{"title":"Magnetic resonance imaging in COVID-19-associated acute invasive fungal rhinosinusitis - Diagnosis and beyond.","authors":"Gayatri Senapathy, Tharani Putta, Srinivas Kishore Sistla","doi":"10.25259/JCIS_46_2023","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of the study was to evaluate the magnetic resonance imaging (MRI) features of acute invasive fungal rhinosinusitis (AIFRS) at presentation and on follow-up imaging when patients receive treatment with systemic antifungal therapy and surgical debridement.</p><p><strong>Material and methods: </strong>This is a retrospective analysis of imaging data from a cohort of patients diagnosed with AIFRS during the second wave of COVID-19 in single tertiary referral hospital in South India between March 2021 and May 2021 (<i>n</i> = 68). Final diagnosis was made using a composite reference standard which included a combination of MRI findings, clinical presentation, nasal endoscopy and intraoperative findings, and laboratory proof of invasive fungal infection. Analysis included 62 patients with \"Definite AIFRS\" findings on MRI and another six patients with \"Possible AIFRS\" findings on MRI and laboratory proof of invasive fungal infection. Follow-up imaging was available in 41 patients.</p><p><strong>Results: </strong>The most frequent MRI finding was T2 hypointensity in the sinonasal mucosa (94%) followed by mucosal necrosis/loss of contrast-enhancement (92.6%). Extrasinosal inflammation with or without necrosis in the pre-antral fat, retroantral fat, pterygopalatine fossa, and masticator space was seen in 91.1% of the cases. Extrasinosal spread was identified on MRI even when the computed tomography (CT) showed intact bone with normal extrasinosal density. Orbital involvement (72%) was in the form of contiguous spread from either the ethmoid or maxillary sinuses; the most frequent presentation being orbital cellulitis and necrosis, with some cases showing extension to the orbital apex (41%) and inflammation of the optic nerve (32%). A total of 22 patients showed involvement of the cavernous sinuses out of which 10 had sinus thrombosis and five patients had cavernous internal carotid artery involvement. Intracranial extension was seen both in the form of contiguous spread to the pachymeninges over the frontal and temporal lobes (25%) and intra-axial involvement in the form of cerebritis, abscesses, and infarcts (8.8%). Areas of blooming on SWI were noted within the areas of cerebritis and infarcts. Perineural spread of inflammation was seen along the mandibular nerves across foramen ovale in five patients and from the cisternal segment of trigeminal nerve to the root exit zone in pons in three patients. During follow-up, patients with disease progression showed involvement of the bones of skull base, osteomyelitis of the palate, alveolar process of maxilla, and zygoma. Persistent hyperenhancement in the post-operative bed after surgical debridement and resection was noted even in patients with stable disease.</p><p><strong>Conclusion: </strong>Contrast-enhanced MRI must be performed in all patients with suspected AIFRS as non-contrast MRI fails to demonstrate tissue necrosis and CT fails to demonstrate extrasinosal disease across intact bony walls. Orbital apex, pterygopalatine fossa, and the cavernous sinuses form important pathways for disease spread to the skull base and intracranial compartment. While cerebritis, intracranial abscesses, and infarcts can be seen early in the disease due to the angioinvasive nature, perineural spread and skull base infiltration are seen 3-4 weeks after disease onset. Exaggerated soft-tissue enhancement in the post-operative bed after debridement can be a normal finding and must not be interpreted as disease progression.</p>","PeriodicalId":15512,"journal":{"name":"Journal of Clinical Imaging Science","volume":"13 ","pages":"23"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/75/54/JCIS-13-23.PMC10481822.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Imaging Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/JCIS_46_2023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The aim of the study was to evaluate the magnetic resonance imaging (MRI) features of acute invasive fungal rhinosinusitis (AIFRS) at presentation and on follow-up imaging when patients receive treatment with systemic antifungal therapy and surgical debridement.
Material and methods: This is a retrospective analysis of imaging data from a cohort of patients diagnosed with AIFRS during the second wave of COVID-19 in single tertiary referral hospital in South India between March 2021 and May 2021 (n = 68). Final diagnosis was made using a composite reference standard which included a combination of MRI findings, clinical presentation, nasal endoscopy and intraoperative findings, and laboratory proof of invasive fungal infection. Analysis included 62 patients with "Definite AIFRS" findings on MRI and another six patients with "Possible AIFRS" findings on MRI and laboratory proof of invasive fungal infection. Follow-up imaging was available in 41 patients.
