{"title":"血清富亮氨酸α 2糖蛋白在克罗恩病中的作用:小肠和结肠病变有区别吗?","authors":"Satohiro Matsumoto, Hirosato Mashima","doi":"10.1093/crocol/otad028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The usefulness of leucine-rich alpha 2 glycoprotein (LRG) to evaluate Crohn's disease (CD) activity differs among various intestinal lesions. We aimed to evaluate the association between endoscopic disease activity based on the Simple Endoscopic Score for Crohn's disease (SES-CD) and LRG level separately for small intestinal and colonic lesions.</p><p><strong>Methods: </strong>We examined the correlation between LRG level and SES-CD and performed receiver operating characteristic (ROC) analysis to determine the LRG cutoff value in 141 patients who underwent endoscopy (total 235 measurements). Furthermore, the LRG cutoff value was analyzed by comparing small intestinal and colonic lesions.</p><p><strong>Results: </strong>LRG levels were significantly higher in patients without mucosal healing than in those with mucosal healing (15.9 μg/mL vs 10.5 μg/mL, <i>P</i> < .0001). The LRG cutoff value for mucosal healing was 14.3 μg/mL (area under the ROC curve [AUC]: 0.80; sensitivity: 0.89; specificity: 0.63). The LRG cutoff value for patients with type L1 was 14.3 μg/mL (sensitivity: 0.91; specificity: 0.53), and that for patients with type L2 was 14.0 μg/mL (sensitivity: 0.95; specificity: 0.73). The diagnostic performance (AUC) of LRG and C-reactive protein (CRP) for mucosal healing was, respectively, 0.75 and 0.60 (<i>P</i> = 0.01) in patients with type L1 and 0.80 and 0.85 (<i>P</i> = 0.90) in patients with type L2.</p><p><strong>Conclusions: </strong>The optimal LRG cutoff value for evaluating mucosal healing in CD is 14.3 μg/mL. LRG is more useful than CRP for predicting mucosal healing in patients with type L1. The superiority of LRG to CRP differs between small intestinal and colonic lesions.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":null,"pages":null},"PeriodicalIF":1.8000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10243872/pdf/","citationCount":"0","resultStr":"{\"title\":\"Usefulness of Serum Leucine-rich Alpha 2 Glycoprotein in Crohn's Disease: Is There Any Difference between Small Intestine and Colonic Lesions?\",\"authors\":\"Satohiro Matsumoto, Hirosato Mashima\",\"doi\":\"10.1093/crocol/otad028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The usefulness of leucine-rich alpha 2 glycoprotein (LRG) to evaluate Crohn's disease (CD) activity differs among various intestinal lesions. We aimed to evaluate the association between endoscopic disease activity based on the Simple Endoscopic Score for Crohn's disease (SES-CD) and LRG level separately for small intestinal and colonic lesions.</p><p><strong>Methods: </strong>We examined the correlation between LRG level and SES-CD and performed receiver operating characteristic (ROC) analysis to determine the LRG cutoff value in 141 patients who underwent endoscopy (total 235 measurements). Furthermore, the LRG cutoff value was analyzed by comparing small intestinal and colonic lesions.</p><p><strong>Results: </strong>LRG levels were significantly higher in patients without mucosal healing than in those with mucosal healing (15.9 μg/mL vs 10.5 μg/mL, <i>P</i> < .0001). The LRG cutoff value for mucosal healing was 14.3 μg/mL (area under the ROC curve [AUC]: 0.80; sensitivity: 0.89; specificity: 0.63). The LRG cutoff value for patients with type L1 was 14.3 μg/mL (sensitivity: 0.91; specificity: 0.53), and that for patients with type L2 was 14.0 μg/mL (sensitivity: 0.95; specificity: 0.73). The diagnostic performance (AUC) of LRG and C-reactive protein (CRP) for mucosal healing was, respectively, 0.75 and 0.60 (<i>P</i> = 0.01) in patients with type L1 and 0.80 and 0.85 (<i>P</i> = 0.90) in patients with type L2.</p><p><strong>Conclusions: </strong>The optimal LRG cutoff value for evaluating mucosal healing in CD is 14.3 μg/mL. LRG is more useful than CRP for predicting mucosal healing in patients with type L1. The superiority of LRG to CRP differs between small intestinal and colonic lesions.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10243872/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otad028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Usefulness of Serum Leucine-rich Alpha 2 Glycoprotein in Crohn's Disease: Is There Any Difference between Small Intestine and Colonic Lesions?
