Anmol Shahid, Bonnie G Sept, Victoria S Owen, Corson Johnstone, Rameiya Paramalingam, Stephana J Moss, Rebecca Brundin-Mather, Karla D Krewulak, Andrea Soo, Jeanna Parsons-Leigh, Céline Gélinas, Kirsten M Fiest, Henry T Stelfox
{"title":"Preliminary clinical testing to inform development of the Critical Care Pain Observation Tool for Families (CPOT-Fam).","authors":"Anmol Shahid, Bonnie G Sept, Victoria S Owen, Corson Johnstone, Rameiya Paramalingam, Stephana J Moss, Rebecca Brundin-Mather, Karla D Krewulak, Andrea Soo, Jeanna Parsons-Leigh, Céline Gélinas, Kirsten M Fiest, Henry T Stelfox","doi":"10.1080/24740527.2023.2235399","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Many patients in the intensive care unit (ICU) cannot communicate. For these patients, family caregivers (family members/close friends) could assist in pain assessment. We previously adapted the Critical Care Pain Observation Tool (CPOT) for family caregiver use (CPOT-Fam). In this study, we conducted preliminary clinical evaluation of the CPOT-Fam to inform further tool development.</p><p><strong>Methods: </strong>For preliminary testing, we collected (1) pain assessments of patients in the ICU from family caregivers (CPOT-Fam) and nurses (CPOT) and determined the degree of agreement (kappa coefficient, κ) and (2) collected openended feedback on the CPOT-Fam from family caregivers. For refinement, we used preliminary testing data to refine the CPOT-Fam with a multidisciplinary working group.</p><p><strong>Results: </strong>We assessed agreement between family caregiver and nurse pain scores for 29 patients. Binary agreement (κ) between CPOT-Fam and CPOT item scores (scores ≥2 considered indicative of significant pain) was fair, κ = 0.43 (95% confidence interval [CI] 0.18-0.69). Agreement was highest for the CPOT-Fam items ventilator compliance/vocalization (weighted κ = 0.48, 95% CI 0.15-0.80) and lowest for muscle tension (weighted κ = 0.10, 95% [CI] -0.17 to 0.20). Most participants (<i>n</i> = 19; 69.0%) reported a very positive experience using the CPOT-Fam, describing it as \"good\" and \"easy-to-use/clear/straightforward.\" We iteratively refined the CPOT-Fam over five cycles using the data collected until no further revisions were suggested.</p><p><strong>Conclusion: </strong>Our preliminary clinical testing suggests that family involvement in pain assessment in the ICU is well perceived. The CPOT-Fam has been further refined and is now ready for clinical pilot testing to determine its feasibility and acceptability.</p>","PeriodicalId":53214,"journal":{"name":"Canadian Journal of Pain-Revue Canadienne de la Douleur","volume":"7 2","pages":"2235399"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10503446/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Pain-Revue Canadienne de la Douleur","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/24740527.2023.2235399","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Many patients in the intensive care unit (ICU) cannot communicate. For these patients, family caregivers (family members/close friends) could assist in pain assessment. We previously adapted the Critical Care Pain Observation Tool (CPOT) for family caregiver use (CPOT-Fam). In this study, we conducted preliminary clinical evaluation of the CPOT-Fam to inform further tool development.
Methods: For preliminary testing, we collected (1) pain assessments of patients in the ICU from family caregivers (CPOT-Fam) and nurses (CPOT) and determined the degree of agreement (kappa coefficient, κ) and (2) collected openended feedback on the CPOT-Fam from family caregivers. For refinement, we used preliminary testing data to refine the CPOT-Fam with a multidisciplinary working group.
