Catherine Chioreso, Mary C Schroeder, Irena Gribovskaja Rupp, Eric Ammann, Knute D Carter, Charles F Lynch, Elizabeth A Chrischilles, Mary E Charlton
{"title":"Stage II/III Rectal Cancer Post-Treatment Surveillance Patterns of Care: A SEER- Medicare Study.","authors":"Catherine Chioreso, Mary C Schroeder, Irena Gribovskaja Rupp, Eric Ammann, Knute D Carter, Charles F Lynch, Elizabeth A Chrischilles, Mary E Charlton","doi":"10.19080/argh.2021.17.555972","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Despite high rectal cancer recurrence rates, knowledge on post-treatment surveillance utilization is limited. Hence, this study aims to estimate patterns of post-treatment surveillance and determine associated factors.</p><p><strong>Patients and methods: </strong>Retrospective study of 1,024 SEER-Medicare patients >65 years old diagnosed with stage II/III rectal cancer between 2007-2013. Logistic regression was used to determine factors associated with ≥1 colonoscopy, ≥2 physician visits, ≥2 carcinoembryonic antigen (CEA) tests and ≥2 computed tomographic colonography (CT) within 14 months after primary treatment.</p><p><strong>Results: </strong>Fifty-five percent had ≥1 colonoscopy, 54% had ≥2 physician visits, 47% had ≥2 CEA tests and 20% had ≥2 CTs. In multivariable logistic models, younger age and receipt of chemoradiation therapy (vs none) were significant across all surveillance procedures while clinical factors such as comorbidity were not. Being married (OR=1.69; 95% CI: 1.26-2.26) and proximity to a high-volume hospital (≤15 vs >30 minutes, OR=1.56; 95% CI: 1.00-2.43) were associated with ≥1 colonoscopy. Female gender (OR=1.56; 95% CI: 1.17-2.09), being married (OR=1.56; 95% CI: 1.17-2.08), white race (OR=1.79; 95% CI: 1.23- 2.62) and surgery from high-volume surgeon (OR=1.47; 95% CI: 1.06-2.04) were associated with ≥2 physician visits. Female gender (OR=1.45; 95% CI: 1.08-1.95), being married (OR=1.46; 95% CI: 1.08-1.96) and surgery from high-volume surgeon (OR=1.55; 95% CI: 1.10-2.17) had higher ≥2 CEA tests.</p><p><strong>Conclusions: </strong>Post-treatment surveillance remains low but is more common among younger patients and recipients of chemoradiation. Distinct profiles of patient characteristics and provider volume were associated with individual surveillance procedures suggesting the need for multicomponent strategies to increase surveillance.