PeriodicalId\":9150,\"journal\":{\"name\":\"BMC Rheumatology\",\"volume\":\"7 1\",\"pages\":\"18\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332027/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41927-023-00343-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-023-00343-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
A case of VEXAS syndrome presenting with unusual bone marrow granulomas: a diagnostic dilemma.
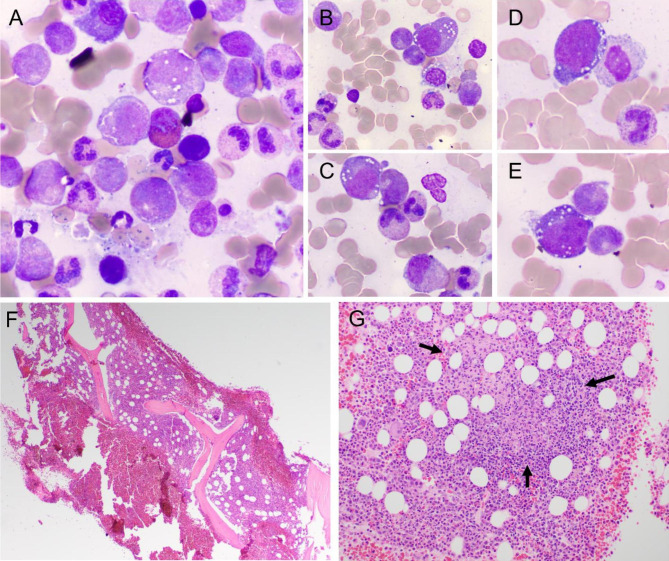
Background: VEXAS is a recently described inflammatory disease caused by mutations in the UBA1 gene. Symptoms are diverse and include fevers, cartilaginous inflammation, lung inflammation, vasculitis, neutrophilic dermatoses, and macrocytic anemia. Cytoplasmic inclusions in myeloid and erythroid progenitors in the bone marrow are a hallmark feature. Here we report the first case of VEXAS with non-caseating granulomas in the bone marrow.
Case presentation: A 62-year-old Asian male presented with fevers, erythema nodosum, inflammatory arthritis, and periorbital inflammation. Labs were significant for persistently elevated inflammatory markers and macrocytic anemia. Over the years his symptoms and inflammatory markers only improved with glucocorticoids and recurred when prednisone dose was lowered below 15-20 mg daily. He underwent bone marrow biopsy showing non-caseating granulomas and PET scan showing hilar/mediastinal lymphadenopathy. He was initially diagnosed with IgG4-related disease (treated with rituximab) and later sarcoidosis (treated with infliximab). After failing these agents, the possibility of VEXAS was considered and later confirmed by molecular testing.
Conclusions: To the best of our knowledge, this is the first observation of non-caseating granulomas in VEXAS, a cautionary reminder of its non-specificity since misinterpretation can lead to diagnostic delay. VEXAS should be in the differential in patients with symptoms of chronic inflammation responding positively to steroids (but not to B-cell depletion or TNF inhibition), which is in line with previous literature.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
