Amiya Ahsan, Hussameldin M Nour, Dimitra V Peristeri, Sameh Abogabal, Christie Swaminathan, Muhammad S Sajid
{"title":"系统评价与meta分析腹腔镜结肠直肠癌切除术后横向与垂直中线提取切口疝的风险。","authors":"Amiya Ahsan, Hussameldin M Nour, Dimitra V Peristeri, Sameh Abogabal, Christie Swaminathan, Muhammad S Sajid","doi":"10.21037/tgh-22-75","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this article is to explore the risk of incisional hernia (IH) occurrence at the site of specimen extraction following laparoscopic colorectal resection (LCR), highlighting the comparison between transverse incision versus midline vertical abdominal incision.</p><p><strong>Methods: </strong>Analysis was conducted according to PRISMA guidelines. Systematic search of medical databases, EMBASE, MEDLINE, PubMed and Cochrane Library were performed to find all types of comparative studies reporting the incidence of IH at the specimen extraction site of transverse or vertical midline incision following LCR. The analysis of the pooled data was done using the RevMan statistical software.</p><p><strong>Results: </strong>Twenty-five comparative studies (including 2 randomised controlled trials) on 10,362 patients fulfilled the inclusion criteria. There were 4,944 patients in the transverse incision group and 5,418 patients in the vertical midline incision group. In the random effects model analysis, the use of transverse incision for specimen extraction following LCR reduced the risk of IH development (odds ratio =0.30, 95% CI: 0.19-0.49, Z=4.88, P=0.00001). However, there was significant heterogeneity (Tau<sup>2</sup>=0.97; Chi<sup>2</sup>=109.98, df=24, P=0.00004; I<sup>2</sup>=78%) among included studies. The limitation of the study is due to lack of RCTs, this study includes both prospective and retrospective studies along with 2 RCTs which makes the meta-analysis potentially biased in source of evidence.</p><p><strong>Conclusions: </strong>Transverse incision used for specimen extraction following LCR seems to reduce the risk of postoperative IH incidence compared to vertical midline abdominal incisions.</p>","PeriodicalId":23267,"journal":{"name":"Translational gastroenterology and hepatology","volume":"8 ","pages":"16"},"PeriodicalIF":3.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5b/c2/tgh-08-22-75.PMC10184032.pdf","citationCount":"0","resultStr":"{\"title\":\"Systematic review with meta-analysis of transverse <i>vs.</i> vertical midline extraction incisional hernia risk following laparoscopic colorectal resections.\",\"authors\":\"Amiya Ahsan, Hussameldin M Nour, Dimitra V Peristeri, Sameh Abogabal, Christie Swaminathan, Muhammad S Sajid\",\"doi\":\"10.21037/tgh-22-75\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aim of this article is to explore the risk of incisional hernia (IH) occurrence at the site of specimen extraction following laparoscopic colorectal resection (LCR), highlighting the comparison between transverse incision versus midline vertical abdominal incision.</p><p><strong>Methods: </strong>Analysis was conducted according to PRISMA guidelines. Systematic search of medical databases, EMBASE, MEDLINE, PubMed and Cochrane Library were performed to find all types of comparative studies reporting the incidence of IH at the specimen extraction site of transverse or vertical midline incision following LCR. The analysis of the pooled data was done using the RevMan statistical software.</p><p><strong>Results: </strong>Twenty-five comparative studies (including 2 randomised controlled trials) on 10,362 patients fulfilled the inclusion criteria. There were 4,944 patients in the transverse incision group and 5,418 patients in the vertical midline incision group. In the random effects model analysis, the use of transverse incision for specimen extraction following LCR reduced the risk of IH development (odds ratio =0.30, 95% CI: 0.19-0.49, Z=4.88, P=0.00001). However, there was significant heterogeneity (Tau<sup>2</sup>=0.97; Chi<sup>2</sup>=109.98, df=24, P=0.00004; I<sup>2</sup>=78%) among included studies. The limitation of the study is due to lack of RCTs, this study includes both prospective and retrospective studies along with 2 RCTs which makes the meta-analysis potentially biased in source of evidence.</p><p><strong>Conclusions: </strong>Transverse incision used for specimen extraction following LCR seems to reduce the risk of postoperative IH incidence compared to vertical midline abdominal incisions.</p>\",\"PeriodicalId\":23267,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"8 \",\"pages\":\"16\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5b/c2/tgh-08-22-75.PMC10184032.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-22-75\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tgh-22-75","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Systematic review with meta-analysis of transverse vs. vertical midline extraction incisional hernia risk following laparoscopic colorectal resections.