</p>","PeriodicalId":72074,"journal":{"name":"Advanced research in gastroenterology & hepatology","volume":"17 5","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10457021/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced research in gastroenterology & hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19080/argh.2021.17.555972","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Despite high rectal cancer recurrence rates, knowledge on post-treatment surveillance utilization is limited. Hence, this study aims to estimate patterns of post-treatment surveillance and determine associated factors.
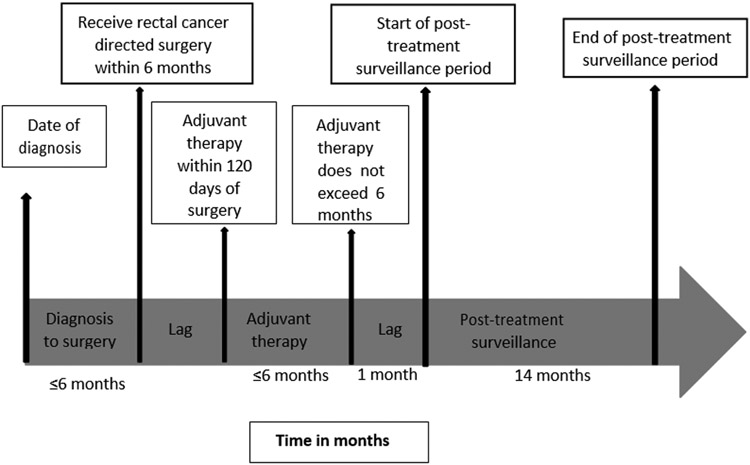
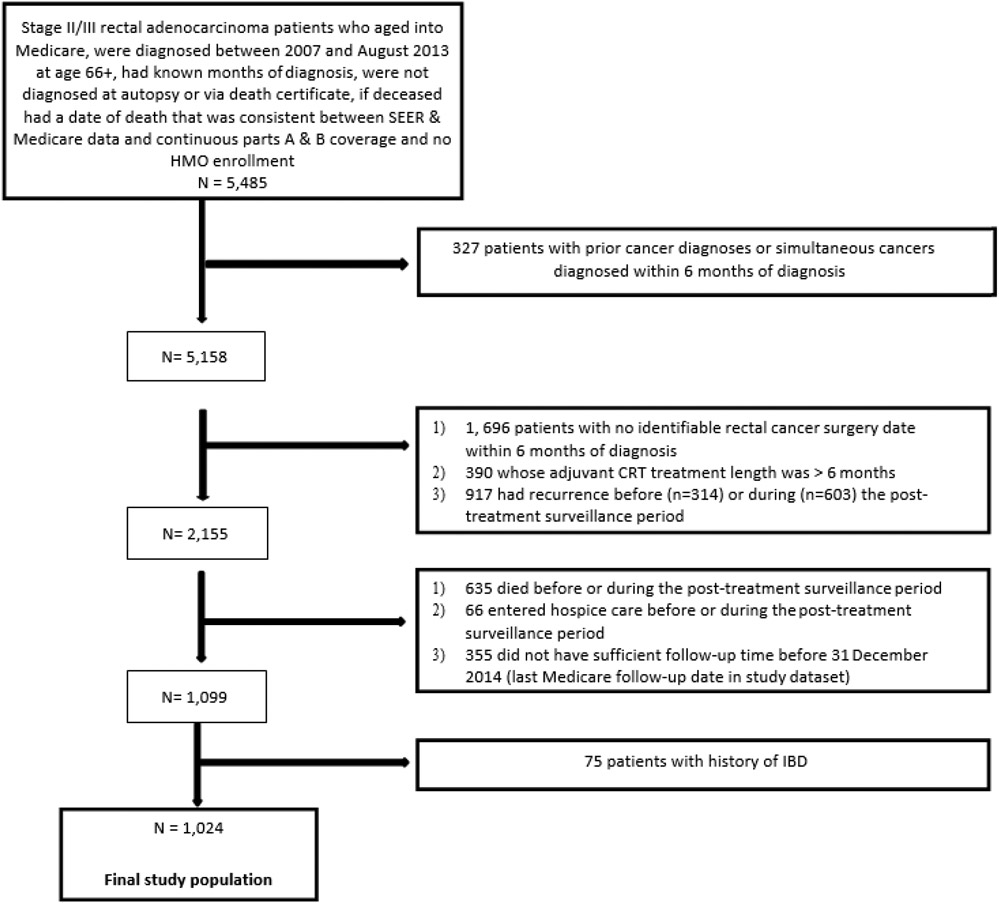
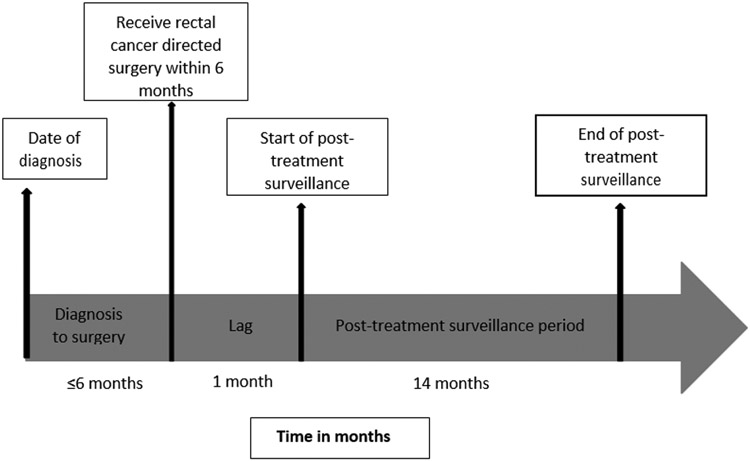
Patients and methods: Retrospective study of 1,024 SEER-Medicare patients >65 years old diagnosed with stage II/III rectal cancer between 2007-2013. Logistic regression was used to determine factors associated with ≥1 colonoscopy, ≥2 physician visits, ≥2 carcinoembryonic antigen (CEA) tests and ≥2 computed tomographic colonography (CT) within 14 months after primary treatment.
Results: Fifty-five percent had ≥1 colonoscopy, 54% had ≥2 physician visits, 47% had ≥2 CEA tests and 20% had ≥2 CTs. In multivariable logistic models, younger age and receipt of chemoradiation therapy (vs none) were significant across all surveillance procedures while clinical factors such as comorbidity were not. Being married (OR=1.69; 95% CI: 1.26-2.26) and proximity to a high-volume hospital (≤15 vs >30 minutes, OR=1.56; 95% CI: 1.00-2.43) were associated with ≥1 colonoscopy. Female gender (OR=1.56; 95% CI: 1.17-2.09), being married (OR=1.56; 95% CI: 1.17-2.08), white race (OR=1.79; 95% CI: 1.23- 2.62) and surgery from high-volume surgeon (OR=1.47; 95% CI: 1.06-2.04) were associated with ≥2 physician visits. Female gender (OR=1.45; 95% CI: 1.08-1.95), being married (OR=1.46; 95% CI: 1.08-1.96) and surgery from high-volume surgeon (OR=1.55; 95% CI: 1.10-2.17) had higher ≥2 CEA tests.
Conclusions: Post-treatment surveillance remains low but is more common among younger patients and recipients of chemoradiation. Distinct profiles of patient characteristics and provider volume were associated with individual surveillance procedures suggesting the need for multicomponent strategies to increase surveillance.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
