Growth of GL261 glioblastoma tumours induced delayed body weight gain and stunted skeletal muscle growth in paediatric mice
Joshua R. Huot1, Nicholas A. Jamnick2, Patrick D. Livingston2, Fabrizio Pin1 and Andrea Bonetto2
1Department of Anatomy, Cell Biology & Physiology, Indiana University School of Medicine, Indianapolis, IN, USA;2Department of Pathology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Introduction: Up to 80% of adult cancer patients will develop involuntary body weight loss associated with skeletal muscle wasting, which altogether lead to increased morbidity and mortality. However, there is minimal understanding or research on the influence of paediatric cancers on muscle development and physiology. Given that brain tumours alone are responsible for 1/4 of all paediatric cancers, the aim of the current research was to investigate the skeletal muscle consequences associated with growth of these tumours in young mice.
Methods:In vitro atrophy was assessed by co-culturing C2C12 myotubes with GL261 murine glioblastoma cells. GL261 cells (1.0 × 106) were injected subcutaneously into 4-week-old male C57BL/6J mice. Body mass was monitored daily. Vehicle (n = 5) and experimental mice (n = 14) were culled 28 days after GL261 implantation. Skeletal muscle and organ weights were measured at the completion of the study. Muscle cross sectional area (CSA) was assessed via immunofluorescent stain of dystrophin. In vivo and ex vivo muscle function testing was completed at baseline and prior to completion of the study. Muscle protein synthesis was measured via the SUnSET method, and gene expression via qPCR.
Results: C2C12 cells exposed to GL261 exhibited myotube atrophy. Carcass, heart, and fat mass were mitigated (P < 0.05) in the tumour bearers, whereas growth of skeletal muscles (tibialis anterior and quadriceps) was impeded in the GL261 hosts (P < 0.05), in line with significantly lower muscle fibre cross sectional (P < 0.05). In vivo gastrocnemius torque was not significantly different between groups, while the ex vivo EDL muscle force was reduced in the GL261 hosts (P < 0.05). Tumour hosts displayed reduced muscle protein synthesis (P < 0.05). MuRF-1, MUSA1 and Atrogin1 muscle ubiquitin ligase mRNA expression was lower in the GL261 hosts.
Conclusions: Our research highlights the impact of GL261 glioblastoma on paediatric mice. GL261 hosts yielded a stunted development of skeletal muscle, as evidenced by decreased skeletal muscle mass, smaller muscle fibre CSA, diminished muscle protein synthesis, and reduced cell signalling associated with protein catabolism. Future research should focus on the mechanisms responsible for the systemic long-term effects of cancer in paediatric patients and investigate potential therapeutic targets to mitigate the blunted muscle development.
1-02
Sexual dimorphism in the development of cancer cachexia in ApcMin/+ mice
Bénédicte Guegan1, Anne-Cécile Durieux1, Esra Elmali1, Valentine Allibert1, Benjamin Buhot1,2, Christophe Hourde3, Julien Gondin4 and Damien Freyssenet1
1Université Jean Monnet Saint-Etienne, Laboratoire Interuniversitaire de Biologie de la Motricité, Saint Etienne, France;2Neurochirurgie, Centre Hospitalier Universitaire de Saint Etienne, Saint Etienne, France;3Université Savoie Mont Blanc, Laboratoire Interuniversitaire de Biologie de la Motricité, Chambéry, France;4Institut NeuroMyoGène - UMR CNRS 5310 – INSERM U1217, Université Claude Bernard Lyon 1, Villeurbanne, France
Introduction: Cancer cachexia is a devastating hypo-anabolic and catabolic syndrome characterized by a progressive unintentional loss of body mass, essentially due to a severe depletion of skeletal muscle compartment. Despites extensive studies over the last decade, little is known about the effects of sex and sex hormones on the development of cancer cachexia. Here, we determined whether the progression of cancer cachexia was different in male and female ApcMin/+ mice, a model of intestinal and colon cancer cachexia that mimics the human adenomatous polyposis.
Methods: Male and female ApcMin/+ mice aged of 11 and 15 weeks have been analysed for body weight, the extent of polyposis, body composition (X-ray technology Lunar PIXImus), muscle weights and muscle force (Aurora Scientific). Age- and sex-matched wild type littermate mice were used as controls.
Results: The number of polyps (27 ± 9.8 in male vs. 27.8 ± 3.2 in female) as well as the haematocrit (35.7 ± 2.5 in male vs. 40.6 ± 2.4 in female), were similar in 15-week-old ApcMin/+ mice, indicating no sex difference in the development of the polyposis. Male ApcMin/+ mice started to lose weight at 12 weeks (−9%, P < 0.05). At the age of 15 weeks, muscle weight loss was about 16% (P < 0.001). By contrast, body weight was not statistically significant between wild type and ApcMin/+ female mice. This was also associated with a better preservation of fat mass and bone mineral density in female ApcMin/+ mice. Gastrocnemius muscle weight was also lowered in 15-week-old (−10%, P < 0.001) male ApcMin/+ mice compared to wild type male mice, whereas it was unchanged between female genotypes. Similar results were obtained for extensor digitorum longus, quadriceps, soleus, and tibialis anterior muscle weights. Functionally, maximum muscle force, which was lowered in 15-week-old male ApcMin/+ mice compared to wild type male mice (−22.5%, P < 0.05) was similar between female genotypes.
Conclusions: These data indicate that that while the progression of the disease per se seems to be the same in males and females ApcMin/+ mice, 15-week-old female ApcMin/+ mice display resistance to the development of cancer cachexia, clearly indicating the existence of a sexual dimorphism. Ongoing analyses will provide information to understand the molecular mechanisms involved in sexual dimorphism.
1-03
Metabolic dysfunction during recovery from colorectal cancer chemotherapy: a role for skeletal muscle AMPK signalling
Jessica Halle1, Quan Zhang1, Hector Paez2, Stephen Alway2 and James Carson1
1Integrative Muscle Biology Laboratory, Division of Regenerative and Rehabilitation Sciences, College of Health Professions, University of Tennessee Health Science Center, Memphis, TN, USA;2Laboratory of Muscle Biology and Sarcopenia, Division of Regenerative and Rehabilitation Sciences, College of Health Professions, University of Tennessee Health Science Center, Memphis, TN, USA
Introduction: The FOLFOX (5-fluorouracil, leucovorin, oxaliplatin) chemotherapy regimen is used to treat colorectal cancer and can induce acute metabolic dysfunction. While skeletal muscle loss can negatively regulate systemic metabolism, gaps remain in our understanding of how changes in the biochemical properties of muscle contribute to long-lasting chemotherapy toxicities. We investigated the effects of FOLFOX chemotherapy on systemic and skeletal muscle metabolism in mice and the direct effects of FOLFOX on AMPK and autophagy flux in cultured myotubes.
Methods: Male C57BL6/J (12 weeks) completed four cycles of FOLFOX or PBS treatment. Chemotherapy recovery was examined at 0 (n = 8), 4 (n = 11), or 10 weeks (n = 8–13) after the fourth chemotherapy cycle. Metabolic measurements were done in CLAMs cages for 5-days. C2C12 myotubes were dosed with FOLFOX for 24-hrs. Bafilomycin A1 (100 nM) and protein expression of LC3B and p62 were used to assess autophagy flux.
Results: FOLFOX attenuated body and fat mass accretion independent of lean mass, cage activity, or food intake. Fat mass remained reduced at 4-week recovery. Acute FOLFOX decreased oxygen consumption (VO2), energy expenditure (EE), carbohydrate (CHO), and lipid oxidation (P < 0.01). Deficits in VO2 and EE remained at 10-week recovery. CHO oxidation was reduced at 4 weeks but returned to control levels at 10-week recovery. FOLFOX significantly decreased soleus (−29%, P = 0.01) and plantaris (−26%, P = 0.03) muscle COXIV enzyme activity. Acute FOLFOX reduced gastrocnemius muscle AMPK (T172) (−25%, P = 0.03) and ULK1 (S555) (−40%, P = 0.01) phosphorylation and LC3B-II protein expression (−43%, P = 0.02). The LC3B-II/I ratio was positively correlated to CHO oxidation (r = 0.75, P = 0.03) in FOLFOX mice. Recovery for 4 weeks normalized muscle AMPK and ULK1 phosphorylation. FOLFOX treatment exerted direct effects on cultured myotubes; AMPK (T172) phosphorylation was reduced (−42%, P < 0.01). Interestingly, FOLFOX administration suppressed myotube autophagy flux (P < 0.01).
Conclusions: FOLFOX chemotherapy disrupted systemic metabolism, which did not recover after cessation of chemotherapy. Interestingly, FOLFOX-induced disruptions to muscle AMPK and autophagy signalling improved independent of systemic metabolism deficits. The activation of AMPK signalling during chemotherapy treatment warrants further investigation as a therapeutic target to prevent chemotherapy toxicities.
Funding: NCI R21 CA231131-01A1 to JA Carson.
1-04
Kidney-specific Tsc1−/− mice as renal cell carcinoma-induced cachexia model
Sara Clerici3, Suvham Barua1, Michella Ferrara3, Elia Angelino1,2, Lorenza Bodo1, Daniela Talarico3, Alessandra Boletta3 and Andrea Graziani1,2
1Molecular Biotechnology Center ‘Guido Tarone’, Department Molecular Biotechnologies and Health Sciences, University of Turin, Turin, Italy;2Department of Translational Medicine, University of Piemonte Orientale, Novara, Italy;3Division of Genetics and Cell Biology, IRCCS, San Raffaele Scientific Institute, Milan, Italy
Introduction: Cachexia is a major determinant of poor quality of life of cancer patients, and among the most frequent cause of death. Renal cell carcinoma (RCC), both localized and metastatic, is frequently associated to cachexia, being a strong prognostic factor for poor outcome. However, no genetic or orthotopic models are available to investigate RCC-induced cachexia. In this study, we aimed to characterize the cachectic phenotype of kidney-specific Tsc1−/− mice (Tsc1flox/flox: KspCre), a newly generated RCC genetic model (Drusian, Cell Report, 2018).
Methods: Tsc1f/f:KspCre mice were generated as described by Drusian et al (Cell Report, 2018). In vivo, mice cachectic phenotype was analysed at post-natal 50 days (p50) and 80 days (p80) by measuring (i) body weight, (ii) weight of tibialis anterior, gastrocnemius and quadriceps, (iii) gastrocnemius cross-sectional area, (iv) cachexia and muscle wasting-related gene expression by quantitative RT-PCR. In vitro, c2c12 myotubes diameter, mTORC1 signalling and STAT3 and NFkB transcriptional activities were measured upon incubation with tumour conditioned medium (TCM) from p50 and p80 Tsc1−/− mice kidney tumours.
Results: Renal cell carcinoma driven by Kidney-specific Tsc1 inactivation drives a cachectic phenotype at a very early stage p50 and p80, when the tumour mass starts to be detectable at histological level. Cachexia was measured by muscle mass, cross-sectional area and induction of cachexia related genes. Moreover, cachectic phenotype is reproduced in in vitro upon c2c12 myotubes incubation with tumour conditioned medium (TCM) from either p50 or p80 tumours.
Conclusions: Kidney-specific Tsc1−/− mice provides a novel genetically engineered mouse model (GEMM) for cachexia-induced by renal cell carcinoma cancer cachexia in mice. The high penetrance and rapid cachexia development makes this model highly suitable to address mechanistic issues specifically related to the onset of kidney cancer cachexia.
1-05
Hepatic metabolism alterations and effects of niacin supplementation in experimental cancer- and chemotherapy-induced cachexia
Natalia Cortez1, Yuki Nakamura2, Fabien Riols3, Marc Beltrà4, Mark Haid3, Shinpei Kawaoka2 and Fabio Penna1
1Department of Clinical and Biological Sciences, University of Turin, Turin, Italy;2Institute for Life and Medical Sciences, Kyoto University, Kyoto, Japan;3Metabolomics & Proteomics Core, Helmholtz Zentrum München, Munich, Germany;4Complex Metabolic Diseases and Mitochondria group, Institute for Research in Biomedicine, Barcelona, Spain
Introduction: Alterations in hepatic function influence energy expenditure in cancer patients and could play an important role in the development and progression of cancer cachexia, a progressive metabolic syndrome that results in depletion of skeletal muscle [1,2]. In cachectic mice, niacin (NA) supplementation ameliorated cancer- and chemotherapy-induced cachexia while repleting hepatic NAD metabolite levels, suggesting that a relevant part of the NA effects may be mediated by the improvement of liver metabolism [3]. Therefore, the objective of this project was to evaluate the differences in the liver metabolism of healthy mice and cancer/chemotherapy cachectic mice with or without niacin supplementation.
Methods: Two in vivo experiments were performed and compared with healthy controls. First, for an acute model of cachexia, female tumour-bearing C26 mice (n = 7/group) were treated with chemotherapy (Folfox) and either treated daily with 150 mg/kg niacin (C26 + F + NA) or given water (C26 + F). Second, for a chronic model of cachexia, Msh2 loxP/loxP Villin-Cre (VCM) 12-month-old male mice (n = 6/group) were either treated with a daily dose of NA or non-treated. Liver samples were lysed and processed to isolate high-quality RNA, RNA-seq libraries were generated, and sequencing experiments were performed. Lipidyzer technology was used to quantify lipid species in the liver.
Results: Diverse fatty acid, energy, immune, and NAD metabolism gene sets were impacted in tumour bearing mice when compared to healthy controls, plus enrichments profiles differed between the cachectic groups supplemented with NA and those not supplemented. Moreover, the acute and the chronic cachexia models showed distinct hepatic gene expression profiles. Importantly, when comparing tumour bearing mice per cachexia model, gene sets associated to NAD metabolism were impacted by NA supplementation in the VCM mice, but not in the C26. Additionally, the lipidomic analysis demonstrated that hepatic lipid composition was also altered in tumour bearing mice with either acute or chronic cachexia when compared to controls, plus that lipid profiles change with NA repletion.
Conclusions: Our preliminary results indicate that in both acute and chronic models of cancer cachexia, gene expression and lipid metabolism profiles are altered in the liver, and that niacin supplementation has an impact in such changes. Further studies are needed to better understand the effects of such hepatic metabolic changes in different stages of cancer cachexia and the potential benefits of niacin supplementation, while also considering the impact of sex, age, and chemotherapy.
The effects of a novel long-acting ghrelin on ameliorating cancer cachexia in mice
Haiming L. Kerr1, Kora Krumm1, Ian (In-gi) Lee1, Barbara Anderson1, Anthony Christiani1, Lena Strait1, Beatrice A. Breckheimer1, Brynn Irwin1, Alice (Siyi) Jiang1, Artur Rybachok1, Amanda Chen1, Lucas Caeiro1, Elizabeth Dacek1, Daniel B. Hall2, Caroline H. Kostyla2,3, Laura M. Hales2, Tarik M. Soliman2 and Jose M. Garcia1
1Geriatric Research, Education and Clinical Center, Veterans Affairs Puget Sound Health Care System, Gerontology and Geriatric Medicine, University of Washington Department of Medicine, Seattle, WA, USA;2Extend Biosciences, Inc., Newton, MA, USA;3Current affiliation: Atalanta Therapeutics, Boston, MA, USA
Introduction: Ghrelin has been investigated as a potential therapy for cachexia because of its orexigenic and anabolic effects on protecting against weight and muscle loss. However, its clinical application is limited due to its short half-life (~11 min in humans). EXT418 is a novel long-acting, constitutively active ghrelin analogue created by covalently linking it to a vitamin D derivative. To evaluate the effects of EXT418 on cancer cachexia and elucidate the underlying mechanisms, we evaluated this compound in a cancer cachexia model in mice induced by Lewis lung carcinoma (LLC).
Methods: Adult male C57BL/6J mice were implanted with 1 × 106 heat-killed (HK) or live LLC cells subcutaneously. After ~7 days, when the tumour was palpable, mice were treated with vehicle (T + V) or EXT418 daily (T + 418 Daily, 0.25 mg/kg/day) or every other day (T + 418 EOD, 0.5 mg/kg/EOD) for up to 14 days, while HK-treated mice were given vehicle (HK + V). Subsets of T + 418 Daily or EOD-treated mice were pair-fed to the T + V group. Body composition and grip strength were assessed at baseline (before tumour implantation) and at the end of the experiment. Skeletal muscles were collected after euthanasia and used for molecular analysis. Statistical analysis was performed by one-way ANOVA or Kruskal-Wallis tests to detect differences between groups (P < 0.05).
