Filipe A Moura, David D Berg, Andrea Bellavia, Jamie P Dwyer, Ofri Mosenzon, Benjamin M Scirica, Stephen D Wiviott, Deepak L Bhatt, Itamar Raz, Mark W Feinberg, Eugene Braunwald, David A Morrow, Marc S Sabatine
{"title":"2型糖尿病患者肾脏疾病进展的风险评估和SGLT2抑制的疗效。","authors":"Filipe A Moura, David D Berg, Andrea Bellavia, Jamie P Dwyer, Ofri Mosenzon, Benjamin M Scirica, Stephen D Wiviott, Deepak L Bhatt, Itamar Raz, Mark W Feinberg, Eugene Braunwald, David A Morrow, Marc S Sabatine","doi":"10.2337/dc23-0492","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To develop a risk assessment tool to identify patients with type 2 diabetes (T2D) at higher risk for kidney disease progression and who might benefit more from sodium-glucose cotransporter 2 (SGLT2) inhibition.</p><p><strong>Research design and methods: </strong>A total of 41,204 patients with T2D from four Thrombolysis In Myocardial Infarction (TIMI) clinical trials were divided into derivation (70%) and validation cohorts (30%). Candidate predictors of kidney disease progression (composite of sustained ≥40% decline in estimated glomerular filtration rate [eGFR], end-stage kidney disease, or kidney death) were selected with multivariable Cox regression. Efficacy of dapagliflozin was assessed by risk categories (low: <0.5%; intermediate: 0.5 to <2%; high: ≥2%) in Dapagliflozin Effect on Cardiovascular Events (DECLARE)-TIMI 58.</p><p><strong>Results: </strong>There were 695 events over a median follow-up of 2.4 years. The final model comprised eight independent predictors of kidney disease progression: atherosclerotic cardiovascular disease, heart failure, systolic blood pressure, T2D duration, glycated hemoglobin, eGFR, urine albumin-to-creatinine ratio, and hemoglobin. The c-indices were 0.798 (95% CI, 0.774-0.821) and 0.798 (95% CI, 0.765-0.831) in the derivation and validation cohort, respectively. The calibration plot slope (deciles of predicted vs. observed risk) was 0.98 (95% CI, 0.93-1.04) in the validation cohort. Whereas relative risk reductions with dapagliflozin did not differ across risk categories, there was greater absolute risk reduction in patients with higher baseline risk, with a 3.5% absolute risk reduction in kidney disease progression at 4 years in the highest risk group (≥1%/year). Results were similar with the 2022 Chronic Kidney Disease Prognosis Consortium risk prediction model.</p><p><strong>Conclusions: </strong>Risk models for kidney disease progression can be applied in patients with T2D to stratify risk and identify those who experience a greater magnitude of benefit from SGLT2 inhibition.</p>","PeriodicalId":11140,"journal":{"name":"Diabetes Care","volume":" ","pages":"1807-1815"},"PeriodicalIF":16.6000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10516252/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Assessment of Kidney Disease Progression and Efficacy of SGLT2 Inhibition in Patients With Type 2 Diabetes.