Background: The aim of this article is to explore the risk of incisional hernia (IH) occurrence at the site of specimen extraction following laparoscopic colorectal resection (LCR), highlighting the comparison between transverse incision versus midline vertical abdominal incision.
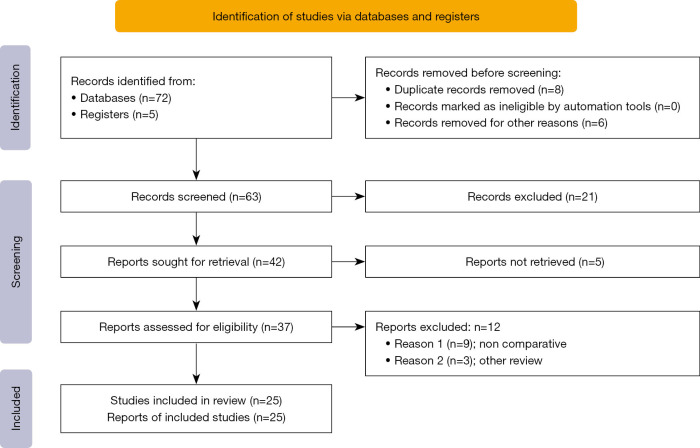
Methods: Analysis was conducted according to PRISMA guidelines. Systematic search of medical databases, EMBASE, MEDLINE, PubMed and Cochrane Library were performed to find all types of comparative studies reporting the incidence of IH at the specimen extraction site of transverse or vertical midline incision following LCR. The analysis of the pooled data was done using the RevMan statistical software.
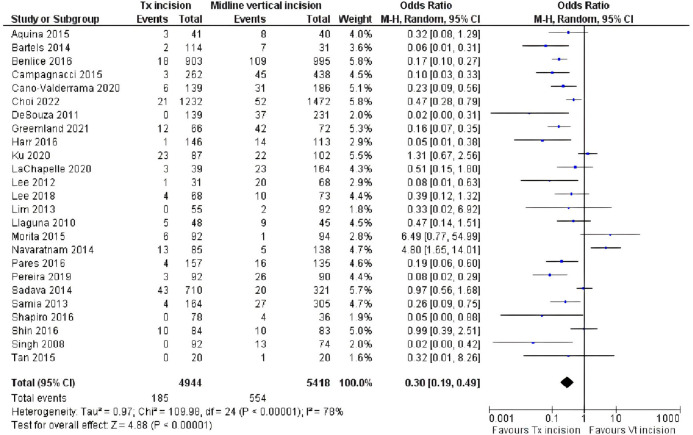
Results: Twenty-five comparative studies (including 2 randomised controlled trials) on 10,362 patients fulfilled the inclusion criteria. There were 4,944 patients in the transverse incision group and 5,418 patients in the vertical midline incision group. In the random effects model analysis, the use of transverse incision for specimen extraction following LCR reduced the risk of IH development (odds ratio =0.30, 95% CI: 0.19-0.49, Z=4.88, P=0.00001). However, there was significant heterogeneity (Tau2=0.97; Chi2=109.98, df=24, P=0.00004; I2=78%) among included studies. The limitation of the study is due to lack of RCTs, this study includes both prospective and retrospective studies along with 2 RCTs which makes the meta-analysis potentially biased in source of evidence.
Conclusions: Transverse incision used for specimen extraction following LCR seems to reduce the risk of postoperative IH incidence compared to vertical midline abdominal incisions.
期刊介绍:
Translational Gastroenterology and Hepatology (Transl Gastroenterol Hepatol; TGH; Online ISSN 2415-1289) is an open-access, peer-reviewed online journal that focuses on cutting-edge findings in the field of translational research in gastroenterology and hepatology and provides current and practical information on diagnosis, prevention and clinical investigations of gastrointestinal, pancreas, gallbladder and hepatic diseases. Specific areas of interest include, but not limited to, multimodality therapy, biomarkers, imaging, biology, pathology, and technical advances related to gastrointestinal and hepatic diseases. Contributions pertinent to gastroenterology and hepatology are also included from related fields such as nutrition, surgery, public health, human genetics, basic sciences, education, sociology, and nursing.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