Results: LLC tumour led to significant decreases in food intake, body weight, fat mass, lean body mass, and grip strength in mice. Administration of EXT418 daily or EOD prevented these decreases in weight and muscle strength, which was partially independent of food intake. Fibre size in tibialis anterior muscles was improved by EXT418 daily administration, and IIB fibre size in red gastrocnemius muscles was improved by EXT418 EOD in tumour-bearing animals. In skeletal muscles, EXT418 administration with both schedules attenuated tumour-induced increases in atrogenes (Fbxo32 and Trim63) and the gene level of IL-6, which were independent of food intake. A similar pattern of inflammatory markers IL-6 in adipose tissue and IL-10 in circulation was observed but the modification from EXT418 was not significant. Tumour-induced increases in mitophagy markers (Bnip3 and p62) in skeletal muscles were also attenuated by EXT418 EOD and/or daily. Meanwhile, tumour size was not altered by either of the EXT418 treatment.
Conclusions: EXT418 protects against LLC-induced cachexia by reducing skeletal muscle inflammation, proteolysis, and mitophagy without affecting tumour mass and is partially independent of food intake.
1-07
Sex differences in amino acid metabolism is linked to cachexia outcomes in mice treated with chemotherapy drugs
Olasunkanmi A.J. Adegoke and Stephen Mora
School of Kinesiology and Health Science, Muscle Health Research Centre, York University, Toronto, Canada
Introduction: Cachexia is a body and skeletal muscle-wasting syndrome that affects ~80% of cancer patients. Given the differences in physiology between the sexes, it is likely that the severity and contributors to cachexia are different between the sexes. Although negative effects of chemotherapy on skeletal muscle are documented, the majority of the studies were completed in male animals.
Branched-chain amino acids (BCAA: leucine, isoleucine, and valine) activate anabolic signalling in skeletal muscle. While BCAA may mitigate some measures of cachexia, BCAA nutritional support does not fully reverse cachexia. This may be related to altered metabolism of these amino acids in cachexia, a subject that has been little studied. The objective of this study is to compare the effects of chemotherapy on cachexia outcomes and BCAA metabolism in male and female mice.
Methods: Three-month-old CD2F1 male and female mice were treated with either the chemotherapy drug combination folfiri (50 mg/kg 5-fluorouracil (5FU), 90 mg/kg Leucovorin, and 24 mg/kg CPT11, (drug)) or vehicle for 6 weeks.
Results: Between sexes, drug-treated female mice lost more body (−15%) and gastrocnemius muscle (−30%) weights compared to drug-treated males (−10% and −19%, respectively; P < 0.05). Consistent with these, drug-treated females showed greater loss of anabolic signalling compared to males. Greater reductions were seen in muscle BCAA concentrations in male (−53% to −74%) compared to female (−27% to −41% (P < 0.05). This was especially so for valine whose level was reduced by ~75% in male but by <30% in female. This correlated with greater reductions in muscle LAT1 (the BCAA transporter), but not in SNAT1, in female treated with the drugs compared to male (55% vs. 40%, P > 0.05). Conversely, plasma levels of BCAA were increased by 60% and concentrations in liver by >100% in male but with much smaller changes in females (no change in plasma, ~45% increase in liver in female). Among the key enzymes involved in BCAA metabolism, the inhibitory phosphorylation of branched-chain alpha-ketoacid dehydrogenase complex (BCKD) tended to be greater in drug-treated male animals. Although BCKD activity was higher in drug-treated animals, no significant sex differences were observed.
Conclusions: Our data suggest a link between body/muscle wasting and decreased BCAA metabolism during chemotherapy, and that these differences are likely regulated at the level of amino acid transport. Interventions that seek to mitigate cachexia need to consider these sex-related changes.
1-08
Unravelling the mechanisms of muscle atrophy: focus on lipocalin 2 and iron homeostasis
Elisabeth Wyart and Myriam Hsu and Erica Mina and Alessio Menga and Paolo E. Porporato
Department of Molecular Biotechnology and Health Sciences, Molecular Biotechnology Center, University of Torino, Turin, Italy
Introduction: Cachexia is a wasting syndrome characterized by severe skeletal muscle atrophy that substantially increases mortality in various diseases. The mechanism of cancer-induced cachexia is still poorly understood, highlighting the need for effective treatment. We previously identified major alterations of iron metabolism in the skeletal muscle of tumour-bearing mice and in particular a decrease in mitochondrial iron, resulting in mitochondrial dysfunction. However, the underlying causes of these alterations in muscle iron metabolism remain unknown. Lipocalin 2 (LCN2), an iron-sequestering protein, has been identified as one of the most upregulated genes in various models of skeletal muscle atrophy. Therefore, we investigated the role of LCN2 in skeletal muscle atrophy associated with cancer and chronic glucocorticoid treatment.
Materials and Methods: We analysed iron metabolism and muscle LCN2 expression both in the cancer-cachexia C26 model and in glucocorticoid-induced atrophy in vivo. To gain a better understanding about the role played by LCN2 in skeletal muscle atrophy, we silenced and overexpressed LCN2 in C2C12-derived myotubes and assessed myotubes diameter, atrophy markers, mitochondrial iron, and the expression of iron-related proteins.
Results: We observed a dramatic increase of LCN2 in the skeletal muscle of both C26 tumour-bearing and dexamethasone-treated mice. In vitro experiments showed that LCN2 overexpression decreased the diameter of C2C12 myotubes while silencing of LCN2 protected myotubes from dexamethasone-induced atrophy, confirming the implication of LCN2 in the atrophic process. In vivo, we found that aminoglutethimide, a drug inhibiting glucocorticoids synthesis, suppressed LCN2 expression in the skeletal muscle of C26 tumour-bearing mice thus suggesting that elevated levels of glucocorticoids are responsible for the upregulation of LCN2 in the C26 model. Additionally, treatment with dexamethasone both in vitro and in vivo led to a significant decrease in mitochondrial iron levels which mirrored the alterations in iron metabolism observed in the C26 model.
Conclusions: Overall, our findings provide new mechanistic insights in both cancer-induced and glucocorticoid-induced skeletal muscle wasting and support targeting lipocalin 2 as a potential therapeutic option for muscle wasting diseases.
1-09
Exploring the lived experience of cachexia for individuals with end-stage kidney disease and the interrelated experience of their carers
Carolyn Blair1, Adrian Slee2, Andrew Davenport3, Denis Fouque4, William Johnston5, Kamyar Kalantar-Zadeh6, Peter Maxwell7, Clare McKeaveney1, Robert Mullan8, Helen Noble1, Sam Porter9, David Seres10, Joanne Shields11, Ian Swaine12, Miles Witham13 and Joanne Reid1
1School of Nursing and Midwifery, Queen's University Belfast, Belfast, UK;2Division of Medicine, Faculty of Medical Sciences, University College London, London, UK;3UCL Department of Renal Medicine Royal Free Hospital, University College London, London, UK;4Division of Nephrology, Dialysis and Nutrition, Hôpital Lyon Sud and University of Lyon, Lyon, France;5Northern Ireland Kidney Patients Association, Belfast, UK;6Irvine Division of Nephrology, Hypertension and Kidney Transplantation, University of California, Irvine, CA, USA;7Centre for Public Health, Queen's University Belfast, Belfast, UK;8Renal Unit, Antrim Area Hospital, Northern Health & Social Care Trust, Belfast, UK;9Department of Social Sciences and Social Work, Bournemouth University, Bournemouth, UK;10Institute of Human Nutrition and Department of Medicine, Columbia University Irving Medical Center, Columbia, New York, USA;11Regional Nephrology Unit, Belfast City Hospital, Belfast Health & Social Care Trust, Belfast, UK;12School of Human Sciences, University of Greenwich, London, UK;13AGE Research Group, NIHR Newcastle Biomedical Research Centre, Campus for Ageing and Vitality, Newcastle upon Tyne, UK
Introduction: Cachexia is an important consideration in the person-centred care that is needed in end-stage kidney disease (ESKD). However, given that clinical guidelines relating to cachexia in ESKD are largely absent, this is an unmet care need. To inform guidelines and future ESKD service planning, there is an urgent need to understand individuals' experiences of cachexia in ESKD and the interrelated impacts on carers in their lives.
Methods: A purposive sampling strategy is being used to recruit individuals living with ESKD who have cachexia and their carers (n = 12) across two nephrology directorates, within two healthcare trusts in the United Kingdom. Interviews are audio-recorded, transcribed verbatim and analysed using interpretative phenomenological analysis. Ethical approval for this study was granted by the Office for Research Ethics Committees Northern Ireland (REC Reference: 22/NI/0107).
Results: Analysis has generated five preliminary themes: reduced appetite; reduced functionality; weight loss interpreted as a bad sign; social impact of cachexia; tension over feeding. Data reflects the multidomain impact of cachexia on patients with ESKD, impacting on biological, psychological and social domains. Furthermore, analysis confirms that the impact of cachexia in ESKD affects not only patients but also their loved ones who care for them in the domiciliary setting.
Conclusions: These preliminary insights are a critical first step in the development of care that both recognizes and responds to the needs of this population. The findings of this study will help healthcare providers understand the challenges that individuals with ESKD and their carers face in relation to cachexia and inform future clinical practice guidelines. Further research and supportive interventions which are co-designed to address the multifaceted impact of cachexia in ESKD are urgently required.
1-10
Induction of adipose lipolysis by acidosis-adapted cancer cells to meet their increased fatty acid demands
Camille Lefevre1, Olivier Feron2 and Laure B. Bindels1
1Metabolism and Nutrition Research group (MNut), Louvain Drug Research Institute (LDRI), Universitécatholique de Louvain, Brussels, Belgium;2Pole of Pharmacology and Therapeutics (FATH), Institut de Recherche Expérimentale et Clinique (IREC), Université catholique de Louvain, Brussels, Belgium
Introduction: Cancer cachexia is characterized by an involuntary weight loss which cannot be restored by nutritional support, often due to adipose tissue depletion, and limits both the survival and the anticancer response in patients. Advanced tumours which are associated to cachexia present an altered micro-environment with large hypoxic and/or acidic areas. We know from previous work that acidosis-adapted cancer cells develop a fatty acid-dependent metabolism, the latter further supporting cancer cell invasion and metastases.
As fatty acid consumption by acidosis-adapted cancer cells increases, we reasoned that fatty acids derived from adipose tissue lipolysis could sustain this fatty acid craving leading to the subcutaneous and visceral adipose tissue depletion observed in the context of cancer cachexia. We formulate the hypothesis that acidosis-adapted cancer cells foster this adipose lipolysis by releasing pro-lipolytic soluble factors.
Methods: To evaluate the pro-lipolytic capacities of acidosis-adapted cancer cells, primary mouse adipocytes from subcutaneous and visceral adipose tissues were exposed to conditioned medium from human acidosis-adapted cancer cells (pH 6.5), compared to naïve cancer cells (pH 7.4), from pharynx (Fadu), cervix (Siha), and colon (HCT). In parallel, rt-PCR and RNA sequencing were performed to identify pro-lipolytic mediators. Because of the ability of tumours to develop spontaneously an acidosis in vivo, Fadu and HCT cancer cells were injected in immunodeficient mice.
Results: Conditioned media from pH 6.5 cells triggered an increase in lipolysis of both subcutaneous and visceral primary adipocytes. Both Fadu and HCT injections in vivo support the ex vivo phenotype by promoting the subcutaneous and/or visceral adipose tissue weight loss. Known pro-lipolytic mediators were distinctly modulated with acidosis according to the cancer cell type, while RNA sequencing reveals 24 common predicted secreted proteins with a potential role in the induction of lipolysis.
Conclusions: Microenvironmental acidosis promotes the mobilization of fatty acids derived from adipocytes via the release of soluble factors by cancer cells. Some of these factors are currently being examined for their pro-lipolytic potential with the goal to identify attractive candidates for dualistic innovative treatments tackling both cancer progression and cachexia.
1-11
Role of fibroadipogenic progenitors in pancreatic cancer cachexia
Ashok Narasimhan and Chun Wai Cheung and Chihkai Chang and Fabio Rossi
School of Biomedical Engineering, University of British Columbia, Vancouver, Canada
Background: Different signalling pathways are associated with muscle atrophy in cancer cachexia. However, the role of muscle micro-environment, particularly the contribution of specific cell types to overall muscle wasting has not been comprehensively explored. The current study aims to understand the role of fibroadipogenic progenitors (FAPs) in muscle wasting using an experimental model of pancreatic cancer cachexia. FAPs provide trophic signals to muscle stem cells for efficient regeneration during injury. However, when chronic inflammation ensues, as often the case in cachexia, the muscle micro-environment is altered where FAPs may produce pathologic fibrogenic and/or adipogenic progeny, leading to fibrofatty infiltration in muscle- a hallmark of cachexia.
Aim: Investigate (i) if FAPs in muscle are dysregulated, (ii) the role of microRNAs (miRNAs, small non-coding RNAs which modulate gene expression) in FAP dysregulation and (iii) if modulating miRNAs in tumour reduces FAP dysregulation and muscle wasting.
Methods: C57BL/6J mice were orthotopically implanted with 2 million KPCY cells. Control group received sham surgery. Muscle and adipose weights were measured at different time points following surgery (weeks 2,3 and 4). FAPs were subjected to RNA sequencing and metabolomics. miRNA from tumour and FAPs were profiled using Nanostring.
Results: No significant difference was observed in muscle weights in weeks 2 and 3 between cancer and control. However, several genes implicated in cachexia such as Il1b, Inhbb, Bmp7 were altered in 2 weeks muscle indicating early molecular changes. Trim 63, Fbxo32 and Il6ra were significantly upregulated in 3 and 4 weeks. Significant difference was observed in muscle weights and gene expression at 4 weeks. RNAseq in FAPs from week 2 identified genes associated with decreased lipid synthesis and inflammation. Fibrosis associated pathways were predominantly present in weeks 3 and 4 potentially indicating a sustained negative effect on FAPs. Metabolomics analysis in FAPs identified downregulation of branched chain amino acids such as leucine, valine, and isoleucine along with other amino acids. Thirty and 194 differentially expressed miRNAs were identified in FAPs and tumour, respectively. miR-27a-3p was selected as candidate molecule for further characterization in tumour and FAPs. Downregulation of miR-27a-3p in FAPs led to increased adipogenesis and its upregulation increased proliferation in cancer cells, exhibiting a cell/tissue type specific function of miRNA. Further characterization of miR-27a-3p in tumour and FAPs is ongoing.
Conclusions: The current study opens a new avenue of research in cachexia to understand the role of FAPs dysregulation in muscle wasting through miRNAs.
1-12
Mechanisms of skeletal muscle atrophy in patients with early breast cancer treated with chemotherapy: insights from acute and chronic measurements
Joris Mallard1,2,3, Elyse Hucteau1,2,3, Laura Bender3, Fabien Moinard-Butot3, Roland Schott3, Carole Pflumio3, Philippe Trensz3, Michal Kalish-Weindling3, Antoine Grandperrin1,2, Fabrice Favret1,2, Xavier Pivot3, Thomas J. Hureau1,2 and Allan F. Pagano1,2
1Biomedicine Research Center of Strasbourg (CRBS), UR 3072, ‘Mitochondrie, Stress oxydant, Protection musculaire’, University of Strasbourg, Strasbourg, France;2Faculty of Sport Sciences, European Center for Education, Research and Innovation in Exercise Physiology (CEERIPE), University of Strasbourg, Strasbourg, France;3Institute of Cancerology Strasbourg Europe (ICANS), Strasbourg, France
Introduction: Patients with early breast cancer are mainly treated with chemotherapy, which leads to skeletal muscle atrophy. To date, a comprehensive understanding of the underlying cellular processes, through skeletal muscle biopsies, is still needed. Moreover, there is no study investigating the acute effects of a single chemotherapy administration in patients while it would provide important insights on the mechanisms involved in skeletal muscle atrophy. Therefore, this study aimed to investigate both acute and chronic cellular mechanisms triggering skeletal muscle atrophy in breast cancer patients treated with chemotherapy.
Methods: Two separate experimentations were conducted. In study 1, 13 early breast cancer patients treated with chemotherapy were included and muscle biopsies from the vastus lateralis muscle were performed pre- and post-treatment (i.e. after the whole chemotherapy treatment completion, 18 ± 1 weeks). In study 2, 10 early breast cancer patients were included and muscle biopsies were performed pre- and 4 days after the first chemotherapy administration. Histological and western blotting analyses were conducted.