\",\"authors\":\"Filipe A Moura, David D Berg, Andrea Bellavia, Jamie P Dwyer, Ofri Mosenzon, Benjamin M Scirica, Stephen D Wiviott, Deepak L Bhatt, Itamar Raz, Mark W Feinberg, Eugene Braunwald, David A Morrow, Marc S Sabatine\",\"doi\":\"10.2337/dc23-0492\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To develop a risk assessment tool to identify patients with type 2 diabetes (T2D) at higher risk for kidney disease progression and who might benefit more from sodium-glucose cotransporter 2 (SGLT2) inhibition.</p><p><strong>Research design and methods: </strong>A total of 41,204 patients with T2D from four Thrombolysis In Myocardial Infarction (TIMI) clinical trials were divided into derivation (70%) and validation cohorts (30%). Candidate predictors of kidney disease progression (composite of sustained ≥40% decline in estimated glomerular filtration rate [eGFR], end-stage kidney disease, or kidney death) were selected with multivariable Cox regression. Efficacy of dapagliflozin was assessed by risk categories (low: <0.5%; intermediate: 0.5 to <2%; high: ≥2%) in Dapagliflozin Effect on Cardiovascular Events (DECLARE)-TIMI 58.</p><p><strong>Results: </strong>There were 695 events over a median follow-up of 2.4 years. The final model comprised eight independent predictors of kidney disease progression: atherosclerotic cardiovascular disease, heart failure, systolic blood pressure, T2D duration, glycated hemoglobin, eGFR, urine albumin-to-creatinine ratio, and hemoglobin. The c-indices were 0.798 (95% CI, 0.774-0.821) and 0.798 (95% CI, 0.765-0.831) in the derivation and validation cohort, respectively. The calibration plot slope (deciles of predicted vs. observed risk) was 0.98 (95% CI, 0.93-1.04) in the validation cohort. Whereas relative risk reductions with dapagliflozin did not differ across risk categories, there was greater absolute risk reduction in patients with higher baseline risk, with a 3.5% absolute risk reduction in kidney disease progression at 4 years in the highest risk group (≥1%/year). Results were similar with the 2022 Chronic Kidney Disease Prognosis Consortium risk prediction model.</p><p><strong>Conclusions: </strong>Risk models for kidney disease progression can be applied in patients with T2D to stratify risk and identify those who experience a greater magnitude of benefit from SGLT2 inhibition.</p>\",\"PeriodicalId\":11140,\"journal\":{\"name\":\"Diabetes Care\",\"volume\":\" \",\"pages\":\"1807-1815\"},\"PeriodicalIF\":16.6000,\"publicationDate\":\"2023-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10516252/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2337/dc23-0492\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2337/dc23-0492","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Risk Assessment of Kidney Disease Progression and Efficacy of SGLT2 Inhibition in Patients With Type 2 Diabetes.
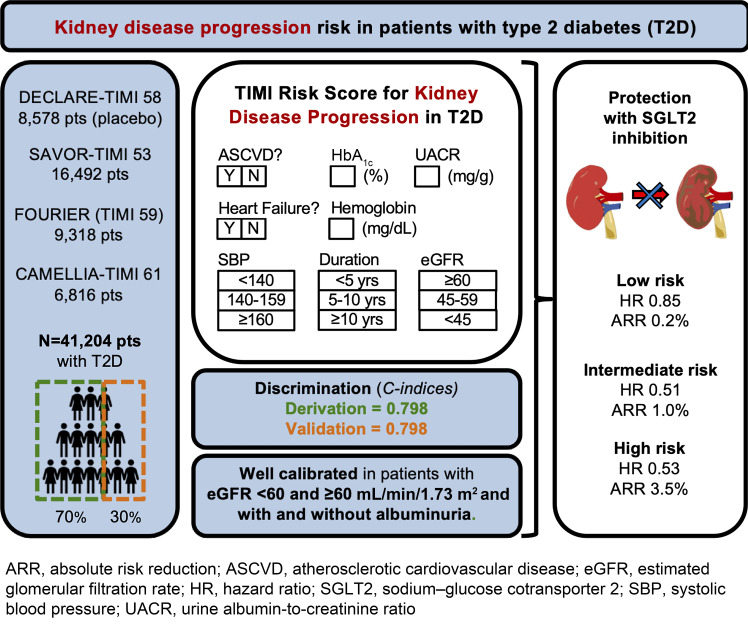
Objective: To develop a risk assessment tool to identify patients with type 2 diabetes (T2D) at higher risk for kidney disease progression and who might benefit more from sodium-glucose cotransporter 2 (SGLT2) inhibition.