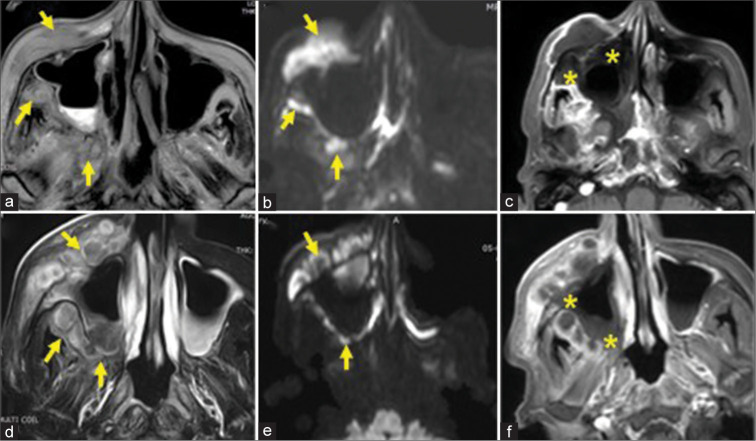
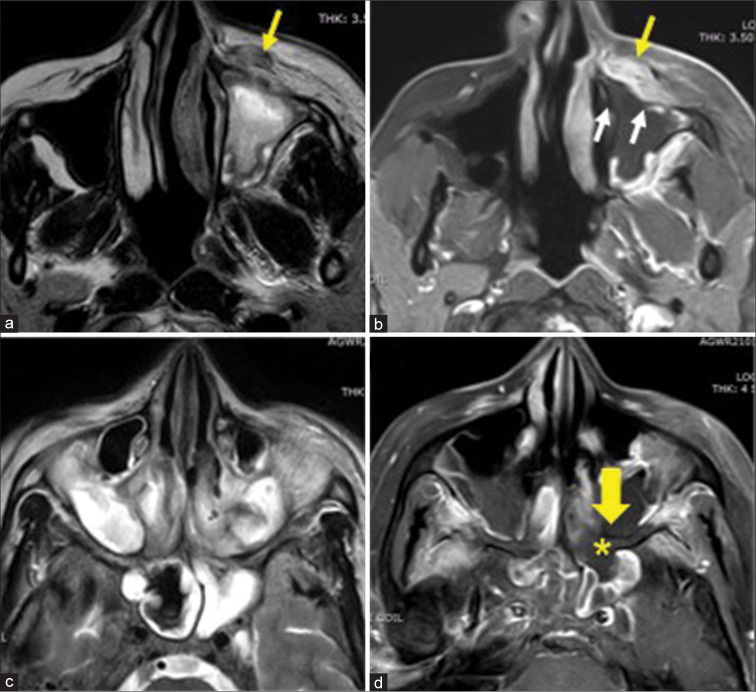
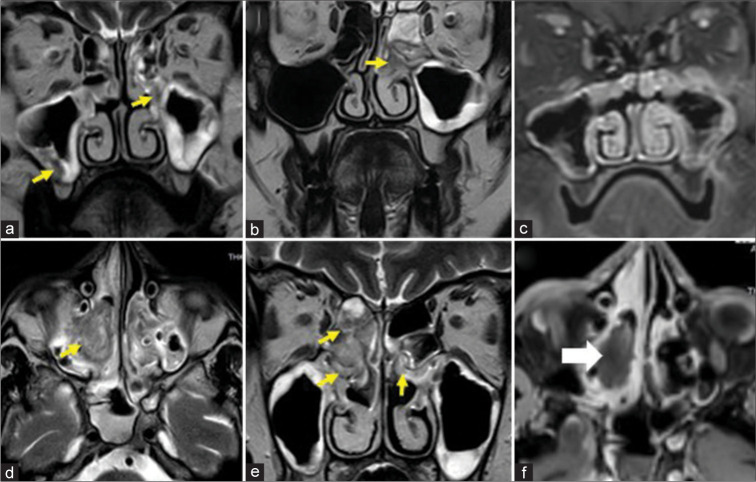
Results: The most frequent MRI finding was T2 hypointensity in the sinonasal mucosa (94%) followed by mucosal necrosis/loss of contrast-enhancement (92.6%). Extrasinosal inflammation with or without necrosis in the pre-antral fat, retroantral fat, pterygopalatine fossa, and masticator space was seen in 91.1% of the cases. Extrasinosal spread was identified on MRI even when the computed tomography (CT) showed intact bone with normal extrasinosal density. Orbital involvement (72%) was in the form of contiguous spread from either the ethmoid or maxillary sinuses; the most frequent presentation being orbital cellulitis and necrosis, with some cases showing extension to the orbital apex (41%) and inflammation of the optic nerve (32%). A total of 22 patients showed involvement of the cavernous sinuses out of which 10 had sinus thrombosis and five patients had cavernous internal carotid artery involvement. Intracranial extension was seen both in the form of contiguous spread to the pachymeninges over the frontal and temporal lobes (25%) and intra-axial involvement in the form of cerebritis, abscesses, and infarcts (8.8%). Areas of blooming on SWI were noted within the areas of cerebritis and infarcts. Perineural spread of inflammation was seen along the mandibular nerves across foramen ovale in five patients and from the cisternal segment of trigeminal nerve to the root exit zone in pons in three patients. During follow-up, patients with disease progression showed involvement of the bones of skull base, osteomyelitis of the palate, alveolar process of maxilla, and zygoma. Persistent hyperenhancement in the post-operative bed after surgical debridement and resection was noted even in patients with stable disease.
Conclusion: Contrast-enhanced MRI must be performed in all patients with suspected AIFRS as non-contrast MRI fails to demonstrate tissue necrosis and CT fails to demonstrate extrasinosal disease across intact bony walls. Orbital apex, pterygopalatine fossa, and the cavernous sinuses form important pathways for disease spread to the skull base and intracranial compartment. While cerebritis, intracranial abscesses, and infarcts can be seen early in the disease due to the angioinvasive nature, perineural spread and skull base infiltration are seen 3-4 weeks after disease onset. Exaggerated soft-tissue enhancement in the post-operative bed after debridement can be a normal finding and must not be interpreted as disease progression.
期刊介绍:
The Journal of Clinical Imaging Science (JCIS) is an open access peer-reviewed journal committed to publishing high-quality articles in the field of Imaging Science. The journal aims to present Imaging Science and relevant clinical information in an understandable and useful format. The journal is owned and published by the Scientific Scholar. Audience Our audience includes Radiologists, Researchers, Clinicians, medical professionals and students. Review process JCIS has a highly rigorous peer-review process that makes sure that manuscripts are scientifically accurate, relevant, novel and important. Authors disclose all conflicts, affiliations and financial associations such that the published content is not biased.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