Results: Four days after the first chemotherapy administration, a decrease in follistatin (−54%; P < 0.05) protein expression was found, without change in myostatin levels. MuRF1 protein expression was drastically increased acutely (+523%; P < 0.05) and remained upregulated at the end of the chemotherapy (+129%; P < 0.05), along with NFκB (+163%; P < 0.05), an important transcription factor implicated in its transcription process. Interestingly, key markers of the autophagy process were dysregulated 4 days after the first chemotherapy, as evidenced by a decrease in Atg7 (−72%; P < 0.05), LC3B-II/I ratio (−50%; P < 0.05), and no change in p62 marker expression. These results, combined with those obtained after the end of the chemotherapy treatment, demonstrate the fact that the autophagy process was downregulated in patients with breast cancer, which induces skeletal muscle atrophy. We therefore explored the cross-sectional area of the vastus lateralis muscle fibres and found a decrease in type I (−18%; P < 0.05) as well as in type II (−22%; P < 0.05) muscle fibres at the end of the chemotherapy treatment.
Conclusions: The skeletal muscle atrophy observed in breast cancer patients treated with chemotherapy is likely explained by an early upregulation of the ubiquitin-proteasome system and a decrease in the autophagy process. These alterations, highlighted as soon as 4 days after the first chemotherapy administration, emphasize the need to develop countermeasures immediately after the start of chemotherapy to prevent skeletal muscle atrophy.
1-13
Lung tumour derived factors impair myogenic capacity and mitochondrial function of muscle progenitor cells
Nikki Wanders1, Wouter van de Worp2, Chrysa Kapsali1,2, Paula Bilbao Fraile2, Hubert Smeets1 and Ramon Langen2
1Department of Toxicogenomics, MHeNS, Maastricht University, Maastricht, The Netherlands;2Department of Respiratory Medicine, NUTRIM, Maastricht University, Maastricht, The Netherlands
Introduction: Cancer cachexia is a multifactorial syndrome, which can affect up to 60% of lung cancer patients. It is characterized by loss of skeletal muscle mass and leads to lower treatment response and reduced quality of life. Previous work has shown myogenesis impairments along with mitochondrial alterations in cachectic muscle. It is unclear whether tumour or host-responses drive these myogenic impairments and mitochondrial alterations. We tested the hypothesis that factors secreted by cachexia-inducing tumours inhibit myogenic fusion and mitochondrial function of muscle cells.
Methods: 344P lung adenocarcinoma cells, which induce lung cancer cachexia and muscle mitochondrial alterations in vivo (Van de Worp, 2023), were cultured in vitro to produce tumour conditioned medium (tCM). A conditional luciferase cassette reliant on myogenic fusion-dependent Cre-mediated recombination was expressed in a myoblast-myotube (MB-MT) co-culture to quantify myogenic fusion by assessing luminescence in cell lysates. During or prior to myotube fusion, MB-MT co-cultures were left untreated or treated with tCM or control lung epithelial cell-derived conditioned medium (cCM), or medium with a mitochondrial inhibitor (CCCP). In addition to luciferase activity, cells were lysed and mitochondrial DNA (mtDNA) copy number, ATP production and citric synthase (CS) and 3-hydroxyacyl-CoA dehydrogenase (HAD) activity were assessed.
Results: When treated in the MB-MT co-culture stage, myogenic fusion was strongly reduced by tCM or CCCP exposure. A similar effect was observed when myoblasts were treated with tCM or CCCP prior to fusion. mtDNA copy number and ATP production were reduced in the co-cultures exposed to tCM during fusion as well, despite an increase in HAD and CS activity.
Conclusions: Our data demonstrate that tumour derived factors can cause mitochondrial impairments and can inhibit fusion of muscle cells. Disrupting mitochondrial function inhibits myogenic fusion as well, which could indicate a potential involvement of mitochondrial dysfunction in tumour-induced muscle wasting in cancer cachexia, although a causal role remains to be established.
Worp, W. R. P. H., Theys, J., González, A. S., Heyden, B., Verhaegen, F., Hauser, D., Caiment, F., Smeets, H. J.M., Schols, A. M.W.J., Helvoort, A., Langen, R. C.J. (2023) A novel orthotopic mouse model replicates human lung cancer cachexia, Journal of Cachexia, Sarcopenia and Muscle. https://doi.org/10.1002/jcsm.13222, 14, 1410, 1423.
1-14
Regulation of pancreatic cancer-induced muscle wasting through the obestatin/GPR39 system
Icía Santos-Zas1, Andrea Calviño-Lodeiro1,2, Tania Cid-Díaz3, Saúl Leal-López2, Silvia Costas-Abalde1,2, Carlos Seoane-Mosteiro1, Rosalía Gallego-Gómez4, Juan Enrique Domínguez-Muñoz2, Yolanda Pazos-Randulfe2 and Jesús Pérez-Camiña1
1Servicio Gallego de Salud (SERGAS), Grupo de Endocrinología Celular, Instituto de Investigación Sanitaria de Santiago (IDIS), Complejo Hospitalario Universitario de Santiago (CHUS), Santiago de Compostela, Spain;2Grupo de Investigación Traslacional en Enfermedades del Aparato Digestivo, IDIS, CHUS, SERGAS, Santiago de Compostela, Spain;3Department of Pathology and Laboratory Medicine, Weill Cornell Medicine, New York, NY, USA;4Department of Morphological Sciences, Universidad de Santiago de Compostela, Santiago de Compostela, Spain
Background: we investigated whether the obestatin/GPR39 system, an autocrine signalling system acting on myogenesis and with anabolic effects on the skeletal muscle, could protect against pancreatic cancer-driven muscle cachexia and associated morbidity and mortality.
Methods: In this study, we used an in vivo model of muscle cachexia induced by orthotopic tumour implantation of pancreatic ductal adenocarcinoma (PDAC). We examined the molecules that define the interplay between the tumour and the skeletal muscle through the obestatin/GPR39 system. The findings were extended to in vitro effects on human myotubes co-cultured with PDAC cells (PANC-1 cells).
Results: A pilot study developed by using a co-culture system of human myotubes and PANC-1 cells showed that obestatin signalling decreased the expression of the E3 ubiquitin-ligase atrogenes (MuRF1/MAFbx). The protection against myotube atrophy was associated to the activation of anabolic signalling hallmarks (AKT/mTORC1/S6/4E-BP1) and autophagy flux, whereas NF-KB and iNOS signalling, hallmarks of muscle wasting, were attenuated. Of note, obestatin increased the expression of both slow- and fast-MHC that positively correlated with restoration of myotube phenotype. Simultaneously, obestatin treatment inhibited proliferation in PANC-1 cells. These actions acquire more significance considering the attenuation of preproghrelin expression, and thus obestatin, in human myotubes in the presence of PANC-1 cells. In vivo, we established an orthotopic PDAC model to examine the therapeutic efficacy of obestatin. Notably, obestatin treatment mitigated cancer-associated cachexia manifestations, reducing tumour associated skeletal muscle weight loss. In this model, obestatin suppressed the catabolic signalling hallmarks in tibialis anterior muscle, including AMPK, to regulate muscle catabolism via the downregulation of the E3-ubiquitin ligases and activation of autophagy flux.
Conclusions: These results highlight the potential of the obestatin/GPR39 system to fine-tune the effects of PDAC on skeletal muscle wasting.
1-15
Tumour organoid-derived factors from cachectic pancreatic cancer patients induce a pro-inflammatory macrophage phenotype: role of macrophage migration inhibitory factor
Valerie D'Antonio and Min Deng and Rianne Vaes and Alisa Huber and Mo Hadfoune and Steven Olde Damink and Sander Rensen
Department of Surgery and NUTRIM School of Nutrition and Translational Research in Metabolism, Maastricht University, Maastricht, The Netherlands
Introduction: Systemic inflammation induced by tumour-derived factors is considered to play a key role in the pathogenesis of cancer cachexia. Macrophages mediate pro-inflammatory immune responses in several metabolic disorders. We hypothesized that factors released by tumour cells from cachectic patients induce a pro-inflammatory macrophage phenotype, and focused on Macrophage Migration Inhibitory Factor (MIF), whose increased expression in several cancer types correlates with poor patient outcomes.
Methods: Human monocyte-derived macrophages were exposed to conditioned medium (CM) collected from pancreatic tumour organoids from cachectic (n = 4) or non-cachectic (n = 3) patients, or maintained in control medium. After 24 h, zymosan-particle phagocytosis assays were performed by live cell imaging, and cytokine expression and secretion were determined by qPCR and ELISA. Mitochondrial respiration was assessed using a Seahorse analyser. Macrophage morphology was assessed using Cellpose software to obtain shape descriptions and area measurements. Several assays were performed in the presence of ISO-1, a clinically approved MIF inhibitor. MIF concentrations in CM and plasma of 107 pancreatic cancer patients were determined by ELISA.
Results: Macrophage phagocytosis rates were increased after exposure to tumour organoid CM from cachectic versus non-cachectic individuals (3.1 ± 0.2 vs. 2.4 ± 0.3, P < 0.05). IL-6 and MIF secretion were increased after exposure to CM from cachectic versus non-cachectic individuals (IL-6: 2.75 ± 2.9 vs. 1.69 ± 4.1 ng/mL, P < 0.05; MIF: 2.84 ± 0.49 vs. 1.87 ± 0.48 ng/mL, P < 0.05). Expression of IL-1alpha, Mcp-1, and TNF-beta followed a similar pattern, but IL-10 was not affected. Average macrophage area was higher after exposure to ‘cachectic’ CM versus control (600 ± 12 vs. 450 ± 31 μm2, P < 0.01) and roundness was reduced (0.65 ± 0.02 vs. 0.72 ± 0.03, P < 0.001). Oxygen consumption rates were lower after exposure to CM from cachectic versus non-cachectic patients (81.7 ± 29.0 vs. 100.8 ± 21.4 pmol/min, P < 0.001). Plasma MIF concentrations were higher in cachectic (n = 73) versus non-cachectic (n = 34) patients (3.05 ± 0.38 vs. 1.72 ± 0.23 ng/mL, P < 0.05) and in ‘cachectic’ versus ‘non-cachectic’ CM (1.48 ± 0.24 vs. 0.30 ± 0.02 ng/mL, P < 0.01). However, MIF inhibition during CM exposure did not affect macrophage phagocytosis or cytokine production.
Conclusions: Factors other than MIF released by tumour cells from cachectic patients induce a pro-inflammatory macrophage phenotype.
1-16
Leucine supplementation alters inflammatory gene expression in male, but not female ApcMin/+ cancer cachectic mice
Eleanor R. Schrems and Francielly Morena Da Silva and Ana Regina Cabrera and Kevin A. Murach and Nicholas P. Greene and Tyrone A. Washington
Department of Health Human Performance and Recreation, University of Arkansas, Fayetteville, AR, USA
Introduction: Cancer cachexia (CC) is a multifactorial wasting syndrome characterized by a significant loss in lean and/or fat mass, and is a leading cause of mortality in cancer patients. CC is often associated with enhanced proteolysis, mediated by pro-inflammatory cytokines. It is established that proinflammatory cytokines (IL-6 and IL-1β) are increased in several models of CC, promoting downstream catabolic functions. Nutraceutical treatments, such as the branched-chain amino acid, leucine, have been proposed as a potential treatment strategy to protect cancer patients against cachexia by targeting inflammation and muscle protein synthesis. However, contradictory findings warrant further investigation.
Purpose: Examine the effects of leucine supplementation on the skeletal muscle inflammatory response across biological sexes during CC.
Methods: Male and female ApcMin/+and their wild type (WT) littermates were used in this study. At ~5 weeks old, mice were given tap water (NL) or 1.5% leucine-supplemented water (L), with ad libitum food and water access (n = 4–10/group/sex). The experimental endpoint for all groups was ~20 weeks of age. Skeletal muscles, fat, and organs were excised and weighed. Il6, Il1b, Tnfa, and Nfkb mRNA abundance in the tibialis anterior muscle was assessed via qPCR. Two-way ANOVAs (leucine supplementation × genotype) were conducted within biological sexes to determine significant main effects and interactions.
Results: The ApcMin/+group had lower body mass, muscle mass, fat mass, and higher spleen mass in both sexes (P < 0.05) compared to WT, confirming a cachectic phenotype independent of leucine supplementation. In males, Il6 was higher in ApcMin/+compared with WT independent of leucine supplementation (P < 0.05). There was an interaction of genotype and treatment on Il1b, where Il1b was higher in APCNL compared with WTNL, but lower in APCL compared with APCNL (P < 0.05). Tnfa was lower in WTL and APCL groups, independent of genotype (P < 0.054). Nfkb was not different between groups. In females, Il6, IL1b, Tfna, and Nfkb were all higher in ApcMin/+ compared with WT groups independent of leucine supplementation (P < 0.05).
Conclusions: Results of this study demonstrate males appear to have a leucine dependent response on inflammatory gene expression in skeletal muscle, whereas females do not. Based on these differences in leucine supplementation between sexes indicates the existence of a sexual dichotomy. Our results demonstrate there may be a sex dependent response to leucine supplementation in cancer cachexia.
1-17
Using adipose tissue organoids: a new avenue for cancer cachexia research in vitro
Abdolreza Nazari and Jochen Springer
Berlin Institute of Health Center for Regenerative Therapies (BCRT), Charité Universitätsmedizin Berlin, Berlin, Germany
One of the primary pathophysiologies of cancer cachexia is systemic inflammation, which leads to weight loss through the breakdown of skeletal muscle and adipose tissue (AT) and the suppression of hunger. Significant crosstalk between AT and muscle loss suggests a strong interplay between the two. There is a dire medical need for effective treatments for the large number of patients suffering from cancer cachexia, as treatment options are extremely limited. Therefore, it is imperative to develop novel therapies. Traditional two-dimensional cell culture methods are inadequate for studying cancer cachexia due to the lack of interaction between different cell types. Animal models, typically rodents, are currently used for meaningful cachexia research. However, a significant gap exists in translating findings from animal models to clinical studies. In this project, we aim to address this gap by developing and validating 3D organoids of adipose tissue in the laboratory. These organoids will provide a better understanding of the molecular mechanisms involved in AT alterations at different stages of cancer cachexia.
2-01
Neutrophil-derived S100a8/a9 as a mediator of adverse cardiac remodelling in cancer-associated cachexia
Parham Diba1,2, Abigail C. Buenafe2, Mason A. Norgard2, Peter R. Levasseur2, Tetiana Korzun1,2, Xinxia Zhu2, Ariana Sattler3, Xiaolin Li2, Brennan Olson1,2 and Daniel L. Marks2,3
1Medical Scientist Training Program, Oregon Health and Science University, Portland, OR, USA;2Pape Family Paediatric Research Institute, Oregon Health and Science University, Portland, OR, USA;3Brenden-Colson Center for Pancreatic Care, Oregon Health and Science University, Portland, OR, USA
Introduction: Compromised cardiac function resulting from structural and functional remodelling is commonly observed in cancer patients and survivors, leading to a difficult treatment management course, reduced quality of life, and eventual death of approximately 15–20% of patients. While some cancer patients experience cardiac dysfunction as a result of chemotherapeutic agents, numerous studies in chemotherapy-naïve cancer patients revealed signs of cardiac insufficiency, implicating cachexia as a contributing factor. Cachexia, a wasting syndrome, is commonly observed in cancer patients, leading to cardinal symptoms including anorexia, fatigue, and elevated basal metabolic rate. However, the mechanistic relationship between cachexia and adverse cardiac remodelling is unknown.
Methods: To investigate this question, we used a murine model of pancreatic ductal adenocarcinoma (PDAC) associated cachexia. To generate the model, a pancreatic tumour cell line was orthotopically implanted in the pancreas of WT mice. The cells are derived from tumours in C57BL/6 mice expressing a constitutively active mutant oncogene KRASG12D and a point mutation in the tumour suppressor gene P53R1172H with expression induced and targeted to the pancreas via Cre recombinase expression under the Pdx-1 promoter. Mediators of cardiac remodelling were assessed at the cellular and molecular level using bulk-RNA sequencing, flow cytometry, and ELISA studies.
Results: Tumour bearing animals demonstrated a gene signature consistent with structural and functional remodelling of the heart and significant elevation in biomarkers of cardiac damage in plasma, including Troponin-I, Galectin-3, and creatine kinase-MB. RNA-sequencing analysis of the heart identified granulocyte-derived S100a8/a9 as a candidate driver of adverse cardiac remodelling. We validated the increase in cardiac S100a8/a9 both at RNA and protein level in various PDAC cells lines, and flow cytometry experiments revealed recruitment of neutrophils to the heart.
Conclusions: Our data identified neutrophils and S100a8/a9 as candidate drivers of adverse cardiac remodelling in cancer-cachexia. Neutrophil activation and NETosis in the heart can lead to release of S100a8/a9 heterodimer, activating inflammatory pathways in the heart and deteriorating cardiac structure and function. Therefore, our observations provide support for neutrophils and S100a8/a9 as potential therapeutic targets of adverse cardiac remodelling in cancer-cachexia patients.