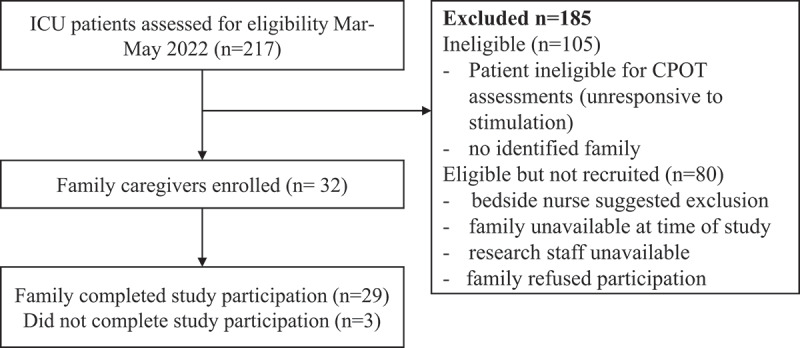
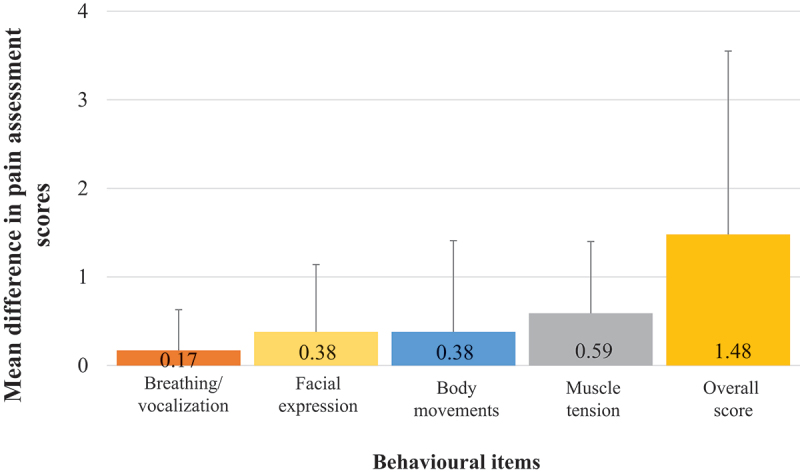
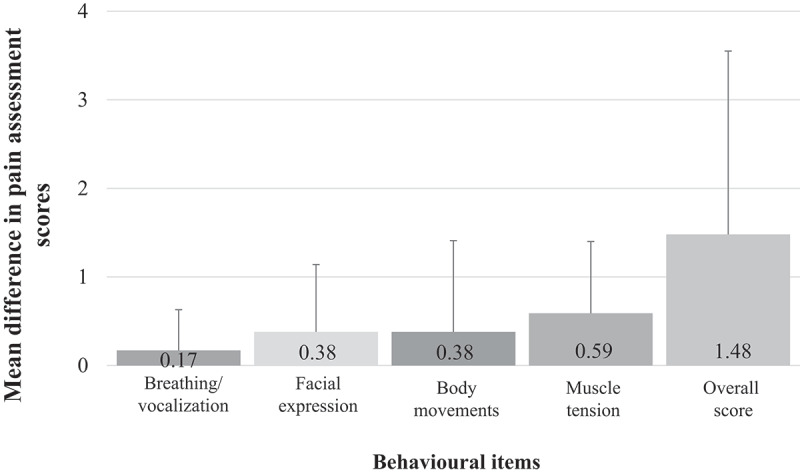
Results: We assessed agreement between family caregiver and nurse pain scores for 29 patients. Binary agreement (κ) between CPOT-Fam and CPOT item scores (scores ≥2 considered indicative of significant pain) was fair, κ = 0.43 (95% confidence interval [CI] 0.18-0.69). Agreement was highest for the CPOT-Fam items ventilator compliance/vocalization (weighted κ = 0.48, 95% CI 0.15-0.80) and lowest for muscle tension (weighted κ = 0.10, 95% [CI] -0.17 to 0.20). Most participants (n = 19; 69.0%) reported a very positive experience using the CPOT-Fam, describing it as "good" and "easy-to-use/clear/straightforward." We iteratively refined the CPOT-Fam over five cycles using the data collected until no further revisions were suggested.
Conclusion: Our preliminary clinical testing suggests that family involvement in pain assessment in the ICU is well perceived. The CPOT-Fam has been further refined and is now ready for clinical pilot testing to determine its feasibility and acceptability.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
