Fouad Jaber, Azizullah Beran, Saqr Alsakarneh, Khalid Ahmed, Mohamed Abdallah, Khaled Elfert, Mohammad Almeqdadi, Mohammed Jaber, Wael T Mohamed, Mohamd Ahmed, Laith Al Momani, Laith Numan, Thomas Bierman, John H Helzberg, Hassan Ghoz, Wendell K Clarkston
{"title":"经颈静脉肝内门静脉系统分流术伴或不伴胃食管静脉曲张栓塞预防静脉曲张再出血:系统回顾和荟萃分析","authors":"Fouad Jaber, Azizullah Beran, Saqr Alsakarneh, Khalid Ahmed, Mohamed Abdallah, Khaled Elfert, Mohammad Almeqdadi, Mohammed Jaber, Wael T Mohamed, Mohamd Ahmed, Laith Al Momani, Laith Numan, Thomas Bierman, John H Helzberg, Hassan Ghoz, Wendell K Clarkston","doi":"10.14740/gr1618","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of variceal embolization (VE) during transjugular intrahepatic portosystemic shunt (TIPS) creation for preventing gastroesophageal variceal rebleeding remains controversial. Therefore, we performed a meta-analysis to compare the incidence of variceal rebleeding, shunt dysfunction, encephalopathy, and death between patients treated with TIPS alone and those treated with TIPS in combination with VE.</p><p><strong>Methods: </strong>We performed a literature search using PubMed, EMBASE, Scopus, and Cochrane databases for all studies comparing the incidence of complications between TIPS alone and TIPS with VE. The primary outcome was variceal rebleeding. Secondary outcomes include shunt dysfunction, encephalopathy, and death. Subgroup analysis was performed based on the type of stent (covered vs. bare metal). The random-effects model was used to calculate the relative risk (RR) with the corresponding 95% confidence intervals (CIs) of outcome. A P value < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>Eleven studies with a total of 1,075 patients were included (597: TIPS alone and 478: TIPS plus VE). Compared to the TIPS alone, the TIPS with VE had a significantly lower incidence of variceal rebleeding (RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001). Subgroup analysis revealed similar results in covered stents (RR: 0.56, 95% CI: 0.36 - 0.86, P = 0.008) but there was no significant difference between the two groups in the subgroup analysis of bare stents and combined stents. There was no significant difference in the risk of encephalopathy (RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13), shunt dysfunction (RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40), and death (RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34). There were similarly no differences in these secondary outcomes between groups when stratified according to type of stent.</p><p><strong>Conclusions: </strong>Adding VE to TIPS reduced the incidence of variceal rebleeding in patients with cirrhosis. However, the benefit was observed with covered stents only. Further large-scale randomized controlled trials are warranted to validate our findings.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 2","pages":"68-78"},"PeriodicalIF":1.7000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/42/gr-16-068.PMC10181335.pdf","citationCount":"0","resultStr":"{\"title\":\"Transjugular Intrahepatic Portosystemic Shunt With or Without Gastroesophageal Variceal Embolization for the Prevention of Variceal Rebleeding: A Systematic Review and Meta-Analysis.\",\"authors\":\"Fouad Jaber, Azizullah Beran, Saqr Alsakarneh, Khalid Ahmed, Mohamed Abdallah, Khaled Elfert, Mohammad Almeqdadi, Mohammed Jaber, Wael T Mohamed, Mohamd Ahmed, Laith Al Momani, Laith Numan, Thomas Bierman, John H Helzberg, Hassan Ghoz, Wendell K Clarkston\",\"doi\":\"10.14740/gr1618\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The role of variceal embolization (VE) during transjugular intrahepatic portosystemic shunt (TIPS) creation for preventing gastroesophageal variceal rebleeding remains controversial. Therefore, we performed a meta-analysis to compare the incidence of variceal rebleeding, shunt dysfunction, encephalopathy, and death between patients treated with TIPS alone and those treated with TIPS in combination with VE.