2-02
Mechanistic insights from an integrative analysis of biological sex differences in two colorectal cancer cachexia models
Ana Regina Cabrera1, J. William Deaver1, Francielly Morena da Silva1, Eleanor Schrems2, Tyrone A. Washington2 and Kevin A. Murach and Nicholas P. Greene1
1Cachexia Research Laboratory, Exercise Science Research Center, Department of Health, Human Performance and Recreation, University of Arkansas, Fayetteville, AR, USA;2Exercise Muscle Biology Laboratory, Exercise Science Research Center, Department of Health, Human Performance and Recreation, University of Arkansas, Fayetteville AR; Molecular Muscle Mass Regulation Laboratory, Exercise Science Research Center, Department of Health, Human Performance and Recreation, University of Arkansas, Fayetteville, AR, USA
Introduction: Cancer-Cachexia (CC) is clinically characterized by an involuntary weight loss of >5% within 6 months. This study aimed to investigate the transcriptomic changes in skeletal muscle (SKM) during CC progression in male and female mice.
Methods: TA samples were collected from two colorectal-CC animal models: eight-week-old BALB/c mice injected with C26-cell allografts or PBS as control (samples collected after 10-, 20-, or 25-days of cancer injection), and 20-week-old ApcMin/+mice and their WT-littermates (n = 6–8/sex/group/model). Global gene expression analysis was performed, and differentially expressed genes were identified (FDR < 0.05).
Results:ApcMin/+ groups, both female and male mice, developed severe cachexia after 20-weeks, while C26-male mice experienced moderate body weight loss after 20-days and SKM mass loss after 25-days. In contrast, C26-females-25-days exhibited a mild cachectic phenotype, with preserved body weight and SKM despite exhibiting other hallmarks of CC such as hepatosplenomegaly. At the transcriptomic level, all groups had Fbxo32 and Trim63 upregulated (>+2.16-fold, except C26-male-20-days), suggesting protein degradation as a common factor between sexes and models. Additionally, Map 1lc3b, Bnip3, P62, and ULK-1 and Beclin-1 complexes related genes were upregulated for C26-male-25-days and males and females ApcMin/+ (>+1.5-fold), suggesting proteolysis and phagophore formation for mitophagy and autophagy. Moreover, in the same groups, genes related to ETC-complex subunits, pyruvate dehydrogenase (PDH) complex, TCA cycle and feeder pathway enzymes were downregulated (>−2.63-fold), potentially affecting mitochondrial energy production and pathways related to amino acid synthesis and their availability. Male and female ApcMin/+ showed dysregulation of carnitine-palmitoyltransferase (CPT) and mitochondrial pyruvate carrier (MPC) genes (>−2.3-fold), suggesting deficiency in the transport of lipid and pyruvate for mitochondrial oxidation. Furthermore, upregulation in genes coding for malonyl-CoA decarboxylase (MCD) and AS160 (>+1.5-fold) was observed after 25-days in both C26 sexes, and in ApcMin/+-males, suggesting an increase in fatty acid and carbohydrate oxidation. In contrast, C26-females did not exhibit dysregulation in the mRNA content of ETC subunits and TCA and feeder pathway enzymes.
Conclusions: This study highlights significant metabolic disruptions in SKM during CC with differences observed between sexes. Preservation of mitochondria function may play a crucial role in maintaining SKM, particularly during early time points in female mice, despite an upregulation in mRNA for common markers of muscle wasting. These findings help define underlying mechanisms of muscle wasting during CC and provide valuable insights into potential interventions to preserve SKM in both male and female populations.
Acknowledgements: Funded by the National Institute of Health (NIH) and the Arkansas Biosciences Institute (ABI). Awards: 5 R01 AR075794-02, P20GM125503, AWD-101273, NIC R00 AG063944.
2-03
The dialogue between metastatic cells and the host
Blanca Majem1, Josefina Martin1, Claudia Bigas1, Gloria Pascual1 and Salvador Aznar Benitah1,2
1Institute for Research in Biomedicine (IRB Barcelona), The Barcelona Institute of Science and Technology (BIST), Barcelona, Spain;2ICREA, Catalan Institution for Research and Advanced Studies, Barcelona, Spain
Introduction: Malnutrition and cachexia are major problems of metastatic cancers and lead to depletion of the main energy depots. Importantly, the metabolic plasticity of metastatic cells allows them to adapt under certain nutrient-limiting conditions and to reach different organs; however, how metastatic cells metabolically outcompete with the host physiology to boost their energetic demands, is poorly understood. Our efforts are focused on understanding how metastatic tumours communicate with distant tissues rarely inhabited by metastatic cells, to unveil potentially targetable mechanisms underpinning cachexia, with the overarching goal of blocking metastasis, and improve quality of life of metastatic patients suffering from cachexia.
Methods: Tackling metastasis in the context of wasting requires understanding of (i) how metastatic tumours communicate with the body through secreted factors, (ii) how metastasis contributes to chronic inflammation, (iii) which metabolic changes underneath of these inflammatory-secretory axes are key during tissue wasting in metastatic patients. We systematically tested this hypothesis by using an oral cancer syngeneic mouse model, and evaluate how tumour/metastasis growth correlates with cachexia parameters, including body weight loss, reduction in food intake and peripheral tissue loss. We performed high-throughput metabolomic and transcriptomic analyses in several tissues, tumours and plasma to comprehensively determine a wasting signature.
Results: We identified systemic metabolic alterations in metastatic bearing hosts in the MOC2 syngeneic mouse model. In particular, we defined by multiple omics a 2-stage cachexia process associated with changes in histological parameters of the liver, muscle and fats. This 2-stage cachexia progression leverages the host metabolism in a different way, associated to a more aggressive metastatic behaviour when tumour cells were previously exposed to palm-rich diet. We also found potential factors that can be secreted by the metastatic cells in the lung metastasis compartment, and found important candidates that could be inhibited, which are related to increased lipid metabolism and cachexia.
Conclusions: We conclude that enhanced metastatic potential is associated with increased body weight loss and identified two stages of cachexia (early and late-cachexia), with no significant changes in food intake when body weight loss is initiated. Progressive peripheral tissue loss was found in the two stages suggesting either gradual or distinct metabolic changes in both stages of cachexia. Metabolic and transcriptomic analyses of these two stages are key to understand how metastasis influence the host metabolism. Finally, inhibition of secreted pro-cachectic factors by metastatic cells will validate the metastasis-to-the-host axes and prove its anti-metastatic and anti-cachectic therapeutic potential.
2-04
Microbiota-derived secondary bile acids to tackle cancer cachexia
Morgane M. Thibaut1, Justine Gillard1,2, Martin Roumain3, Adeline Dolly1, Nathalie M. Delzenne1, Giulio G. Muccioli3 and Laure B. Bindels1
1Metabolism and Nutrition Research Group, Louvain Drug Research Institute, Université catholique de Louvain (UCLouvain), Brussels, Belgium;2Laboratory of Hepato-Gastroenterology, Institut de Recherche Expérimentale et Clinique, Université catholique de Louvain (UCLouvain), Brussels, Belgium;3Bioanalysis and Pharmacology of Bioactive Lipids Research Group, Louvain Drug Research Institute, Université catholique de Louvain (UCLouvain), Brussels, Belgium
Introduction: Bile acids can act as powerful signalling molecules and exert diverse actions on host metabolism and immunity. The two main steps involved in the bacterial metabolism of bile acids are the hydrolysis of conjugated bile acids into free bile acids, catalysed by bile salt hydrolases (BSH), and the 7α-dehydroxylation (7αDH) to generate secondary bile acids. We previously reported alterations in the gut microbiota composition and in bile acid pathways in cancer cachexia. We also showed that the modulation of the bile acid profile could affect cachectic features. Here, we investigated the gut microbiota-bile acid crosstalk in cancer cachexia.
Methods: We compared mice inoculated with cachexia-inducing C26 colon carcinoma cells (C26 mice), non-cachexia-inducing C26 colon carcinoma cells (NC mice), and sham-injected mice (CT mice). We performed hepatic and portal bile acid quantification using HPLC-MS and analysis of the gut microbiota composition using 16S rRNA gene sequencing of CT, C26 and NC mice. We also measured the BSH activity in CT and C26 mice and we estimated the 7αDH activity.
Results: Hepatic bile acid profiling revealed increased levels in conjugated primary bile acids and a four-fold decrease in total secondary bile acids in C26 cachectic mice as compared to CT mice, whereas they were not changed in NC mice compared to CT. We also revealed that the gut dysbiosis found in the C26 cachectic mice, marked by an increase in the Enterobacteriaceae family and decreased levels in the Ruminococcaceae and Lachnospiraceae families, was not observed in NC mice, displaying similar profile to CT mice. No significant difference in microbial BSH activity was found in faecal extracts from C26 mice as compared to CT. Interestingly, the Lachnospiraceae family that has been shown to be able to perform the 7αDH activity, was found to be positively correlated with portal secondary bile acids in C26 mice. In accordance with our hypothesis, the predicted 7αDH activity (based on the secondary/primary bile acid ratio) decreased in the faeces of C26 mice as compared to CT mice.
Conclusions: The alterations in bile acid profile and gut microbiota are intrinsically linked with cachexia itself, and cannot only be ascribed to the presence of the tumour in C26 mice. Moreover, our data suggest a major role for the gut microbiota in bile acid alterations. Altogether, this work highlights microbiota-derived secondary bile acids as promising candidates to improve cancer cachexia.
2-05
Cancer induces cachexia by reprogramming the nuclear SUMOylation landscape in striated muscle cells
Luis V. Gand1, Bushra Khan1, Natalie Weber2, Dongchao Lu2, Christian Bär2, Andreas Pich3, Theresia Kraft1, Mamta Amrute-Nayak1 and Arnab Nayak1
1Institute for Molecular and Cell PhysiologyHannover Medical School, Hannover, Germany;2Institute of Molecular and Translational Therapeutic StrategiesHannover Medical School, Hannover, Germany;3Institute of Toxicology, Hannover Medical School, Hannover, Germany
Introduction: Cachexia is a complex, debilitating muscle-wasting disorder prevalent in 80% of cancer patients, with mortality in 30% of patients. The molecular mechanisms underlying cancer-induced cachexia (CIC) remain largely unclear. Cells use the SUMO (Small Ubiquitin-like Modifier) machinery to respond rapidly to external challenges, particularly during the stress response. As cancer triggers oxidative stress, we hypothesize that the link between SUMO and CIC might prevail. In this study, we investigated this possibility.
Methods: To induce cachexia (CIC), we treated striated muscle cells (mature mouse myotubes and neonatal rat cardiomyocytes) with IFNγ and TNFα. To study the effect of CIC on muscle physiology, we checked calcium transient, muscle cell contraction, and sarcomere organization. By RNAseq, we determined global changes of in gene expression programme in muscle cell. We performed quantitative endogenous SUMO proteomics, chromatin immunoprecipitations, epigenetic profiling of muscle-specific genes, confocal microscopy, and gene expression approaches to establish detailed molecular mechanisms in CIC.
Results: Here, we demonstrated that CIC affects muscle cell physiology at different levels. CIC-altered specific gene expression programme that ultimately led to sarcomere disorganization, impaired calcium transient process, and severely disrupted muscle cell contraction. Mechanistically, CIC triggered an enhanced level of nuclear-soluble and chromatin-associated SUMO2/3-conjugated proteins. The mass spectrometry analysis revealed a reprogrammed network of increased SUMO-modified nuclear proteins, particularly the non-canonical polycomb repressor protein L3MBTL2 in CIC. Surprisingly, L3MBTL2 positively regulated genes involved in calcium transient and sarcomere organization. In line with this observation, depletion of L3MBTL2 phenocopied CIC. Preliminary observations showed enhanced SUMO modification of L3MBTL2 was associated with compromised active chromatin state of L3MBTL2 target genes particularly Myosin heavy chain (Myh1) and Atp2a1.
Conclusions: These outcomes revealed an unprecedented connection between SUMO and CIC. The paradoxical SUMO-associated transcriptional role of L3MBTL2 in regulating muscle-specific gene expression was targeted in CIC. Transcriptional activator role of L3MBTL2 is critical for muscle cell function. CIC-triggered higher SUMOylation of L3MBTL2 dampened transcriptional activator function leading to sarcomere organization, calcium transient process and thereby muscle function. This serves as one of the underlying mechanisms of CIC. Restoring balanced SUMOylation levels- particularly of L3MBTL2- in our ongoing experiments in the cancer cachexia models is expected to unravel possible strategies to ameliorate CIC.
2-06
Skeletal muscle microRNAs profile in patients with gastrointestinal cancer
Federica Tambaro1, Giovanni Imbimbo1, Giulia Lauteri2, Antonietta Gigante1, Maria Ida Amabile3, Giuseppe Nigri2, Cesarina Ramaccini1, Alessio Molfino1 and Maurizio Muscaritoli1
1Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2Department of Medical and Surgical Sciences and Translational Medicine, Sapienza University of Rome, Rome, Italy;3Department of Surgical Sciences, Sapienza University of Rome, Rome, Italy
Introduction: The imbalance between catabolic and anabolic processes is the defining reason for skeletal muscle (SM) atrophy, a key feature of cancer cachexia (CC). microRNAs (miRs) were shown to mediate several signalling pathways associated to muscle wasting. However, their biological roles in CC are still poorly explored. This study aimed at evaluating the expression of muscle-derived miR486-5p and miR15b-5p, which both have been found to have a regulatory effect on inflammatory pathways as well as on modulation of protein synthesis and SM homeostasis, making them attractive as early non-invasive diagnostic tools and potential novel therapeutic targets in CC therapy.
Methods: SM biopsies were obtained from 25 newly diagnosed gastrointestinal (GI) cancer patients (CP) and 10 healthy controls (C), undergoing abdominal surgery for cancer resection or for a non-malignant condition, respectively. Total RNA was extracted from SM specimens and expression levels of miR486-5p and miR15b-5p were analysed through RT-qPCR.
Results: BMI (kg/m2) did not differ in GI CP and C (24.57 ± 4.11 vs. 24.41 ± 4.00). In GI CP, the expression of miR486-5p was lower, whereas miR15b-5p was overexpressed with respect to C (0.90 ± 0.49 vs. 1.90 ± 1.98, P = 0.038 and 1.5 ± 0.49 vs. 0.53 ± 0.49, P = 0.041, respectively). Both miR486-5p and miR15b-5p expression levels were higher in weight-losing (n = 11) than in non-weight losing (n = 13) CP (1.10 ± 0.63 vs. 0.69 ± 0.25, P = 0.042 and 1.84 ± 2.14 vs. 0.60 ± 0.43, P = 0.053, respectively).
Conclusions: These preliminary data suggest that miR486-5p and miR15b-5p are differentially modulated in the SM of GI CP. Moreover, unintentional weight loss, a main feature of CC, is also associated with changes in the expression patterns of these miRs. Further investigations are mandatory in order to better clarify their role in CC-related SM wasting.
2-07
First-in-patient (phase 1b) study of the GDF-15 inhibitor ponsegromab in patients with cancer and cachexia: safety, tolerability, and exploratory measures of efficacy
Jeffrey Crawford1, Roberto A. Calle2, Susie M. Collins3, Yan Weng4, Shannon L. Lubaczewski5, Clare Buckeridge2, Ellen Q. Wang6, Magdalena A. Harrington7, Anil Tarachandani8, Michelle I. Rossulek2 and James H. Revkin2
1Duke Cancer Institute, Duke University Medical Center, Durham, NC, USA;2Internal Medicine Research Unit, Pfizer Inc, Cambridge, MA, USA;3Global Biometrics and Data Management, Pfizer R&D UK Ltd, Sandwich, Kent, UK;4Clinical Pharmacology, Pfizer Inc, Cambridge, MA, USA;5Early Clinical Development, Pfizer Inc, Collegeville, PA, USA;6Clinical Pharmacology, Pfizer Inc, New York, NY, USA;7Global Access and Value, Pfizer Inc, Cambridge, MA, USA;8Early Clinical Development, Pfizer Inc, Cambridge, MA, USA
Introduction: Cachexia is common in patients with advanced cancer and has been associated with elevated serum growth/differentiation factor 15 (GDF-15) concentrations. This first-in-patient (phase 1b) study assessed the use of ponsegromab, a monoclonal antibody against GDF-15, in participants with advanced cancer and cachexia.
