{"title":"Detection of SARS-CoV-2 RNA in exhaled breath and its potential for prevention measures","authors":"Madiha Malik, Thomas Kunze","doi":"10.1016/j.infpip.2023.100299","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>To propose infection prevention measures it is essential to understand the dynamics of SARS-CoV-2 shedding, particularly in asymptomatic patients. This report compares the viral load progression in exhaled breath (EB) with the symptom severity. We aim to evaluate the adequacy of symptom assessment regarding the infectivity level of individuals.</p></div><div><h3>Methods</h3><p>We observed infected patients since their first positive test during hospitalization. EB samples were collected on days 1, 3, 5, 7, 10, 12 and 14 of hospitalization using a filter-based device. After extraction, viral loads were quantified with qRT-PCR. The infection trajectory was documented after symptom onset.</p></div><div><h3>Case Presentation and Discussion</h3><p>A 34-year old patient showed mild symptoms, e.g. fever, cough, headache, muscle pain and loss of taste and smell across trajectory of infection (Case 1). The viral loads emitted via exhaling were nearly constant and ranged from 8.6 x 10<sup>3</sup> and 4.1 x 10<sup>4</sup> RNA copies per hour. After the infection, the patient developed a pneumonia. The second case of a 65-year old patient depicted an asymptomatic infection trajectory for 14 days after the first diagnosis (Case 2). Nevertheless, the patient exhaled up to 2 x 10<sup>5</sup> SARS-CoV-2 virus copies hourly, approximately 10 fold higher than measured for Case 1.</p></div><div><h3>Conclusion</h3><p>Symptomatic and asymptomatic COVID-19 patients exhale distinctive amounts of SARS-CoV-2 not necessarily correlating with symptom severity. Particularly, asymptomatic patients might show higher EB viral shedding. Therefore, EB testing should be included in infection prevention measures as it has high potential to reveal the most infectious individuals regardless of their symptoms during infection.</p></div>","PeriodicalId":33492,"journal":{"name":"Infection Prevention in Practice","volume":"5 3","pages":"Article 100299"},"PeriodicalIF":1.9000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/26/7c/main.PMC10374965.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection Prevention in Practice","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S259008892300032X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background
