{"title":"具有复合生发中心和非生发中心类型的弥漫性大B细胞淋巴瘤:附2例报告。","authors":"Ayumi Sugitani, Suguru Fukuhara, Maki Shibata, Ryosuke Ichihara, Haruhi Furukawa, Akiko Miyagi Maeshima","doi":"10.3960/jslrt.23020","DOIUrl":null,"url":null,"abstract":"<p><p>We report two cases of diffuse large B-cell lymphoma (DLBCL) with composite germinal center B-cell (GCB) and non-GCB types. Case 1 was a 72-year-old woman with inguinal lymph node swelling. Two morphologically different lesions were concurrently observed in needle biopsy specimens. One lesion was DLBCL with centroblastic morphology and a GCB phenotype (CD10<sup>+</sup>, BCL6<sup>+</sup>, and MUM1<sup>-</sup>), according to the Hans algorithm. The other lesion was DLBCL with anaplastic morphology and a non-GCB phenotype (CD10<sup>-</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>). Considering cellular atypia, the GCB-type DLBCL likely progressed to non-GCB-type DLBCL. Case 2 was a 34-year-old man who underwent ileocecal resection, with four lesions observed in the ileum. All four lesions indicated centroblastic morphology. Three lesions showed a GCB phenotype (CD10<sup>+</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>), while the other showed a non-GCB phenotype (CD10<sup>-</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>). These tumors were clonally related. BCL2 expression and MYC rearrangement were not related to changes in the cell of origin (COO) in either case. In conclusion, changes in the COO in DLBCL may not be uncommon. Therefore, investigation of the COO in other sites or at relapse may be needed if new drugs with different indications for each COO are developed.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":" ","pages":"181-186"},"PeriodicalIF":1.4000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628827/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diffuse large B-cell lymphoma with composite germinal center and non-germinal center types: A report of two cases.\",\"authors\":\"Ayumi Sugitani, Suguru Fukuhara, Maki Shibata, Ryosuke Ichihara, Haruhi Furukawa, Akiko Miyagi Maeshima\",\"doi\":\"10.3960/jslrt.23020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report two cases of diffuse large B-cell lymphoma (DLBCL) with composite germinal center B-cell (GCB) and non-GCB types. Case 1 was a 72-year-old woman with inguinal lymph node swelling. Two morphologically different lesions were concurrently observed in needle biopsy specimens. One lesion was DLBCL with centroblastic morphology and a GCB phenotype (CD10<sup>+</sup>, BCL6<sup>+</sup>, and MUM1<sup>-</sup>), according to the Hans algorithm. The other lesion was DLBCL with anaplastic morphology and a non-GCB phenotype (CD10<sup>-</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>). Considering cellular atypia, the GCB-type DLBCL likely progressed to non-GCB-type DLBCL. Case 2 was a 34-year-old man who underwent ileocecal resection, with four lesions observed in the ileum. All four lesions indicated centroblastic morphology. Three lesions showed a GCB phenotype (CD10<sup>+</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>), while the other showed a non-GCB phenotype (CD10<sup>-</sup>, BCL6<sup>+</sup>, and MUM1<sup>+</sup>). These tumors were clonally related. BCL2 expression and MYC rearrangement were not related to changes in the cell of origin (COO) in either case. In conclusion, changes in the COO in DLBCL may not be uncommon. Therefore, investigation of the COO in other sites or at relapse may be needed if new drugs with different indications for each COO are developed.</p>\",\"PeriodicalId\":45936,\"journal\":{\"name\":\"Journal of Clinical and Experimental Hematopathology\",\"volume\":\" \",\"pages\":\"181-186\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628827/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Experimental Hematopathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3960/jslrt.23020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.23020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Diffuse large B-cell lymphoma with composite germinal center and non-germinal center types: A report of two cases.