Methods: Adult participants (n = 10) with cachexia, advanced cancer (non-small cell lung, colorectal, or pancreatic), and elevated serum concentrations of GDF-15 received open-label subcutaneous ponsegromab every 3 weeks (Q3W) for 12 weeks in addition to standard of care anti-cancer treatment. Study endpoints included assessment of ponsegromab safety, tolerability, and pharmacokinetics. Serum GDF-15 concentrations and exploratory measures of efficacy were also assessed.
Results: No treatment-related adverse events or injection site reactions were reported. No adverse trends in clinical laboratory tests, vital signs, or electrocardiogram parameters attributable to ponsegromab dosing were evident. Ninety-two adverse events deemed unrelated to treatment were reported; most were mild (Grade 1 = 58.7%) or moderate (Grade 2 = 28.3%) in severity. All participants were negative for anti-drug antibodies at baseline (n = 10) and after receiving 5 doses (Q3W) of ponsegromab (n = 9).
Mean unbound ponsegromab Ctrough ranged from 4041 to 4383 ng/mL between days 22 and 106. An elevated GDF-15 concentration was required for inclusion in the study. Following initiation of study treatment, median unbound GDF-15 concentration was reduced to below the lower limit of quantification (0.0424 ng/mL) on day 1 and remained suppressed until week 15 (3 weeks after final dose).
Increases in body weight were observed at all time points during the treatment (weeks 3, 6, 9, and 12) and follow-up (weeks 15, 18, and 24) periods. The mean (SD) body weight at baseline was 70.49 (16.97) kg. An LS mean (SE) increase of 4.63 kg (1.98) was observed at week 12 (end of treatment); representing an increase of approximately 6.5% relative to baseline. Improvements in actigraphy-based assessments of physical activity and in quality of life, including appetite, as assessed by Functional Assessment of Anorexia-Cachexia Therapy (FAACT) total and subscale scores, were also observed during the course of ponsegromab treatment.
Conclusions: In participants with advanced cancer, cachexia, and elevated baseline GDF-15, ponsegromab was well tolerated and suppressed serum GDF-15 concentrations to below the median concentration seen in healthy populations. Preliminary evidence of efficacy, including a mean observed weight gain of approximately 6.5% at 12 weeks, supports continued development of ponsegromab for the treatment of cancer cachexia.
Two phase 3 studies to evaluate the ghrelin receptor agonist anamorelin for malignancy-associated weight loss and anorexia in adults with non-small cell lung cancer (NSCLC): updates to the ongoing SCALA programme
Richard J.E. Skipworth1, Barry J.A. Laird2,3, Eric J. Roeland4, Tora S. Solheim5,6, Jann Arends7, Jose M. García8, Mariana S. Sousa9 and David C. Currow10
1Clinical Surgery, University of Edinburgh, Edinburgh, UK;2Institute of Genetics and Cancer, University of Edinburgh, Edinburgh, UK;3St Columba's Hospice, Edinburgh, UK;4Oregon Health & Science University, Knight Cancer Institute, Portland, OR, USA;5Department of Oncology, St. Olavs University Hospital, Trondheim, Norway;6Department of Cancer Research and Molecular Medicine, Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway;7Department of Internal Medicine, Medical Center-University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany;8Department of Medicine, Division of Gerontology and Geriatric Medicine, University of Washington School of Medicine, Geriatric Research, Education and Clinical Center, VA Puget Sound Health Care System, Seattle, WA, USA;9IMPACCT, Faculty of Health, University of Technology Sydney, Sydney, Australia;10Faculty of Science, Medicine and Health, University of Wollongong, Wollongong, Australia
Introduction: Cachexia is a devastating multifactorial syndrome characterized by weight loss and anorexia affecting most patients with advanced cancer. With no standard of care or newly FDA- or EMA-approved drugs, therapy remains an unmet clinical need. Central to this challenge are the lack of agreement on acceptable clinical trial efficacy primary endpoints and the need to revisit predetermined trial endpoints due to ongoing developments within the field.1 Formerly, regulatory agencies requested drug studies to demonstrate a meaningful change associated with morbidity/mortality, disease biology, and physical function. Consequently, lean body mass (LBM) and physical function measures have been required as suitable co-primary endpoints. However, the relevance of any association between them and of changes in physical function parameters remains theoretical,2 and phase 3 trials with new agents have not surprisingly failed to meet the functional endpoint.
Anamorelin is an oral selective ghrelin receptor agonist recently approved in Japan for cancer cachexia treatment in NSCLC, gastric, pancreatic, or colorectal cancer. In the phase 3 ROMANA trials, anamorelin demonstrated significant increase in LBM versus placebo without significant effect on handgrip strength (co-primary endpoints). Subsequently, conforming to the anabolic and appetite-stimulating properties of anamorelin, the newer phase 3 SCALA programme aimed to evaluate anamorelin superiority versus placebo in weight gain and anorexia. Herein, we report the updated efficacy endpoints of the ongoing SCALA programme.
Methods: The SCALA programme comprises two international, double-blind, phase 3 studies (NCT03743051/NCT03743064) with identical designs that enrolled adults with advanced NSCLC, weight loss (body mass index <20 kg/m2, >2% weight loss within prior 6 months), and anorexia (≤17 points on the 5-item anorexia symptoms subscale [5-IASS] and ≤37 points on the 12-item Functional Assessment of Anorexia/Cachexia Therapy anorexia/cachexia subscale [12-FAACT A/CS]). In total, 632 patients received 100 mg anamorelin or placebo (1:1) daily for up to 24 weeks. Updated co-primary efficacy endpoints are mean change in weight and 5-IASS from baseline over 12 weeks. Updated secondary efficacy endpoints (measured from baseline over 12 weeks) include: duration of treatment benefit (≥ a predefined threshold of clinical meaningfulness) in weight (≥5%) and anorexia symptoms (≥2 points in 5-IASS) (previous co-primary endpoints); duration of treatment benefit (≥0) in weight and 5-IASS, and mean change in 12-FAACT A/CS and fatigue (FACIT-F) (new endpoints added); FAACT total score (endpoint maintained). Exploratory efficacy endpoints are mostly maintained, and include mean change from baseline in weight, 5-IASS, and FAACT analysed every 3 weeks, among others. Recruitment is completed.
[1] Laird, BJA, Balstad, TR, Solheim, TS. Endpoints in clinical trials in cancer cachexia: where to start?Curr Opin Support Palliat Care.2018; 12: 445–52.
[2] McDonald, JJ, Fallon, MT, Laird, BJA. Meaningful measures in cancer cachexia: implications for practice and research. Curr Opin Support Palliat Care.2019; 13: 323–7.
Disclosures: The SCALA studies (NCT03743051 and NCT03743064) are sponsored and funded by Helsinn Healthcare SA. Helsinn participated in the writing, review, and approval of this abstract.
Richard J.E. Skipworth: R.J.E.S. is funded by an NHS Research Scotland clinician post. He is a previous member of advisory boards for Helsinn; has received grant funding from Novartis; and has served as a consultant for Helsinn, Avidity Biosciences, Faraday Pharmaceuticals, and Actimed Therapeutics; Barry J.A. Laird: Dr Laird has done consultancy for Artelo, Faraday, Toray and Actimed; Eric J. Roeland: E.R. has served as a consultant for Mitobridge Inc., Asahi Kasei Pharmaceuticals, DRG Consulting, Napo Pharmaceuticals, American Imaging Management, Immuneering Corporation, and Prime Oncology. Additionally, he has served on recent advisory boards for Heron Pharmaceuticals, Vector Oncology, and Helsinn Pharmaceuticals. He has also served as a member of data safety monitoring boards for Oragenics, Inc, Galera Pharmaceuticals, and Enzychem Lifesciences Pharmaceutical Company; Tora S. Solheim: nothing to disclose; Jann Arends: J.A. has served on advisory boards for Baxter and Danone and has received honoraria for scientific presentations from Baxter, B. Braun, Fresenius Kabi, Nestlé, and Danone; Jose M. García: J.M.G has received research support from Aeterna Zentaris Inc., Helsinn Therapeutics, Inc. and Extend Biosciences and is a consultant with Faraday Pharmaceuticals, Toray Pharmaceuticals and Dexcel Pharmaceuticals; Mariana S. Sousa: nothing to disclose; David C. Currow: D.C.C. is an unpaid advisory board member for Helsinn Healthcare SA. He is a paid consultant and receives payment for intellectual property with Mayne Pharma, and is a consultant with Specialized Therapeutics Australia Pty. Ltd.;
Acknowledgments: The authors would like to acknowledge and thank the patients, investigators, and the study teams at the participating centers. Editorial and medical writing support was provided by Iratxe Abarrategui, PhD, CMPP, from Aptitude Health, The Hague, the Netherlands and funded by Helsinn Healthcare SA.
2-09
Scalable and privacy-preserving AI can characterize and discover more cachectic cancer patients compared to ICD codes and NLP based approaches
Richard Skipworth1,2, Judith Sayers1,2, Barry J.A. Laird1,2, Yike Guo3,4,5, Jingqing Zhang3,5, Marcin Burda5, Parastoo Falakaflaki5, Atri Vivek Sharma5 and Vibhor Gupta5
1University of Edinburgh, Edinburgh, UK;2NHS Lothian, Edinburgh, UK;3Data Science Institute, Imperial College London, London, UK;4The Hong Kong University of Science and Technology, Hong Kong SAR, China;5Pangaea Data Limited, London, UK
Introduction: International Classification of Diseases (ICD) codes cannot be used to accurately discover cachectic cancer patients, due to significant miscoding. We present application of novel AI driven product (PIES) that improves on the limitations of ICD or pre-emptive keyword based methods by automatically characterizing undiagnosed, misdiagnosed, and miscoded cachectic patients based on the discovery of clinical signatures (which otherwise clinicians have to ascertain through manual review) from electronic patient records (EPRs) in a scalable and privacy-preserving manner.
Methods: PIES uses AI to determine the clinical signature, i.e the key clinical features and their relationships, which characterize cancer patients with cachexia based on both structured and textual data within EPRs. Three hundred eighty patient records were manually assessed by three clinicians, of which, 145 were used to configure PIES to discover the clinical signature for cachectic cancer patients and the remaining 235 were used as the test set to evaluate its performance.
Results: On the test set, ICD codes correctly discovered only 39 patients with cancer cachexia. In comparison, PIES correctly discovered 146 cachectic cancer patients (90.7% sensitivity) - meaning PIES found 274% more clinically validated cachectic cancer patients compared to ICD codes. These results corroborate those of our previous study, where PIES was applied on a dataset of 29 339 patients and found six times (316) more cachectic cancer patients than ICD codes (51).
Conclusions: PIES automatically discovers clinical signatures to characterize cancer patients with cachexia based on EPRs without external parties moving or touching patient data, which helped clinicians find more undiagnosed, misdiagnosed, and miscoded patients in a privacy preserving manner. NHS Lothian will apply PIES to 8000 lung and pancreatic cancer patients with a view to use PIES as part of the clinical care pathway and to help find more suitable patients for screening for new clinical trials and therapies. Additionally, PIES allows the clinical signature to evolve automatically, which helps clinicians address data heterogeneity and scale across multiple healthcare providers. PIES's ability to uncover novel insights through these clinical signatures across different hard-to-diagnose diseases will further facilitate research and drug development.
2-10
Correlation of preoperative body composition with postoperative complications and 30-day-mortality in 255 patients in resectable pancreatic cancer
Martin Henselmann and Tara Müller and Stefan Reischl and Marc Martignoni
Department of Surgery, Klinikum Rechts der Isar, School of Medicine, Technical University of Munich, Munich, Germany
Introduction: This study aimed to demonstrate the association between body composition parameters and postoperative complications including 30-day-mortality in patients with pancreatic cancer who underwent surgical therapy.
Methods: A total of 255 patients with pancreatic cancer who underwent surgery between 2007 and 2021 were included in the retrospective data analysis. For the corresponding question, the body composition of these patients was determined by analysis of CT images, which were taken up to 4 weeks before surgery, using the sliceOmatic software. The parameters were skeletal muscle, intermuscular adipose tissue, visceral adipose tissue, and subcutaneous adipose tissue at the level of the 3rd lumbar vertebra, standardized by body height resulting in SMI and FMI. Additionally examined variables included ASA score, unintentional weight loss within the last 6 months, BMI, as well as incidence and Clavien-Dindo classification of surgical complications and mortality within 30 postoperative days.
Results: SMI and FMI were determined in 255 patients with a mean value of 45.0 cm2/m2 (± 8.2 cm2/m2) and 102.6 cm2/m2 (± 50.1 cm2/m2), respectively. One hundred thirty-three patients had a low SMI (≤38.5 cm2/m2 for women and ≤52.4 cm2/m2 for men). 69.9% of patients with a low SMI had postoperative complications (Clavien-Dindo 1–5) and the 30-day mortality was 2.3%. In addition, BMI was determined in all patients, with a mean value of 24.6 kg/m2 (± 3.8); 8.6% had a BMI of < 20 kg/m2 in this regard. Among this group of patients, 72.7% had postoperative complications (Clavien-Dindo 1–5) and 4.5% died within the first 30 postoperative days.
Unintentional weight loss of more than 5 kg within the last 6 months preoperatively occurred in 31 of 255 documented patients. In those patients, postoperative complications could be found in 80.6% (Clavien-Dindo 1–5) and the 30-day mortality rate was 6.5%. In contrast, postoperative complications (Clavien-Dindo 1–5) occurred in only 67.9% of patients without this unintentional weight loss. In this group, 30-day mortality was 1.3%.
Conclusions: Changes of body composition and cachexia influence postoperative outcomes and should be considered in the management of pancreatic cancer patients. Regardless of the quality of the surgery, which is measured by the postoperative complications, the postoperative mortality rate remains relatively high. This can be explained by the patient's pre-operative poor general and nutritional condition. Therefore, it would be recommended to apply the concept of pre-habilitation in such patients.
2-11
Body composition endpoints in cancer cachexia clinical trials: a systematic review from the cachexia endpoints series
Leo R. Brown1, Mariana S. Sousa2, Michael S. Yule1, Judith Sayers1,3,4, Tora S. Solheim5, Barry J.A. Laird3,4 and Richard J.E. Skipworth1
1Clinical Surgery, University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;2Improving Palliative, Aged and Chronic Care through Clinical Research and Translation (IMPACCT), University of Technology, Sydney, Australia;3Institute of Genetics and Molecular Medicine, University of Edinburgh, Edinburgh, UK;4St Columba's Hospice, Edinburgh, UK;5European Palliative Care Research Centre, Norwegian University of Science and Technology, Trondheim, Norway
Introduction: Significant variation exists in the chosen outcomes utilized by cachexia trials. Heterogeneity within the literature is likely to adversely impact the development and approval of targeted therapies. The aim of this review is to summarize the endpoints, related to body composition, that have been utilized in cancer cachexia trials.
Methods: A systematic search of MEDLINE, EMBASE and Cochrane Library databases was conducted to identify prospective clinical trials, published between January 1990 and June 2021, which considered interventions aimed at attenuating the effects of cancer cachexia. Inclusion was irrespective of the modality of intervention (e.g. pharmacological, nutritional, physical exercise and behavioural) or comparator. The present study is one of six systematic reviews on outcomes used in cachexia trials, and will focus on radiological, bio-electrical and anthropometric endpoints pertaining to body composition.
Results: A total of 83 clinical trials, comprising 13 048 patients, were eligible for inclusion. While numerous primary tumour sites were considered, non-small cell lung and pancreatic cancer were the most frequently studied. The majority of trial interventions (52%) were pharmacological or nutritional (34%) in nature. The most frequently reported anthropometric endpoint was body weight (69 trials, n = 11 915) and over one third of trials (n = 26) noted differences between groups using this endpoint. Bio-impedance analysis (BIA) was the most commonly utilized radiological modality for body composition (23 trials, n = 3198). Only six studies (27%) identified a significant difference between trial groups using BIA-based measures. Sixteen trials (n = 3052) considered dual-energy X-ray absorptiometry (DEXA) based endpoints with significant differences between groups found in over half of these (56%). Computed tomography (CT) body composition was considered by seven trials, with a move towards this modality in more recent years. However, none of these trials detected any significant between-group differences using CT based estimates of body composition.
Conclusions: This systematic review has described the most frequently utilized body composition outcome measures in cancer cachexia clinical trials. While it is difficult to comment on the optimal endpoint for body composition, based on the heterogeneity within the existing literature, we describe several considerations to aid the design of future cachexia trials.