To propose infection prevention measures it is essential to understand the dynamics of SARS-CoV-2 shedding, particularly in asymptomatic patients. This report compares the viral load progression in exhaled breath (EB) with the symptom severity. We aim to evaluate the adequacy of symptom assessment regarding the infectivity level of individuals.
Methods
We observed infected patients since their first positive test during hospitalization. EB samples were collected on days 1, 3, 5, 7, 10, 12 and 14 of hospitalization using a filter-based device. After extraction, viral loads were quantified with qRT-PCR. The infection trajectory was documented after symptom onset.
Case Presentation and Discussion
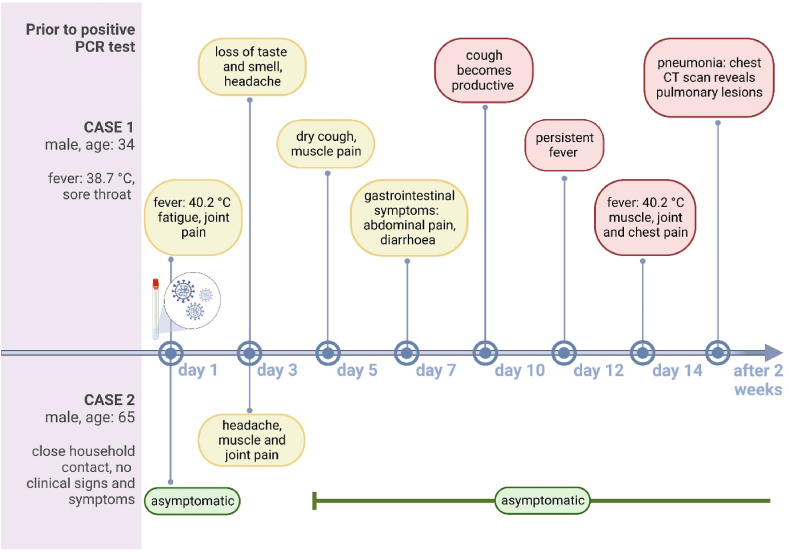
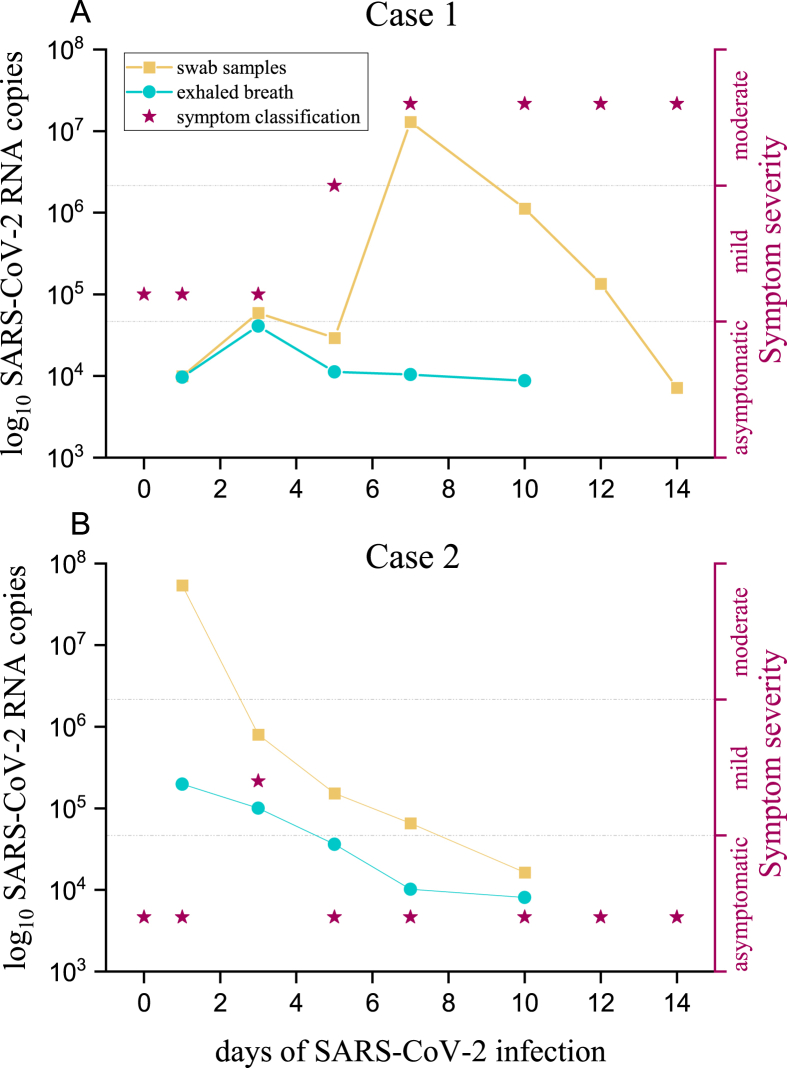
A 34-year old patient showed mild symptoms, e.g. fever, cough, headache, muscle pain and loss of taste and smell across trajectory of infection (Case 1). The viral loads emitted via exhaling were nearly constant and ranged from 8.6 x 103 and 4.1 x 104 RNA copies per hour. After the infection, the patient developed a pneumonia. The second case of a 65-year old patient depicted an asymptomatic infection trajectory for 14 days after the first diagnosis (Case 2). Nevertheless, the patient exhaled up to 2 x 105 SARS-CoV-2 virus copies hourly, approximately 10 fold higher than measured for Case 1.
Conclusion
Symptomatic and asymptomatic COVID-19 patients exhale distinctive amounts of SARS-CoV-2 not necessarily correlating with symptom severity. Particularly, asymptomatic patients might show higher EB viral shedding. Therefore, EB testing should be included in infection prevention measures as it has high potential to reveal the most infectious individuals regardless of their symptoms during infection.
背景:为了提出感染预防措施,了解严重急性呼吸系统综合征冠状病毒2型脱落的动态至关重要,尤其是在无症状患者中。本报告比较了呼气中病毒载量的进展与症状的严重程度。我们的目的是评估关于个体传染性水平的症状评估的充分性。方法:我们观察了感染患者在住院期间首次检测呈阳性后的情况。使用基于过滤器的设备在住院的第1、3、5、7、10、12和14天采集EB样本。提取后,用qRT-PCR对病毒载量进行定量。症状出现后记录感染轨迹。病例介绍和讨论:一名34岁的患者在感染过程中表现出轻微症状,如发烧、咳嗽、头痛、肌肉疼痛以及味觉和嗅觉丧失(病例1)。通过呼气释放的病毒载量几乎恒定,范围为每小时8.6 x 103和4.1 x 104个RNA拷贝。感染后,病人患上了肺炎。第二例65岁患者在首次诊断后14天内出现无症状感染轨迹(病例2)。尽管如此,患者每小时呼出多达2×105个SARS-CoV-2病毒拷贝,比病例1的测量值高出约10倍。结论:有症状和无症状的新冠肺炎患者呼出不同数量的SARS-CoV-2,不一定与症状严重程度相关。特别是,无症状患者可能表现出较高的EB病毒脱落。因此,EB检测应包括在感染预防措施中,因为它很有可能揭示最具传染性的个体,无论他们在感染期间的症状如何。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