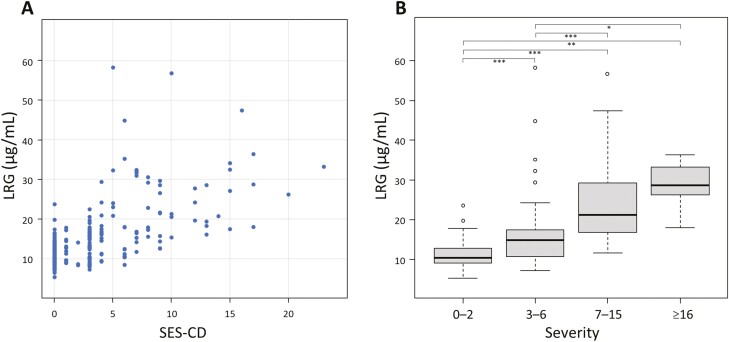
Background: The usefulness of leucine-rich alpha 2 glycoprotein (LRG) to evaluate Crohn's disease (CD) activity differs among various intestinal lesions. We aimed to evaluate the association between endoscopic disease activity based on the Simple Endoscopic Score for Crohn's disease (SES-CD) and LRG level separately for small intestinal and colonic lesions.
Methods: We examined the correlation between LRG level and SES-CD and performed receiver operating characteristic (ROC) analysis to determine the LRG cutoff value in 141 patients who underwent endoscopy (total 235 measurements). Furthermore, the LRG cutoff value was analyzed by comparing small intestinal and colonic lesions.
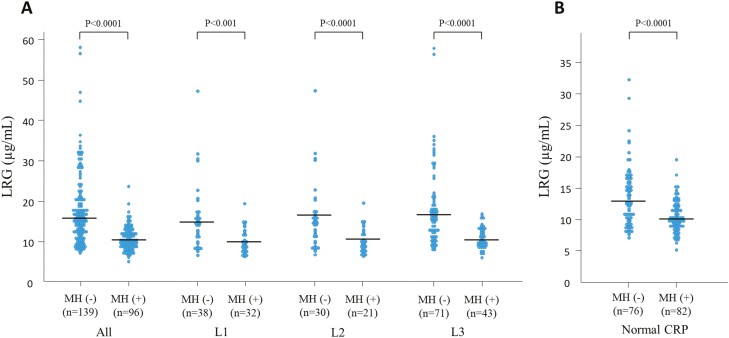
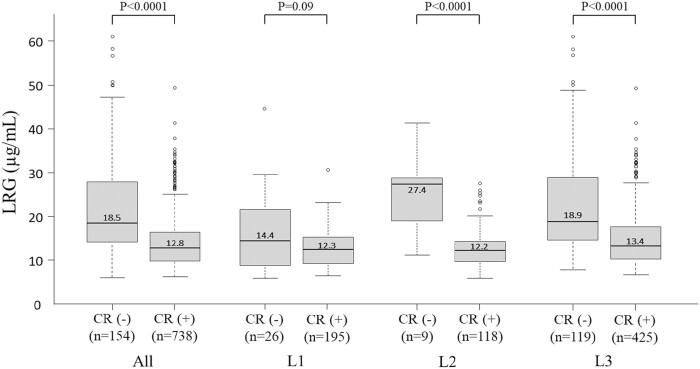
Results: LRG levels were significantly higher in patients without mucosal healing than in those with mucosal healing (15.9 μg/mL vs 10.5 μg/mL, P < .0001). The LRG cutoff value for mucosal healing was 14.3 μg/mL (area under the ROC curve [AUC]: 0.80; sensitivity: 0.89; specificity: 0.63). The LRG cutoff value for patients with type L1 was 14.3 μg/mL (sensitivity: 0.91; specificity: 0.53), and that for patients with type L2 was 14.0 μg/mL (sensitivity: 0.95; specificity: 0.73). The diagnostic performance (AUC) of LRG and C-reactive protein (CRP) for mucosal healing was, respectively, 0.75 and 0.60 (P = 0.01) in patients with type L1 and 0.80 and 0.85 (P = 0.90) in patients with type L2.
Conclusions: The optimal LRG cutoff value for evaluating mucosal healing in CD is 14.3 μg/mL. LRG is more useful than CRP for predicting mucosal healing in patients with type L1. The superiority of LRG to CRP differs between small intestinal and colonic lesions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