2-12
Oncological endpoints in cancer cachexia clinical trials: systematic review of cachexia endpoints
Iain Phillips1, Olav Dajani2, Ester Størckson2, Barry Laird3, Richard Skipworth3, Tora Solheim4 and Jann Arends5 and On behalf of Cachexia Clinical Trials Endpoints Group
1Edinburgh Cancer Center, Edinburgh, UK;2Department of Oncology, Oslo University Hospital, Oslo, Norway;3University of Edinburgh, Edinburgh, UK;4Norwegian University of Science and Technology, Trondheim, Norway;5University of Freiburg, Freiburg im Breisgau, Germany
Introduction: Cachexia affects outcomes for patients receiving anti-cancer treatment. These include reduced response rates to anticancer treatment, decreased survival and an increased incidence of adverse events.
To further understand the impact of cachexia on oncology outcomes, we aimed to identify which oncology endpoints have been reported in cachexia clinical trials.
Methodology: This systematic review was conducted according to the PRISMA statement and registered on the PROSPERO database. Six study groups collaborated to combine one search, creating one common data extraction table.
Ovid MEDLINE, EMBASE and Cochrane were searched for longitudinal studies and clinical trials. A hand search for additional relevant articles from references of key articles was conducted. Articles were eligible if they were: controlled trials aiming to treat/attenuate cachexia in adult patients with cancer, reported outcomes at >1 time point, published in full text from 1990 and were written in English. There were no restrictions on the type of intervention.
Primary outcomes investigated in this review were measures of oncological outcomes in cancer cachexia. These included: assessments of overall survival, progression free survival, response rate, completion of treatment and toxicity/adverse events.
Results: We identified 55 papers for further analysis. A further 101 papers met the manuscript criteria above, but did not include an oncology endpoint.
The commonest reported outcome was overall survival, reported in 85% of trials (see Table 1). Only 1 trial was positive. Toxicity/adverse events were reported in 21 trials (38%).
Twenty five (45%) of the studies were performed in a single tumour site: 8 in lung cancer, 6 in pancreatic cancer, 5 in Head and Neck cancers and 5 in GI cancers. The remaining 55% were basket studies. Forty-one studies (75%) were performed in stage 3–4 patients. Most studies (36/41, 65%) included patients receiving palliative anti-cancer drug treatment. Ten studies (18%) involved curative treatment and 4 studies (7%) included curative and palliative treatment.
The commonest interventions were pharmacological (47%) or nutritional (45%).
Conclusions: Oncology endpoints are principally included as secondary endpoints. These studies are heterogeneous for cancer type and treatment received. This may be the reason for the majority of studies reporting negative oncology endpoints.
The choice of appropriate oncology endpoints are likely to depend on the setting of the clinical trial, including: type of cancer, whether patients are receiving curative or palliative treatment, the type of oncology intervention, the type of cachexia intervention and the likely prognosis of the patient population being investigated.
2-13
Biomarkers in cancer cachexia clinical trials: systematic review of the cachexia endpoints series
Ross Dolan1, Mariana S. Sousa2, Alison Winaski1, Andrea Gonzalez1, Josh McGovern1, Richard J.E. Skipworth3, Tora S. Solheim4, Marie Fallo5,6, Donald McMillan1 and Barry J.A. Laird5,7 and On behalf of the Cachexia Endpoints Series Working Group
1Academic Department of Surgery, University of Glasgow, Glasgow Royal Infirmary, Glasgow, UK;2Improving Palliative, Aged and Chronic Care through Clinical Research and Translation (IMPACCT), University of Technology Sydney, Sydney, Australia;3Clinical Surgery University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;4European Palliative Care Research Centre, Norwegian University of Science and Technology, Trondheim, Norway;5St Columba's Hospice, Edinburgh, UK;6Cicely Saunders Institute of Palliative Care, Policy and Rehabilitation, Kings College, London, UK;7Edinburgh Cancer Research Centre, University of Edinburgh, Edinburgh, UK
Introduction: Over the course of the last decade systemic inflammation has moved towards central stage in the definition and diagnosis of cancer cachexia. While the basis of the systemic inflammatory response (SIR) in cancer patients is not fully understood, its prognostic ability is unquestioned. As a result, it is necessary for biomarkers including markers of the SIR to be incorporated into future endpoints for any cancer cachexia trials.
Methods: This systematic review is part of a series which examines multiples endpoints in cancer cachexia clinical trials and specifically addresses measures of SIR. The extensive literature review was carried out in the MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials databases. Clinical trials conducted between January 1990 and June 2021 that assessed SIR as a study endpoint were eligible.
Results: There were 56 controlled trials identified for inclusion with data from 6488 patients. Interventions varied from pharmacological (n = 23), multimodal (n = 17) and nutritional (n = 16). Most trials (n = 28) included people with varied primary cancer sites, followed by trials specific to gastrointestinal (n = 9), lung (n = 8) and pancreatic cancers (n = 4). Studies were conducted across the globe with multinational trials (n = 8) most frequently reported, followed by trials based in the USA (n = 7) and the UK (n = 4). The most frequently reported endpoint for SIR in cancer cachexia trials was albumin (n = 32 trials) containing data on 2969 patients. Out of these, about 40% noted significant results.
Conclusions: Work to date suggests albumin is the most used measure of SIR in cancer cachexia clinical trials.
2-14
The relationship between appetite and lean body mass as endpoints in cancer cachexia interventional clinical trials: a systematic review
Eilidh Fraser1, Tora Solheim2, Richard Skipworth3, Inger Ottestad2, Asta Bye4, Trude Balstad2, Christine Greil5 and Ola Magne Vagnildhaug2
1University of Edinburgh, Edinburgh, UK;2Norwegian University of Science and Technology, Trondheim, Norway;3Clinical Surgery University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;4European Palliative Care Research Centre (PRC), Oslo, Norway;5Faculty of Medicine, University of Frieburg, Freiburg im Breisgau, Germany
Introduction: There are currently no approved therapeutics for cancer cachexia. Co-primary endpoints, assessing endpoints such as physical function and/or nutrition in addition to body composition endpoints, have been requested in cancer cachexia clinical trials. Failure of therapeutic regulatory approval has recently been due to inadequate improvement in function co-primary endpoints. It has been suggested this may be due to a non-linear relationship between physical function and lean body mass (LBM). This review aims to determine the relationship LBM and appetite. To understand if a linear relationship exists, and to determine the acceptability of utilizing LBM and appetite as body composition and nutrition co-primary endpoints in cachexia clinical trials. This will aid the research regarding optimum endpoints in cancer cachexia clinical trials.
Methods: Relevant studies published between 1990 and June 2021 were retrieved through an extensive literature search of electronic databases Medline, Embase and Cochrane. Eligible studies had sample sizes > 40, participants >18 years old with cancer cachexia interventions of ≥14 days. Included studies were required to measure appetite and LBM as endpoints. Records were reviewed by two independent reviewers and PRISMA guidance was followed.
Results: 5976 studies were identified from the literature search of which 14 were eligible to be included. Studies varied in intervention type (11 pharmacological, 3 multimodal), intervention time (2–26 weeks), mean baseline appetite (mean 4.7 ± 1.83), mean baseline LBM (40.2 ± 8.53 kg), methods of recording appetite (VAS, NRS, EORTC QLQ-C30, QoL-ACD) and methods of recording LBM (DEXA, BIA, CT). Seven studies provided appropriate mean appetite change data, which was able to be correlated with mean LBM change. Pearson's correlation between mean appetite change and mean LBM change was 0.539 (P = 0.212). Controlling for numerical co-variables (baseline appetite, baseline LBM and intervention time) a partial correlation of 0.968 (P = 0.032) was observed.
Conclusions: Inadequate evidence was available to conclude a valid correlation between appetite and LBM within cancer cachexia clinical trials. Further research is required to enhance findings.
2-15
The impact of acute systemic inflammation and the metabolic response to surgery on computed tomography body composition analyses
Leo R. Brown1, Michael I. Ramage1, Nikki Bruce2, Lachlan Dick3, Sharukh Sami4, Judith Sayers1 and Richard J.E. Skipworth1
1Clinical Surgery, University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;2Department of General Surgery, Borders General Hospital, Melrose, UK;3Department of General Surgery, Victoria Hospital, Kirkcaldy, UK;4Department of General Surgery, Dumfries and Galloway Royal Infirmary, Dumfries, UK
Aim: Body composition has been used extensively for prognostication across malignant and benign diseases. Systemic inflammation is both a key driver of cancer cachexia and a common finding in patients presenting with acute pathology. However, its influence on body composition is poorly understood. This study aimed to longitudinally assess computed tomography (CT) body composition, in patients who experienced an anastomotic leak post-oesophagectomy, as a model of acute, severe systemic inflammation.
Methods: Consecutive patients who suffered an anastomotic leak, following oesophagectomy, between 1 January 2012 and 1 January 2022 were identified from a prospectively maintained database. Changes in body composition were assessed across staging, pre-operative, post-complication and follow-up scans at the L3 vertebral level.
Results: Twenty patients (median 65 years, 90% male) were included. Of these, 15 underwent neoadjuvant chemo (radio)therapy. Body composition was not altered by neoadjuvant treatment. Following surgery and anastomotic leak, a decrease in skeletal muscle volume (mean difference: −68.06 cm3, P = 0.028) was noted. Estimates of intramuscular and subcutaneous adipose tissue conversely increased (P = 0.038 and P = 0.039, respectively). Skeletal muscle density fell while adipose densities were higher following anastomotic leak. Although tissue radiodensity and subcutaneous fat volumes normalized on follow-up CT scans, skeletal muscle volume remained below pretreatment levels.
Conclusions: Acute systemic inflammation has a marked effect on body composition analyses. Decreased muscle volume and increased volumes of adipose tissue were evident following the inflammatory insult. Radiodensity across muscle and adipose tissues trended towards that of water, likely secondary to oedema. Research utilizing body composition variables should be interpreted with consideration of the potential of influence of underlying inflammatory status.
2-16
An international survey on nutritional issues in patients with cancer: preliminary results
Giovanni Imbimbo1, Alessio Molfino1, Juan-Jose Ventura2, Joost Wesseling3, Karin Kastrati4 and Maurizio Muscaritoli1
1Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2European Cancer Patient Coalition, Brussels, Belgium;3The European Nutrition for Health Alliance, Amsterdam, The Netherlands;4Klinik für Innere Medizin II, University Hospital Jena, Jena, Germany
*These authors equally contributed.
Introduction: Nutritional disorders are common in patients with cancer and can lead to poor quality of life and survival. By the present international survey, we aimed at assessing the patients' perspectives on different nutritional aspects during cancer journey.
Methods: This survey was developed by Das Lebenshaus with The European Cancer Patient Coalition (ECPC) and The European Nutrition for Health Alliance (ENHA), and designed and analysed by researchers from Sapienza University of Rome. The majority of the participants were from Germany, Italy, United Kingdom and Hungary. The survey consisted of 46 questions on different nutritional issues. For this analysis, we considered the most relevant questions related to nutritional alterations.
Results: The survey reached 1010 patients with cancer. The mean age of the participants was 55 ± 14 y. Based on the answers available, the most represented cancer type was breast (28%) and renal (16%); a recent diagnosis of cancer was performed in 35%, whereas 27% were diagnosed more than 8 years before. About 40% of the participants reported eating problems, such as loss of appetite (116/252) (46%), nausea (119/252) (47%), diarrhoea (114/252) (45%). Regarding quality of life, patients answering on impact of nutritional problems reported a score of 3.5 ± 1.1 (from 1 = no impact, to 5 = extremely negative impact); 441/672 (66%) reported that ‘rarely or never a physician or a member of the cancer care team asked about any feeding problems’, and 483/670 (72%) believe that ‘oncology team do not take care of nutritional issues‘; 176/643 (27%) of the participants reported unvoluntary body weight loss and 138 out of 153 (90%) presented no awareness about the risk of not receiving anticancer treatment for this reason.
Conclusions: Patients with cancer largely experienced nutritional alterations with a negative impact on quality of life. Well-structured health-care programs for nutritional intervention are needed.
2-17
Non-steroidal anti-inflammatory drugs for treatment of cancer cachexia: a systematic review
Megan Bowers1, Brittany Cucchiaro2 and Adrian Slee3
1Cicely Saunders Institute of Palliative Care, Policy & Rehabilitation, Florence Nightingale Faculty of Nursing, Midwifery & Palliative Care, King's College London, Bessemer Road, London, UK;2Division of Medicine, Faculty of Medical Sciences, University College London, London, UK;3Division of Medicine, Faculty of Medical Sciences, University College London, London, UK
Introduction: The objective of this review was to assess the efficacy and safety of non-steroidal anti-inflammatory drugs (NSAIDs) on patient-centred outcomes in patients with cancer cachexia (CC). This review is needed, as two systematic reviews on this topic, published in 2013, concluded there was not sufficient evidence to recommend the use of NSAIDs for clinical management of CC outside of clinical trials. However, recent clinical trials of multimodal CC interventions have included NSAIDs as an intervention component, so an up-to-date assessment of the evidence for NSAIDs in the treatment of CC is warranted.
Methods: Four databases (MEDLINE, EMBASE, CENTRAL, CINAHL) and three trial registers (ClinicalTrials.gov, WHO ICTRP, ISRCTN) were searched on 16/12/2022. Randomized controlled trials (RCTs) comparing any NSAID (any dose or duration) with a control arm, in adult patients with CC, reporting measures of body weight, body composition, nutrition impact symptoms, inflammation, performance status or fatigue, were eligible for inclusion. Outcome classification was determined through patient involvement activities; primary outcomes were survival, changes in muscle strength, body composition, body weight, and quality of life. Included studies were assessed for risk of bias using the Revised Cochrane risk-of-bias tool for randomized trials.
Results: Five studies were included, which investigated Indomethacin (n = 1), Ibuprofen (n = 1) and Celecoxib (n = 3). Risk of bias was high; four studies were judged to be at high risk for all outcomes, and one study was at high risk for some outcomes and raised concerns for all others. Considerable clinical and methodological heterogeneity among the studies meant that meta-analysis was not appropriate. There was insufficient evidence to determine whether Indomethacin or Ibuprofen are effective or safe for use in patients with CC; RCTs with lower risk of bias are needed. Results from Celecoxib studies indicated it was safe for use in this population at the doses tested (200–400 mg/day), but found contrasting results regarding efficacy, potentially reflecting heterogeneity among the studies.
Conclusions: At present, there is inadequate evidence to recommend any NSAID for clinical practice in the management of CC. Whilst current clinical studies in the field of treating CC are shifting towards multimodal interventions, further research to determine the efficacy and safety of NSAIDs alone is necessary if they are to be included in such multimodal interventions. Furthermore, the lack of data on patient-determined primary outcomes in this review highlights the need for patient and public involvement in clinical trials for CC.
2-18
The mortality burden of cachexia in patients with non-small cell lung cancer: a meta-analysis
Philip D. Bonomi1, Jeffrey Crawford2, Richard F. Dunne3, Eric J. Roeland4, Karen E. Smoyer5, Mohd K. Siddiqui6, Thomas D. McRae7, Michelle I. Rossulek8, James H. Revkin8 and Lisa C. Tarasenko7
1Rush University Medical Center, Chicago, IL, USA;2Duke Cancer Institute, Duke University Medical Center, Durham, NC, USA;3Department of Medicine and Wilmot Cancer Institute, University of Rochester Medical Center, Rochester, NY, USA;4Knight Cancer Institute, Oregon Health and Science University, Portland, OR, USA;5Envision Pharma Group, Philadelphia, PA, USA;6EBM Health Consultants, Delhi, India;7Pfizer Inc, New York, NY, USA;8Pfizer Inc, Cambridge, MA, USA
Introduction: Cachexia and weight loss [WL] have been linked to poor outcomes in patients with cancer. This study's aim was to conduct a meta-analysis to estimate the mortality risk associated with cachexia in patients with non-small cell lung cancer (NSCLC) in studies identified through a systematic literature review (SLR).
Methods: Following a feasibility assessment, a meta-analysis evaluating cancer cachexia's impact (per International Consensus criteria [ICC] or previous WL ≥ 5% [without specifying a 6-month duration]) on overall survival (OS) in patients with NSCLC was conducted. The impact of heterogeneity was evaluated through sensitivity and subgroup analyses. Standard measures of statistical heterogeneity were calculated for each meta-analysis. We evaluated clinical heterogeneity by assessing variation in study characteristics, patient populations, and outcome definition.