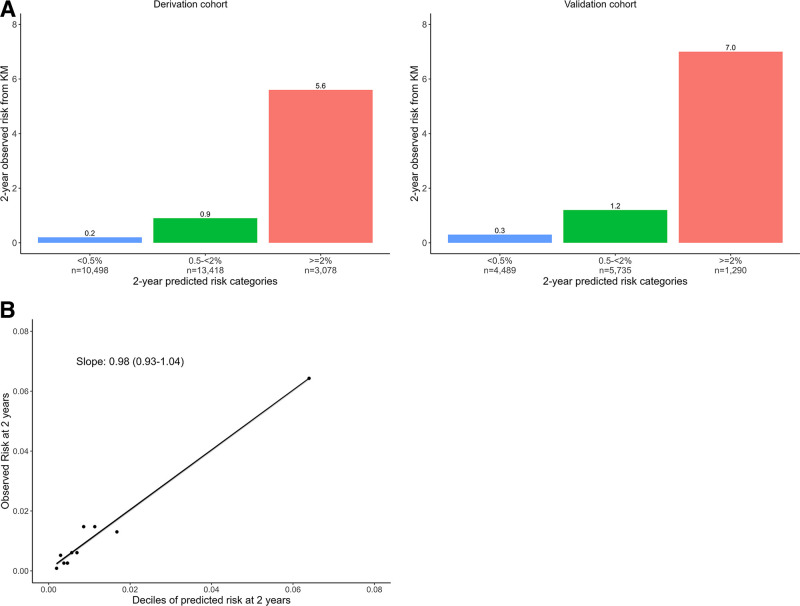
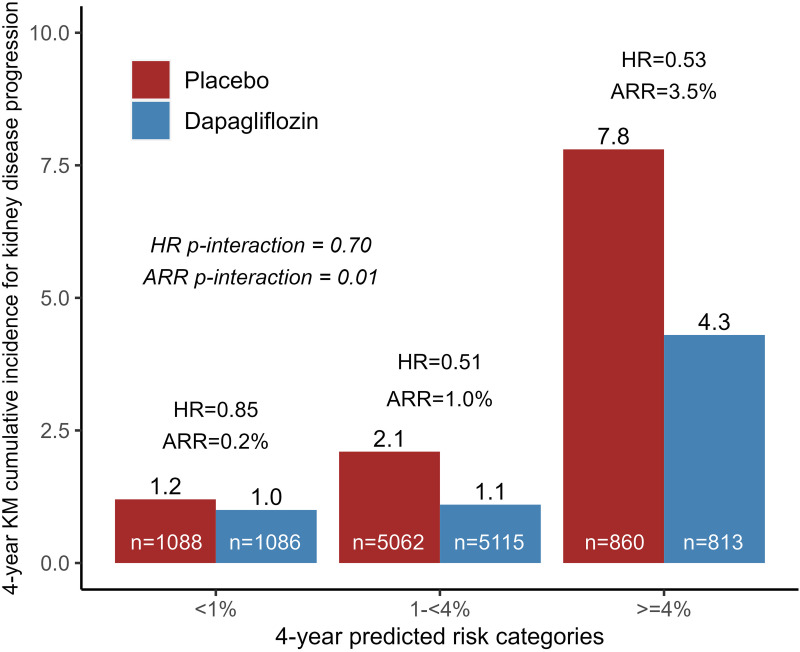
Research design and methods: A total of 41,204 patients with T2D from four Thrombolysis In Myocardial Infarction (TIMI) clinical trials were divided into derivation (70%) and validation cohorts (30%). Candidate predictors of kidney disease progression (composite of sustained ≥40% decline in estimated glomerular filtration rate [eGFR], end-stage kidney disease, or kidney death) were selected with multivariable Cox regression. Efficacy of dapagliflozin was assessed by risk categories (low: <0.5%; intermediate: 0.5 to <2%; high: ≥2%) in Dapagliflozin Effect on Cardiovascular Events (DECLARE)-TIMI 58.
Results: There were 695 events over a median follow-up of 2.4 years. The final model comprised eight independent predictors of kidney disease progression: atherosclerotic cardiovascular disease, heart failure, systolic blood pressure, T2D duration, glycated hemoglobin, eGFR, urine albumin-to-creatinine ratio, and hemoglobin. The c-indices were 0.798 (95% CI, 0.774-0.821) and 0.798 (95% CI, 0.765-0.831) in the derivation and validation cohort, respectively. The calibration plot slope (deciles of predicted vs. observed risk) was 0.98 (95% CI, 0.93-1.04) in the validation cohort. Whereas relative risk reductions with dapagliflozin did not differ across risk categories, there was greater absolute risk reduction in patients with higher baseline risk, with a 3.5% absolute risk reduction in kidney disease progression at 4 years in the highest risk group (≥1%/year). Results were similar with the 2022 Chronic Kidney Disease Prognosis Consortium risk prediction model.
Conclusions: Risk models for kidney disease progression can be applied in patients with T2D to stratify risk and identify those who experience a greater magnitude of benefit from SGLT2 inhibition.
期刊介绍:
The journal's overarching mission can be captured by the simple word "Care," reflecting its commitment to enhancing patient well-being. Diabetes Care aims to support better patient care by addressing the comprehensive needs of healthcare professionals dedicated to managing diabetes.
Diabetes Care serves as a valuable resource for healthcare practitioners, aiming to advance knowledge, foster research, and improve diabetes management. The journal publishes original research across various categories, including Clinical Care, Education, Nutrition, Psychosocial Research, Epidemiology, Health Services Research, Emerging Treatments and Technologies, Pathophysiology, Complications, and Cardiovascular and Metabolic Risk. Additionally, Diabetes Care features ADA statements, consensus reports, review articles, letters to the editor, and health/medical news, appealing to a diverse audience of physicians, researchers, psychologists, educators, and other healthcare professionals.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
