Than-Van Sy, Le Thanh Dung, Bui-Van Giang, Nguyen Quang Nghia, Ninh Viet Khai, Cao Manh Thau, Pham Gia Anh, Trinh Hong Son, Nguyen Minh Duc
{"title":"肝细胞癌大肝切除术前经动脉化疗栓塞后肝静脉剥夺的安全性和有效性。","authors":"Than-Van Sy, Le Thanh Dung, Bui-Van Giang, Nguyen Quang Nghia, Ninh Viet Khai, Cao Manh Thau, Pham Gia Anh, Trinh Hong Son, Nguyen Minh Duc","doi":"10.2147/TCRM.S411080","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to evaluate the safety and efficacy of liver venous deprivation (LVD) following transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC).</p><p><strong>Methods: </strong>Between January 2021 and December 2022, HCC patients indicated for hepatectomy with initial insufficient future liver remnant (FLR) underwent LVD after TACE to induce preoperative liver hypertrophy.</p><p><strong>Results: </strong>Twenty-seven HCC patients with a median age of 55 years underwent LVD. No TACE or LVD procedure-associated complications occurred, except for 1 case presenting with grade A liver failure after LVD (then recovered after 7 days). The FLR volume was 29.3% (interquartile range [IQR] = 7.5) and 48.9% (IQR = 8.6) of the total liver volume before and after LVD, respectively (p < 0.001). The degree of hypertrophy and FLR hypertrophy rate were 14.8% (IQR = 8.4) and 55.2% (IQR = 36.7), respectively. All 27 patients demonstrated sufficient FLR after LVD (24 patients at three weeks post-LVD, one at six weeks, and two at ten weeks), but only 21 patients accepted surgery. Postoperative histopathology showed 16 patients with cirrhosis and five with mild fibrosis (F1, F2). One patient presented with severe intraoperative bleeding due to damage of left hepatic vein and developed grade C liver failure, then died on day 32 postoperation.</p><p><strong>Conclusion: </strong>LVD following TACE seems to be a safe, effective, and feasible method of inducing significant FLR regeneration in HCC, even in well-selected cirrhotic livers. Comparative studies with a large patient population and multicenter data are needed for further evaluation.</p>","PeriodicalId":48769,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"19 ","pages":"425-433"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d6/33/tcrm-19-425.PMC10202697.pdf","citationCount":"0","resultStr":"{\"title\":\"Safety and Efficacy of Liver Venous Deprivation Following Transarterial Chemoembolization Before Major Hepatectomy for Hepatocellular Carcinoma.\",\"authors\":\"Than-Van Sy, Le Thanh Dung, Bui-Van Giang, Nguyen Quang Nghia, Ninh Viet Khai, Cao Manh Thau, Pham Gia Anh, Trinh Hong Son, Nguyen Minh Duc\",\"doi\":\"10.2147/TCRM.S411080\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aimed to evaluate the safety and efficacy of liver venous deprivation (LVD) following transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC).</p><p><strong>Methods: </strong>Between January 2021 and December 2022, HCC patients indicated for hepatectomy with initial insufficient future liver remnant (FLR) underwent LVD after TACE to induce preoperative liver hypertrophy.</p><p><strong>Results: </strong>Twenty-seven HCC patients with a median age of 55 years underwent LVD. No TACE or LVD procedure-associated complications occurred, except for 1 case presenting with grade A liver failure after LVD (then recovered after 7 days). The FLR volume was 29.3% (interquartile range [IQR] = 7.5) and 48.9% (IQR = 8.6) of the total liver volume before and after LVD, respectively (p < 0.001). The degree of hypertrophy and FLR hypertrophy rate were 14.8% (IQR = 8.4) and 55.2% (IQR = 36.7), respectively. All 27 patients demonstrated sufficient FLR after LVD (24 patients at three weeks post-LVD, one at six weeks, and two at ten weeks), but only 21 patients accepted surgery. Postoperative histopathology showed 16 patients with cirrhosis and five with mild fibrosis (F1, F2). One patient presented with severe intraoperative bleeding due to damage of left hepatic vein and developed grade C liver failure, then died on day 32 postoperation.</p><p><strong>Conclusion: </strong>LVD following TACE seems to be a safe, effective, and feasible method of inducing significant FLR regeneration in HCC, even in well-selected cirrhotic livers. Comparative studies with a large patient population and multicenter data are needed for further evaluation.</p>\",\"PeriodicalId\":48769,\"journal\":{\"name\":\"Therapeutics and Clinical Risk Management\",\"volume\":\"19 \",\"pages\":\"425-433\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d6/33/tcrm-19-425.PMC10202697.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutics and Clinical Risk Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/TCRM.S411080\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S411080","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Safety and Efficacy of Liver Venous Deprivation Following Transarterial Chemoembolization Before Major Hepatectomy for Hepatocellular Carcinoma.
Objective: This study aimed to evaluate the safety and efficacy of liver venous deprivation (LVD) following transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC).
Methods: Between January 2021 and December 2022, HCC patients indicated for hepatectomy with initial insufficient future liver remnant (FLR) underwent LVD after TACE to induce preoperative liver hypertrophy.
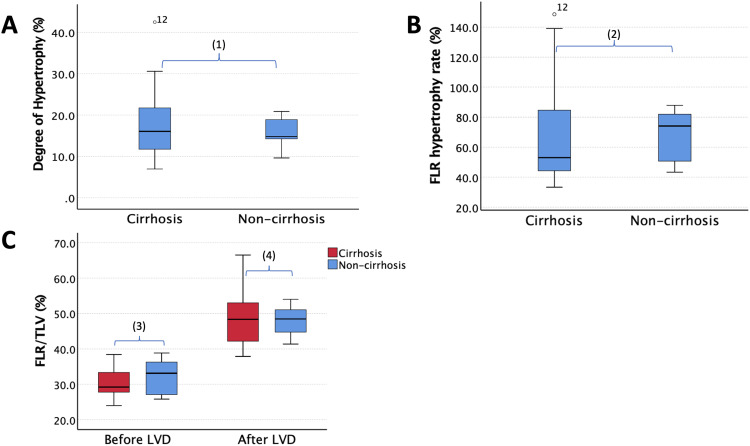
Results: Twenty-seven HCC patients with a median age of 55 years underwent LVD. No TACE or LVD procedure-associated complications occurred, except for 1 case presenting with grade A liver failure after LVD (then recovered after 7 days). The FLR volume was 29.3% (interquartile range [IQR] = 7.5) and 48.9% (IQR = 8.6) of the total liver volume before and after LVD, respectively (p < 0.001). The degree of hypertrophy and FLR hypertrophy rate were 14.8% (IQR = 8.4) and 55.2% (IQR = 36.7), respectively. All 27 patients demonstrated sufficient FLR after LVD (24 patients at three weeks post-LVD, one at six weeks, and two at ten weeks), but only 21 patients accepted surgery. Postoperative histopathology showed 16 patients with cirrhosis and five with mild fibrosis (F1, F2). One patient presented with severe intraoperative bleeding due to damage of left hepatic vein and developed grade C liver failure, then died on day 32 postoperation.
Conclusion: LVD following TACE seems to be a safe, effective, and feasible method of inducing significant FLR regeneration in HCC, even in well-selected cirrhotic livers. Comparative studies with a large patient population and multicenter data are needed for further evaluation.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