Results: Of the 40 NSCLC publications identified in the SLR, 20 (50%) used the ICC definition or reported WL ≥ 5%. Sixteen studies (80%, n = 6225 patients, published 2016–2021) met the criteria for inclusion in the meta-analysis: 11 (69%) studies per ICC and 5 (31%) studies per WL ≥ 5%. Combined criteria (ICC or WL ≥ 5%) were associated with 82% higher mortality risk versus no cachexia or WL < 5% (pooled hazard ratio [95% CI]: 1.82 [1.47, 2.25]). A subgroup analysis of studies using the ICC definition (hazard ratio [95% CI]: 2.26 [1.80, 2.83]) or WL ≥ 5% (hazard ratio [95% CI]: 1.28 [1.12, 1.46]) showed consistent findings. Although statistical heterogeneity (I-square = 88%) was high across studies, a meta-influence analysis did not identify any potential outliers. Additionally, the results of sensitivity and subgroup analyses were consistent with the base-case analysis. Cumulative meta-analyses by publication year or data collection midpoint identified no time-varying effect, indicating results were robust to the differing timeframes of publication or data collection. No substantial publication bias, measured via funnel plot analysis, was identified in the meta-analysis.
Conclusions: ICC-defined cachexia or WL ≥ 5% were associated with inferior OS in patients with NSCLC. Identifying cachexia or WL ≥ 5% for patients with NSCLC has important implications for prognosis, treatment, and participant selection for interventional cachexia trials.
The role of body composition and pulmonary function in predicting survival after surgery for resectable lung cancer
Koen C.H.A. Verkoulen1, Yvonne L.J. Vissers1, Karel W.E. Hulsewé1, Steven W.M. Olde Damink2, David P.J. van Dijk1,2 and Erik R. de Loos1
1Department of Surgery, Division of General Thoracic Surgery, Zuyderland Medical Center, Heerlen, The Netherlands;2Department of Surgery, Maastricht University Medical Centre, Maastricht, The Netherlands
*These authors contributed equally.
Introduction: TNM-classification is widely used to stage patients with non-small cell lung cancer (NSCLC) and is the major determinant of appropriate treatment and prognosis. Host factors such as body composition and pulmonary function are barely considered in predicting long term outcome for these patients. The goal of this study was to assess body composition and pulmonary function as predictors of overall survival in patients undergoing surgery for NSCLC. The second objective of this study was to assess the association of body composition with pulmonary function.
Methods: A prospective cohort of NSCLC patients undergoing surgical resection was used. Abdominal CT-scans were analysed at the L3-vertebra level. Skeletal muscle (SM), visceral adipose tissue (VAT), and subcutaneous adipose tissue (SAT) mass and radiation attenuation (RA) were assessed. Pulmonary function was defined as the forced expiratory volume in 1 second (FEV1). SM, VAT and SAT were corrected for sex and age by calculating Z-scores. Multivariable cox-regression analysis was used for survival analysis. Multivariate linear regression was used to assess the association between body composition and FEV1.
Results: 475 NSCLC patients had an abdominal CT-scan suitable for body composition analysis. The majority of patients underwent lobectomy (82%), followed by pneumonectomy (7%), bilobectomy (6%), and wedge resection (5%) one patient underwent segmentectomy. Overall mean survival was 59 months. Old age (HR 1.042, 95% CI 1.027–1.058), ASA III-classification (HR 2.152, 95% CI 1.170–3.960), and high SAT-RA (HR 1.155, 95% CI 1.031–1.294) were associated with shorter overall survival in multivariable analysis. High FEV1 (HR 0.987 95% CI 0.981–0.993) was associated with longer survival. Both ASA-III classification (B = −9.562, 95% CI −17.648 to −1.476, P = 0.021) and SM-RA (B = 2.197, 95% CI 0.232–4.161, P = 0.028) were associated with FEV1 in multivariable linear regression analysis.
Conclusions: Both SAT-RA and FEV1 are strongly associated with overall survival in surgically treated NSCLC patients. SM-RA is significantly associated with FEV1. These are readily available parameters in the standard work-up of NSCLC patients and could play a role in decision making and possible enhanced prehabilitation.
2-20
Prospective characterization of cancer cachexia in patients with advanced cancer
Judith Sayers1,2,3, Leo R. Brown1, Richard J.E. Skipworth1 and Barry J.A. Laird2,3
1Clinical Surgery, University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;2St Columba's Hospice, Edinburgh, UK;3Institute of Genetics and Cancer, University of Edinburgh, Edinburgh, UK
Introduction: Cancer cachexia is a complex metabolic syndrome, with a multifactorial aetiology and widespread clinical effects. To date, there has been little work examining the different clinical phenotypes within the cachexia syndrome, or the interactions between tumour, systemic inflammation and clinical phenotype. Robust characterization is required to direct future research, provide meaningful trial endpoints and improve patient care.
Methods: Patients with a diagnosis of incurable cancer were recruited from outpatient oncology, palliative care and hospice settings in Edinburgh, UK and enrolled in the Revolution Study, a prospective observational study aiming to characterize people with incurable cancer across five cachexia phenotypic areas. (1) Body composition was assessed using weight, BMI and CT-assessed sarcopenia, (2) physical activity was examined using physical activity monitors and Karnofsky performance status, (3) symptoms were examined using validated questionnaires (functional assessment of anorexia/cachexia therapy scale, Patient Generated Subjective Global Assessment–Short Form, Hospital Anxiety and Depression Scale (HADS) and Eating Assessment Tool– 10), (4) quality of life was assessed using the European Organization for the Research and Treatment of Cancer–Quality of Life Questionnaire–C30, and (5) systemic inflammation was examined through analysis of blood samples for markers of the inflammatory response including white cell count, C-reactive protein, lactate dehydrogenase and albumin.
Results: We present the results for the first 90 patients recruited, with longitudinal data for 12 week follow up period available for a subset of patients (n = 28). We compared demographic, pathologic and treatment data to clinical and biological phenotypic data and assessed for key differences between weight-losing, weight stable and sarcopenic patient groups. Modified Glasgow Prognostic Score (mGPS) was correlated with survival data.
Conclusions: There is a need for robust characterization of people with incurable cancer, to understand underlying clinical phenotypes and guide future research. We present initial data from a prospective characterization study which can be used to better understand the ‘symptom phenotypes’ within the cachexia syndrome and correlate these with systemic inflammatory and body composition profiles.
2-22
Assessment of lipolysis biomarkers in subcutaneous adipose tissue of gastrointestinal cancer patients
Giovanni Imbimbo1, Federica Tambaro1, Elisabetta Ferraro2, Martina Andreini1, Michele Melena1, Maria Ida Amabile1, Giulia Lauteri3, Giuseppe Nigri3, Maurizio Muscaritoli1 and Alessio Molfino1
1Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2Department of Biology, University of Pisa, Pisa, Italy;3Department of Medical-Surgical Sciences and Translational Medicine, Sapienza University of Rome, Rome, Italy
Introduction: Lipolysis was shown to be involved in adipose tissue loss during cachexia. However, these mechanisms are not completely clarified in patients with cancer. We assessed the expression levels of lipolysis-associated genes in subcutaneous adipose tissue (SAT) of newly diagnosed gastrointestinal (GI) cancer patients according to the presence/absence of cachexia.
Methods: We considered patients with GI cancer at their first diagnosis and controls undergoing surgery for tumour resection and for benign diseases, respectively. Cachexia was defined as involuntary body weight loss > 5% in the prior 6 months. We collected SAT samples during the first phases of surgery. RNA was extracted from SAT and expression levels of ATGL, HSL, PPARα and MCP1 were analysed by qRT-PCR.
Results: We enrolled 24 cancer patients (pancreatic, gastric and colorectal) and 15 controls. Cancer patients did not differ from controls in terms of BMI. We found significant upregulation of ATGL and HSL in GI cancer patients with respect to controls (P = 0.008, P = 0.006). We observed a trend of increased mRNA levels of PPARα (P = 0.055) in GI cancer patients compared to controls, whereas no significant difference was observed in MCP1 levels. Comparing to controls, we found an upregulation of ATGL in GI cancer patients with cachexia (P < 0.05), and also in the group without cachexia (P = 0.02). HSL levels resulted upregulated in GI cancer patients with cachexia (P = 0.02), without cachexia (P = 0.02), compared to controls. We found an upregulation of ATGL in gastric patients compared to controls (P = 0.01) and higher HSL levels in gastric cancer and in pancreatic cancer compared to controls (P < 0.04).
Conclusions: In our cohort of gastrointestinal cancer patients, we found a modulation in the expression of genes of lipolysis and significant differences in their levels according to cancer type.
2-23
Effect of malnutrition risk on the association between skeletal muscle index and health-related quality of life and survival in upper gastrointestinal cancer
Lauren Hanna1,2, Kay Nguo2, Judi Porter2,3, Daniel Croagh4,5 and Catherine E. Huggins2,6
1Department of Nutrition and Dietetics, Monash Health, Clayton, Australia;2Department of Nutrition, Dietetics and Food, Monash University, Clayton, Australia;3Institute for Physical Activity and Nutrition, School of Exercise and Nutrition Sciences, Deakin University, Geelong, Australia;4Department of Upper Gastrointestinal Surgery, Monash Health, Clayton, Australia;5Department of Surgery, Monash University, Clayton, Australia;6Globe Obesity Centre (GLOBE), Institute for Health Transformation, Deakin University, Burwood, Australia
Introduction: Low skeletal muscle index (SMI) is an established prognostic indicator in cancer1, and may also be associated with poor health-related quality of life (HRQOL)2. Presence or risk of malnutrition is also associated with poor survival and HRQOL outcomes3,4, yet this confounding factor is rarely accounted for in studies investigating the consequences of low SMI. Malnutrition is prevalent in upper gastrointestinal (GI) cancer5, therefore this study examined the effect of malnutrition risk on the association between SMI at diagnosis of upper GI cancer, and both HRQOL at diagnosis and survival over the following year.
Methods: A prospective study was conducted using data from participants enrolled in a randomized controlled trial at diagnosis of oesophageal, gastric or pancreatic cancer6. Baseline data included: SMI from diagnostic computed tomography imaging, malnutrition risk (PG-SGA Short Form, PG-SGASF7), and HRQOL (EORTC-QLQ C30)8. Low SMI was identified using sex-specific thresholds9. The correlation between SMI and PG-SGASF scores was examined, and multiple linear regression was used to identify contributors to variation in HRQOL at baseline. Predictors of mortality within 12 months of diagnosis were investigated using Cox proportional hazards regression.
Results: The study included 105 treatment-naive patients with oesophageal (43%), gastric (20%), or pancreatic (37%) cancers. The cohort was 68% male, mean age 65.9 (SD ± 10.0) years; 56% of patients had low SM1, and 49% were at high risk of malnutrition (PG-SGASF score ≥9)10. SMI was weakly, negatively correlated with PG-SGASF score (r = −0.268, P = 0.006), and some HRQOL domains (physical and role functioning, summary score11, all P < 0.05). When adjusted for PG-SGASF score, SMI was not significantly associated with any measure of HRQOL at baseline. Higher PG-SGASF scores were independently associated with lower HRQOL across all scales. Advanced (unresectable) disease at diagnosis was independently associated with 12-month mortality (HR 2.643, 95% CI 1.041–6.711, P = 0.041), adjusting for baseline PGSGASF score and cancer type; baseline SMI was not prognostic. In a subgroup analysis of those with resectable/borderline resectable disease (n = 52), high PG-SGASF score (≥9) at diagnosis was the only variable associated with 12-month mortality (HR 4.539, 95% CI 1.012–20.352, P = 0.048).
Conclusions: Malnutrition risk measured by the PG-SGASF was a stronger predictor of poorer HRQOL and survival than SMI, and should be included as a covariate in future studies investigating the effect of low SMI on these outcomes in people with cancer.
1. Shachar, SS, Williams, GR, Muss, HB, Nishijima, TF. Prognostic value of sarcopenia in adults with solid tumours: A meta-analysis and systematic review. Eur J Cancer.2016; 57: 58–67.
2. Hanna, L, Nguo, K, Furness, K, Porter, J, Huggins, CE. Association between skeletal muscle mass and quality of life in adults with cancer: a systematic review and meta-analysis. Journal of Cachexia, Sarcopenia and Muscle.2022; 13(2): 839–57.
3. Lis, CG, Gupta, D, Lammersfeld, CA, Markman, M, Vashi, PG. Role of nutritional status in predicting quality of life outcomes in cancer–a systematic review of the epidemiological literature. Nutr J.2012; 11(1):1–18, 27.
4. Zhang, X, Tang, T, Pang, L, Sharma, SV, Li, R, Nyitray, AG, Edwards, BJMalnutrition and overall survival in older adults with cancer: A systematic review and meta-analysis. J Geriatr Oncol.2019; 10(6): 874–83.
5. Hébuterne, X, Lemarié, E, Michallet, M, Montreuil, CB, Schneider, SM, Goldwasser, F. Prevalence of Malnutrition and Current Use of Nutrition Support in Patients With Cancer. J Parenter Enter Nutr.2014; 38(2): 196–204.
6. Huggins, CE, Hanna, L, Furness, K, Silvers, MA, Savva, J, Frawley, H, Croagh, D, Cashin, P, Low, L, Bauer, J, Truby, H, Haines, TPEffect of early and intensive telephone or electronic nutrition counselling delivered to people with upper gastrointestinal cancer on quality of life: a three-arm randomized controlled trial. Nutrients.2022; 14(15): 3234.
7. Ottery, FD. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition.1996; 12(1 Suppl): S15–9.
8. Aaronson, NK, Ahmedzai, S, Bergman, B, Bullinger, M, Cull, A, Duez, NJ, Filiberti, A, Flechtner, H, Fleishman, SB, Haes, , Kaasa, S, Klee, M, Osoba, D, Razavi, D, Rofe, PB, Schraub, S, Sneeuw, K, Sullivan, M, Takeda, FThe European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst.1993; 85(5): 365–76.
9. Martin, L, Birdsell, L, Macdonald, N, Reiman, T, Clandinin, MT, McCargar, LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol.2013; 31(12): 1539–47.
10. Jager-Wittenaar, H, Bats, HF, Welink-Lamberts, BJ, Gort-van Dijk, D, Laan, BFAM, Ottery, FD, et al. Self-completion of the patient-generated subjective global assessment short form is feasible and is associated with increased awareness on malnutrition risk in patients with head and neck cancer. Nutr Clin Pract.2020; 35(2): 353–62.
11. Giesinger, JM, Kieffer, JM, Fayers, PM, Groenvold, M, Petersen, MA, Scott, NW, Sprangers, MA, Velikova, G, Aaronson, NK,
EORTC Quality of Life GroupReplication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol.2016; 69: 79–88.
2-24
Adipose tissue radiation attenuation is an independent predictor of chemotherapy toxicity and shorter overall survival in metastatic colorectal cancer patients
Yan Sun1, Isabel M. van Ruijven2, David P.J. van Dijk1, Ralph Brecheisen1, Nicolette Wierdsma2, Sander S. Rensen1 and Steven M.W. Olde Damink1,3
1Department of Surgery, NUTRIM School of Nutrition and Translational research in Metabolism, Maastricht University, Maastricht, The Netherlands;2Department of Nutrition & Dietetics, Amsterdam UMC, Amsterdam, The Netherlands;3Department of Visceral and Transplantation Surgery, RWTH Aachen University, Aachen, Germany
Introduction: Skeletal muscle mass and radiodensity have been shown to be associated with chemotherapy toxicity and survival of cancer patients. However, little is known about the clinical significance of adipose tissue radiodensity, which has been hypothesized to be associated with tissue inflammation and insulin resistance. We investigated the association between adipose tissue radiodensity, chemotherapy toxicity, and survival in patients with metastatic colorectal cancer (mCRC).
Methods: 104 patients of a prospective cohort of mCRC patients treated with standard first-line chemotherapy were included into this study. Using diagnostic abdominal CT scans, we assessed height adjusted area and radiation attenuation (RA) of skeletal muscle (SM), visceral adipose tissue (VAT), and subcutaneous adipose tissue (SAT) at the third lumbar vertebra. Associations between these body composition parameters and overall survival as well as chemotherapy toxicity (CTCAE v4.03) were evaluated using univariable and multivariable logistic and cox regression analysis, respectively. Body composition variables were corrected for covariates including age, sex, nutritional support, and chemotherapy regimen.
Results: Forty-four patients (42.3%) developed grade 3–4 toxicity. Pretreatment VAT-RA was independently associated with grade 3–4 toxicities (OR = 0.912, 95% CI 0.843–0.987, P = 0.022). Chemotherapy regimen and nutritional support were not associated with chemotoxicity. SAT-RA and chemotoxicity grade 3–4 were associated with shorter overall survival (HR = 1.044, 95% CI 1.016–1.072, P = 0.002 and HR = 2.334, 95% CI 1.337–4.074, P = 0.003, respectively). When stratifying patients for SAT-RA and chemotoxicity grade 3–4, patients with low SAT-RA and no chemotoxicity grade 3–4 had a significantly longer overall survival compared with patients with either high SAT-RA or chemotoxicity grade 3–4 or both (109.0 months compared with 28.2 months and 17.7 months, respectively, log rank P < 0.001).