</p><p><strong>Methods: </strong>We performed a literature search using PubMed, EMBASE, Scopus, and Cochrane databases for all studies comparing the incidence of complications between TIPS alone and TIPS with VE. The primary outcome was variceal rebleeding. Secondary outcomes include shunt dysfunction, encephalopathy, and death. Subgroup analysis was performed based on the type of stent (covered vs. bare metal). The random-effects model was used to calculate the relative risk (RR) with the corresponding 95% confidence intervals (CIs) of outcome. A P value < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>Eleven studies with a total of 1,075 patients were included (597: TIPS alone and 478: TIPS plus VE). Compared to the TIPS alone, the TIPS with VE had a significantly lower incidence of variceal rebleeding (RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001). Subgroup analysis revealed similar results in covered stents (RR: 0.56, 95% CI: 0.36 - 0.86, P = 0.008) but there was no significant difference between the two groups in the subgroup analysis of bare stents and combined stents. There was no significant difference in the risk of encephalopathy (RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13), shunt dysfunction (RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40), and death (RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34). There were similarly no differences in these secondary outcomes between groups when stratified according to type of stent.</p><p><strong>Conclusions: </strong>Adding VE to TIPS reduced the incidence of variceal rebleeding in patients with cirrhosis. However, the benefit was observed with covered stents only. Further large-scale randomized controlled trials are warranted to validate our findings.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"16 2\",\"pages\":\"68-78\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/42/gr-16-068.PMC10181335.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr1618\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1618","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:静脉曲张栓塞(VE)在经颈静脉肝内门静脉系统分流术(TIPS)中预防胃食管静脉曲张再出血的作用仍然存在争议。因此,我们进行了一项荟萃分析,比较单独使用TIPS和联合使用VE的患者的静脉曲张再出血、分流功能障碍、脑病和死亡的发生率。方法:我们使用PubMed、EMBASE、Scopus和Cochrane数据库进行文献检索,比较TIPS单独使用和TIPS联合VE的并发症发生率。主要结局是静脉曲张再出血。次要结局包括分流功能障碍、脑病和死亡。根据支架类型(覆盖与裸金属)进行亚组分析。采用随机效应模型计算相对危险度(RR)和相应的95%置信区间(ci)。P值< 0.05为差异有统计学意义。结果:纳入了11项研究,共1,075例患者(597例:TIPS单独,478例:TIPS加VE)。与单独使用TIPS相比,TIPS合并VE的静脉曲张再出血发生率显著降低(RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001)。亚组分析显示,覆盖支架组的结果相似(RR: 0.56, 95% CI: 0.36 ~ 0.86, P = 0.008),但两组在裸支架和联合支架的亚组分析中差异无统计学意义。脑病(RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13)、分流功能障碍(RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40)和死亡(RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34)的风险无显著差异。同样,根据支架类型进行分层时,各组之间的这些次要结果也没有差异。结论:在TIPS中加入VE可降低肝硬化患者静脉曲张再出血的发生率。然而,只有覆盖支架才能观察到这种益处。需要进一步的大规模随机对照试验来验证我们的发现。
Transjugular Intrahepatic Portosystemic Shunt With or Without Gastroesophageal Variceal Embolization for the Prevention of Variceal Rebleeding: A Systematic Review and Meta-Analysis.
Background: The role of variceal embolization (VE) during transjugular intrahepatic portosystemic shunt (TIPS) creation for preventing gastroesophageal variceal rebleeding remains controversial. Therefore, we performed a meta-analysis to compare the incidence of variceal rebleeding, shunt dysfunction, encephalopathy, and death between patients treated with TIPS alone and those treated with TIPS in combination with VE.