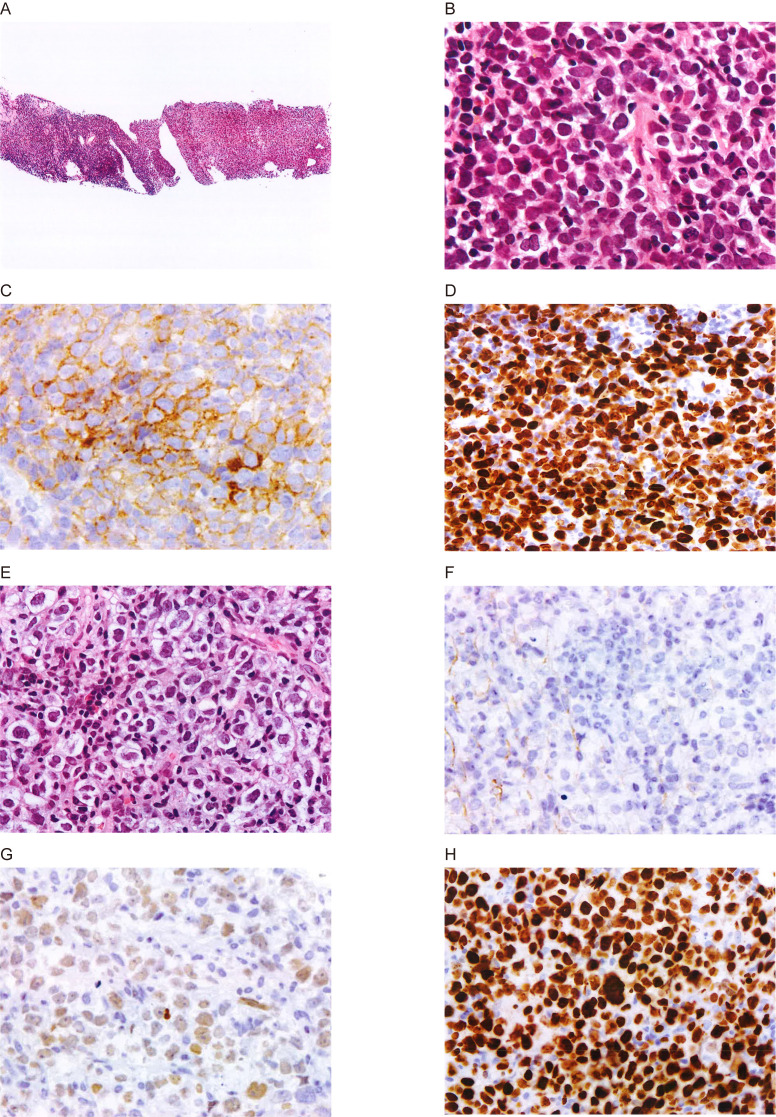
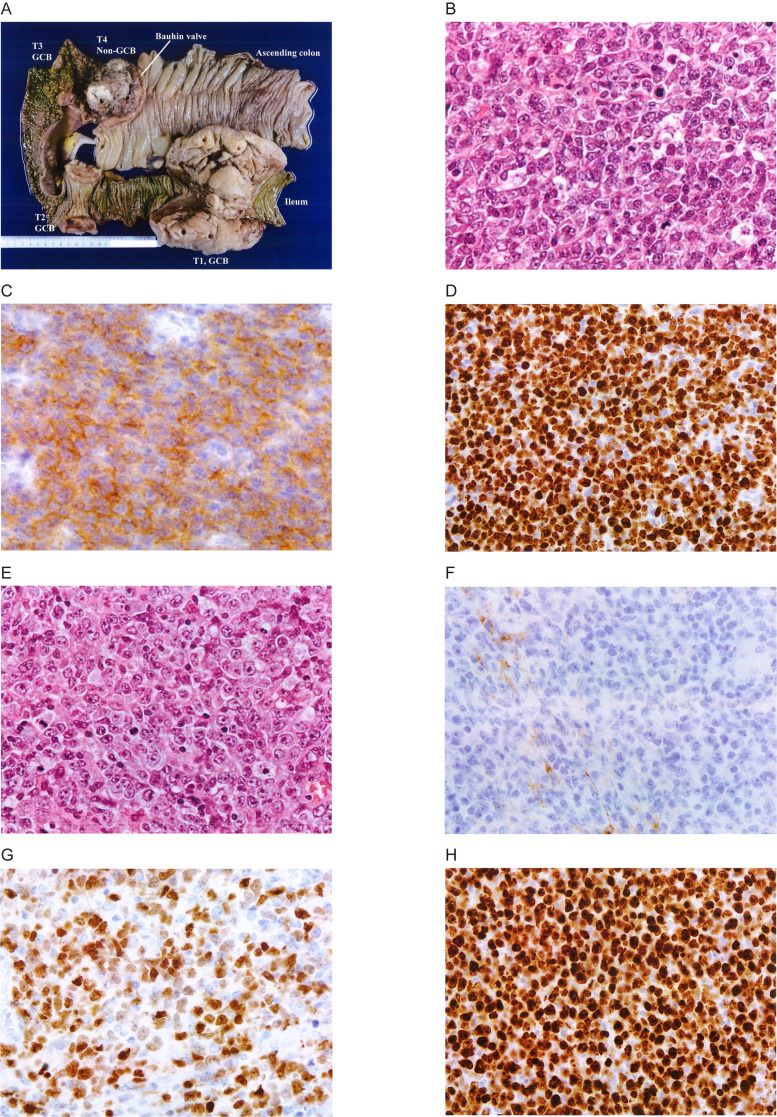
We report two cases of diffuse large B-cell lymphoma (DLBCL) with composite germinal center B-cell (GCB) and non-GCB types. Case 1 was a 72-year-old woman with inguinal lymph node swelling. Two morphologically different lesions were concurrently observed in needle biopsy specimens. One lesion was DLBCL with centroblastic morphology and a GCB phenotype (CD10+, BCL6+, and MUM1-), according to the Hans algorithm. The other lesion was DLBCL with anaplastic morphology and a non-GCB phenotype (CD10-, BCL6+, and MUM1+). Considering cellular atypia, the GCB-type DLBCL likely progressed to non-GCB-type DLBCL. Case 2 was a 34-year-old man who underwent ileocecal resection, with four lesions observed in the ileum. All four lesions indicated centroblastic morphology. Three lesions showed a GCB phenotype (CD10+, BCL6+, and MUM1+), while the other showed a non-GCB phenotype (CD10-, BCL6+, and MUM1+). These tumors were clonally related. BCL2 expression and MYC rearrangement were not related to changes in the cell of origin (COO) in either case. In conclusion, changes in the COO in DLBCL may not be uncommon. Therefore, investigation of the COO in other sites or at relapse may be needed if new drugs with different indications for each COO are developed.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