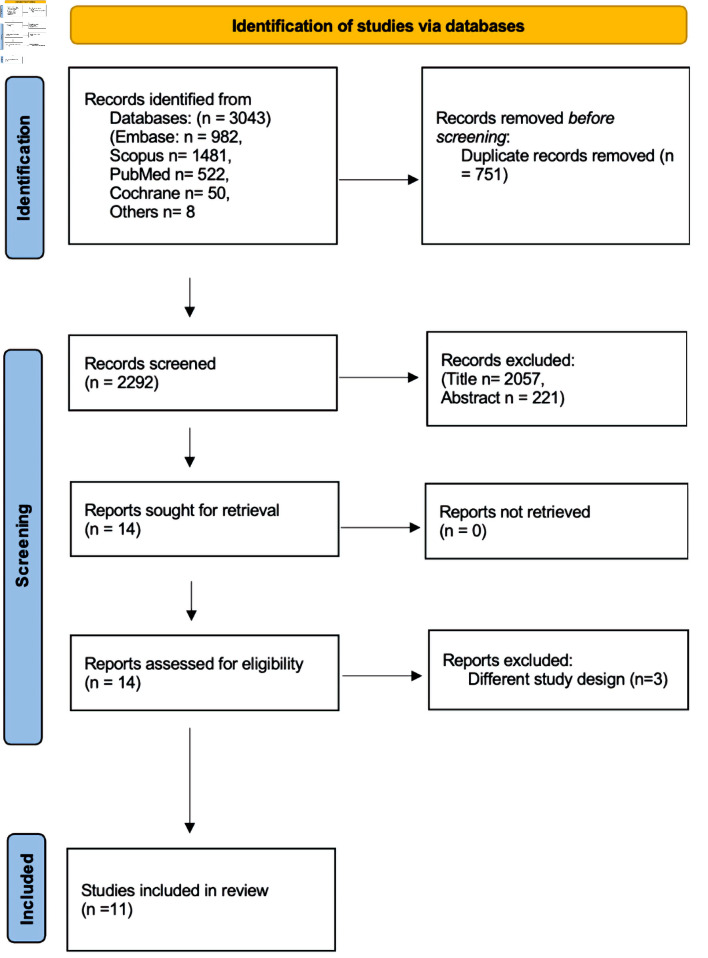
Methods: We performed a literature search using PubMed, EMBASE, Scopus, and Cochrane databases for all studies comparing the incidence of complications between TIPS alone and TIPS with VE. The primary outcome was variceal rebleeding. Secondary outcomes include shunt dysfunction, encephalopathy, and death. Subgroup analysis was performed based on the type of stent (covered vs. bare metal). The random-effects model was used to calculate the relative risk (RR) with the corresponding 95% confidence intervals (CIs) of outcome. A P value < 0.05 was considered statistically significant.
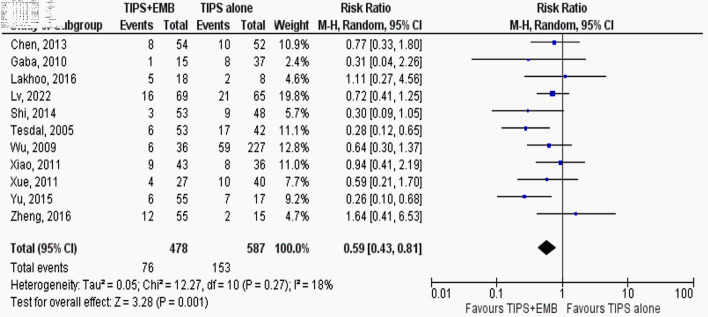
Results: Eleven studies with a total of 1,075 patients were included (597: TIPS alone and 478: TIPS plus VE). Compared to the TIPS alone, the TIPS with VE had a significantly lower incidence of variceal rebleeding (RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001). Subgroup analysis revealed similar results in covered stents (RR: 0.56, 95% CI: 0.36 - 0.86, P = 0.008) but there was no significant difference between the two groups in the subgroup analysis of bare stents and combined stents. There was no significant difference in the risk of encephalopathy (RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13), shunt dysfunction (RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40), and death (RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34). There were similarly no differences in these secondary outcomes between groups when stratified according to type of stent.
Conclusions: Adding VE to TIPS reduced the incidence of variceal rebleeding in patients with cirrhosis. However, the benefit was observed with covered stents only. Further large-scale randomized controlled trials are warranted to validate our findings.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