2-25
The prognostic impact of pretreatment cachexia in resectional surgery for oesophagogastric cancer: a systematic review, meta-analysis, and meta-regression
Leo R. Brown1, Judith Sayers1, Michael S. Yule1, Thomas M. Drake2,3, Ross D. Dolan4, Donald C. McMillan4, Barry J.A. Laird5, Stephen J. Wigmore1 and Richard J.E. Skipworth1
1Clinical Surgery, University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK;2Centre for Medical Informatics, University of Edinburgh, Edinburgh, UK;3Cancer Research UK Beatson Institute, Glasgow, UK;4Academic Unit of Surgery, University of Glasgow, Glasgow Royal Infirmary, Glasgow, UK;5Institute of Genetics and Cancer, University of Edinburgh, Edinburgh, UK
Background: Cancer cachexia is not purely an end-stage phenomenon and can even influence the outcomes of patients with potentially curable disease. This review examines the effect of pretreatment cachexia on overall survival, in patients undergoing surgical resection of an oesophagogastric cancer.
Methods: A systematic literature search of MEDLINE, EMBASE and Cochrane Library databases was conducted, from January 2000 to May 2022, to identify studies reporting the influence of cachexia on patients undergoing an oesophagogastric resection for cancer with curative intent. Meta-analyses of the primary (overall survival) and secondary (disease-free survival and postoperative mortality) outcomes were performed using random-effects modelling. Meta-regression was used to examine disease stage as a potential confounder.
Results: Ten non-randomized studies, comprising 7186 patients, were eligible for inclusion. The prevalence of pretreatment cachexia was 35% (95% CI: 24–47%). Pooled adjusted hazard ratios showed that cachexia is adversely associated with overall survival (HR 1.46, 95% CI: 1.31–1.60, P < 0.001). Meta-analysis of proportions identified decreased overall survival at 1, 3 and 5 years in cachectic cohorts. Pretreatment cachexia was not a predictor of disease-free survival and further data are required to establish its influence on postoperative mortality. The proportion of patients with stage III/IV disease was a significant moderator of between-study heterogeneity (P = 0.027). Cachexia may have a greater influence on overall survival in studies where more patients have a locally advanced malignancy.
Conclusions: Pretreatment cachexia adversely influences overall survival following resection of an oesophagogastric malignancy. Consideration of cachexia, during the shared decision-making process, may improve risk-stratification and facilitate targeted interventions.
2-26
Progressive loss of bone density in patients with oesophageal cancer
Miles Cameron1,2, Ziad Awad3, Sarah Judge1 and Andrew Judge1
1Department of Physical Therapy, University of Florida, Gainesville, FL, USA;2MD-PhD Training Program, University of Florida, Gainesville, FL, USA;3Department of Surgery, University of Florida, Jacksonville, FL, USA
Background: Changes in body composition are common in oesophageal cancer (EC). More than 60% of patients, regardless of stage, display signs of cachexia, including weight loss, skeletal muscle atrophy and fat wasting. In the current study, we questioned whether bone density also decreases in patients with EC and associates with oncologic outcomes.
Methods: We performed a retrospective review of all patients that received esophagectomy between 2015 and 2020 at University of Florida Health. Patients with pre-existing cardiac disease were excluded. Body composition was measured using PET/CT scans, and patients were classified as having cachexia/myopenia if having an L3 skeletal muscle index below sex- and BMI-dependent cut-offs. A P-value <0.05 was considered statistically significant.
Results: Bone density was significantly reduced in patients with cachexia relative to those with normal muscle mass (108 ± 37.2 HU vs. 146 ± 55.0 HU, P = 0.003). Furthermore, bone density correlated with muscle mass (P < 0.0001, R = 0.5055) and muscle quality/radiodensity (P = 0.0002, R = 0.4736). Mean rate of bone loss was −12.0 ± 27.9 HU/100d between initial and re-staging imaging studies after neoadjuvant therapy. Patients with regional lymph node metastases at surgery (N1–3) had more bone loss than those with N0 disease (−26.6 ± 30.8 HU/100d vs. −2.71 ± 22.1 HU/100d, P = 0.03). Similarly, progressive loss of bone was observed in patients with positive Lymphovascular (LV)invasion (−41.8 ± 32.6 HU/100d vs. −3.53 ± 20.1 HU/100d, P = 0.005) and positive perineural (PN) invasion (−29.8 ± 32.4 HU/100d vs. −3.12 ± 21.1 HU/100d, P = 0.01).
3-01
Prognostic value of weight loss in hospitalized patients with acute heart failure
1Department of Medical Science and Cardiorenal Medicine, Yokohama City University Graduate School of Medicine, Yokohama, Japan;2Division of Cardiology, Yokohama City University Medical Center, Yokohama, Japan;3Department of Cardiology, Yokohama City University School of Medicine, Yokohama, Japan;4Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan;5Department of Cardiology, The Sakakibara Heart Institute of Okayama, Okayama, Japan;6Department of Digital Health and Telemedicine R&D, Juntendo University, Tokyo, Japan;7Department of Rehabilitation, School of Allied Health Sciences, Kitasato University, Sagamihara, Japan;8Department of Rehabilitation, Kameda Medical Centre, Kamogawa, Japan;9Department of Cardiovascular Medicine, Kitasato University School of Medicine, Sagamihara, Japan;10Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Centre, Osaka, Japan
Introduction: Weight loss is a known poor prognostic factor in patients with chronic heart failure (HF). Whether weight loss is a poor prognostic factor in patients with acute HF is unknown. In this study, we aimed to investigate the prognostic value of weight loss in patients hospitalized for acute HF.
Methods and Results: This study was a post-hoc analysis of the FRAGILE-HF study, a prospective multicenter observational study that included 1332 hospitalized older (≥65 years) patients with HF. The primary outcome was all-cause death within 2 years of discharge. The self-reported body weight 1 year prior to hospital admission was available in 1106 patients (83.0%) and was compared with their weight before discharge after decongestion therapy. The mean weight change was −7.4 ± 8.3% and 86.8% of the overall cohort experienced any weight loss. Whereas patients with weight loss ≥5%, which is a well-validated cut-off in chronic HF, showed comparable mortality to those with less weight loss (P = 0.955 by log-rank), patients with weight loss ≥12%, the lowest quartile value, showed higher mortality than those with less weight loss or no weight loss (P = 0.024 by log-rank; figure). In a Cox proportional hazard model, weight loss ≥12% was associated with high mortality after adjustment with the known prognostic factors (age, gender, current smoking, NYHA class, ejection fraction, serum creatinine, systolic blood pressure, body mass index, past history of diabetes, chronic obstructive pulmonary disease, HF, medication, and log B-type natriuretic peptide; adjusted hazard ratio: 1.58 [1.14–2.19], P = 0.006).
3-02
Circulating microRNA-22 as an innovative biomarker in patients with sarcopenia and heart failure: results from the SICA-HF
Mirela Vatić1,2, Anselm A. Derda3,4, Tania Garfias-Veitl1,2, Goran Lončar1,5,6, Ryosuke Sato1, Guglielmo Fibbi1, Wolfram Doehner7,8,9, Stefan D. Anker7,9,10, Thomas Thum3,11,12 and Stephan von Haehling1,2
1Department of Cardiology and Pneumology, University of Goettingen, Goettingen, Germany;2German Center for Cardiovascular Reserach (DZHK), partner site Goettingen, Goettingen, Germany;3Institute of Molecular and Translational Therapeutic Strategies (IMTTS), Hannover Medical School, Hannover, Germany;4Department of Cardiology and Angiology, Hannover Medical School, Hannover, Germany;5Dedinje Cardiovascular Institute, Belgrade, Serbia;6Faculty of Medicine, University of Belgrade, Belgrade, Serbia;7Berlin-Brandenburg Center for Regenerative Therapies (BCRT), Charité University, Medical Center Berlin, Berlin, Germany;8Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany;9German Center for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany;10Division of Cardiology and Metabolism - Heart Failure, Cachexia & Sarcopenia, Department of Cardiology (CVK), Charité University Medical Center Berlin, Berlin, Germany;11Rebirth Center for Translational Regenerative Therapies, Hannover Medical School, Hannover, Germany;12Fraunhofer Institute of Toxicology and Experimental Medicine, Hannover, Germany
Background: Escalating loss of skeletal muscle mass and strength (sarcopenia) is a frequent co-morbidity of heart failure (HF) and often present in the elderly. MicroRNA-22 (miR-22) targets several muscle function-related genes, such as myotubularin-related protein 2, myosin IXA, tropomyosin 3 or sarcalumenin and regulates skeletal muscle differentiation. Our aim was to assess the diagnostic value of miR-22 in sarcopenic HF patients and its association with variables deemed clinically relevant in sarcopenia.
Methods: We assessed miR-22 in 176 chronic HF patients (‘Studies Investigating Comorbidities Aggravating Heart Failure″ SICA-HF; overall prevalence of sarcopenia 15.9%). Sarcopenia was defined as appendicular skeletal muscle mass index <7.26 kg/m2 in males and <5.45 kg/m2 in females. Body composition was assessed by dual-energy X-ray absorptiometry. miR-22 serum concentrations were measured by miR-specific TaqMan RT-qPCR analyses.
Results: In the present study, patients with HF and sarcopenia were older compared to non-sarcopenic HF patients (74.5 [68.7–80.2] vs. 68.4 [60.9–74.8]; P = 0.001), had a lower BMI (25.1 [22.4–26.8] vs. 29.2 [26.0–32.9] kg/m2; P < 0.001), higher NT-proBNP levels (3693.2 [1183.3–5000.0] vs. 1066.4 [521.3–2453.6] pg/mL; P < 0.001), lower left ventricular ejection fraction (16.8 [15.0–20.0] vs. 35.0 [30.0–40.0] %; P = 0.025), lower maximal handgrip strength (31.1 ± 6.0 vs. 37.0 ± 13.0 kg; P = 0.016), lower absolute peak VO2 (1181.3 ± 379.5 vs. 1593.0 ± 487.0 mL/min; P < 0.001) and a lower 6-min walk test distance (389.0 ± 135.5 vs. 466.3 ± 120.0 m; P = 0.009). Cycle threshold (CT) value after RT-qPCR analysis showed that sarcopenic patients with HF had significantly higher serum levels of miR-22 compared to non-sarcopenic patients (5.2 ± 0.8 vs. 5.7 ± 0.9; P = 0.032). In the ROC curve and Youden index analysis the optimal diagnostic cut-off CT-value of miR-22 was 5.39, providing the best trade-off between sensitivity (45.3%) and specificity (85.7%). In the multivariate regression model adjusted for age, diabetes mellitus, ejection fraction, NT-proBNP levels and absolute peak VO2, miR-22 levels (adjusted OR 0.410, 95% CI 0.193–0.868, P = 0.020) and BMI (adjusted OR 0.784, 95% CI 0.642–0.959, P = 0.018) remained associated with presence of sarcopenia in HF patients.
Conclusions: miR-22 is independently associated with sarcopenia in HF patients, proposing a novel epigenetic biomarker of alteration in skeletal muscle.
3-03
Novel biomarkers as possible prognostic tools in the determination of muscle wasting in HF patients
Tania Garfias-Veitl1,2, Sascha Dierks1, Mirela Vatic1,2, Ryosuke Sato1, Guglielmo Fibbi1, Wolfram Doehner3,4,5, Stefan D. Anker3,5,6 and Stephan von Haehling1,2
1Department of Cardiology and Pneumology, University Medical Center Goettingen, Georg-August University, Goettingen, Germany;2German Center for Cardiovascular Research (DZHK), partner site Goettingen, Goettingen, Germany;3Berlin Institute of Health-Center for Regenerative Therapies (BCRT), Charité-Universitätsmedizin Berlin, Berlin, Germany;4Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany;5German Center for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany;6Division of Cardiology and Metabolism - Heart Failure, Cachexia & Sarcopenia, Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany
Background: Muscle wasting is a co-morbidity gaining attention among heart failure (HF) patients and older adults. According to the European Society of Cardiology, its prevalence in HF ranges from 20 to 50%. Identification of sarcopenia in the clinical practice can be challenging, firstly due to its multiple definitions in literature, secondly because of the lack of specific biomarkers that allow early recognition of deterioration of muscle mass. The present study therefore aimed to find possible biomarkers for early screening of muscle wasting.
Methods: Using ProcartaPlex Multiplex Immunoassay (ThermoFisher Scientific, Germany) 43 biomarkers were measured in 169 HF patients from the Studies Investigating Comorbidities Aggravating Heart Failure (SICA-HF). Body composition was assessed by dual energy X-ray absorptiometry. Sarcopenia was defined as a low appendicular lean mass adjusted by height squared (≤7.26 kg/m2 in men, ≤5.5 kg/m2 in women).
Results: Patients with sarcopenia (21.3%) were all male, older (72.35 ± 9 vs. 66.5 ± 11 years, P = 0.006) and presented with lower weight and body mass index (77.31 ± 14 vs. 89.82 ± 16 kg, 24.64 [22.18–26.79] vs. 29.11 [26–32.71] kg/m2; both P < 0.001), had more frequently ischaemic aetiology (77.8 vs. 57.3%, P = 0.025) and higher prevalence of iron deficiency (72 vs. 36%, P < 0.001) and anaemia (44 vs. 23%, P = 0.009) compared to patients without sarcopenia. Estimated glomerular filtration rate (65.61 [48.6–80.6] vs. 71.6 [54.9–82.6] mL/min/1.73 m2, P = 0.226) showed no difference between the groups. In sarcopenic patients concentrations of periostin (41.06 [32.92–47.89] vs. 33.21 [28.39–40.77] pg/mL, P = 0.013), vascular endothelial growth factor-a (VEGF-a) (167.72 [84.89–238.21] vs. 110.36 [60.33–160.44] pg/mL, P = 0.014) and tumour necrosis factor receptor 2 (TNF-R2) (58.93 [44.76–76.56] vs. 48.89 [40–63.86], P = 0.027) were elevated in comparison to non-sarcopenic patients. Previously suggested biomarkers for sarcopenia, namely osteocalcin (18.6 [12.2–22.2] vs. 13.6 [9.83–18] μg/L, P = 0.002), osteoprotegerin (5.88 [4.14–7.64] vs. 4.52 [3.64–6.08] pmol/L, P = 0.016), parathyroid hormone (59.85 [34.5–91.8] vs. 42.1 [32.05–64.35] pg/mL, P = 0.038) and fibroblast growth factor 23 (153.68 [78.74–819.32] vs. 82.9 [56.96–148.72] pg/mL, P = 0.002) were higher in sarcopenic patients. Using univariate logistic regression models, VEGF-a (OR 3.51, 95% CI [1.19–10.31], P = 0.023) and TNF-R2 (OR 1.02, 95% CI [1.002–1.036], P = 0.029) were associated with sarcopenia. In a multivariate logistic regression model, VEGF-a remained an independent predictor of sarcopenia (adjusted OR 4.56, 95% CI [1.03–20.19], P = 0.046).
Conclusions: VEGF-a showed a strong association with sarcopenia in HF patients. It is known that VEGF-a plays a role in angiogenesis but further investigation regarding its relation with muscle deterioration and heart failure is needed.
Count: 390 words.
3-04
Association between bioimpedance phase angle and post-stroke dysphagia: pilot study
Hae-Yeon Park and Seung Yup Song and Geun-Young Park and Sun Im
Department of Rehabilitation Medicine, The Catholic University of Korea Bucheon St. Mary's Hospital, Bucheon, Korea
Introduction: Dysphagia is one of the common sequelae of stroke and can be observed in up to 60–70% of post-stroke patients. Post-stroke dysphagia is associated with various complications including aspiration pneumonia, prolonged length of hospital stay, and increased mortality. Bioimpedance analysis (BIA) is non-invasive tool to evaluate body composition and is commonly used in diagnosing and evaluating sarcopenia. Phase angle is one of the values obtained from BIA, which is useful in evaluating cellular health and known to be related with functional outcome in stroke patients. However, studies on association between phase angle and post-stroke dysphagia is scarce. Therefore, this study aimed to explore the association between phase angle and post-stroke dysphagia severity.
Methods: This study was retrospective observational pilot study, and first-ever stroke patients were included in the study. BIA (In-Body S10; Biospace Co. Ltd., Seoul, South Korea) was performed to measure appendicular skeletal muscle mass (ASM) and phase angle. Post-stroke dysphagia function was evaluated using functional oral intake scale (FOIS) and Korean Mann assessment of swallowing ability (K-MASA).
Results: A total of 34 post-stroke patients were included in the analysis. Sarcopenia accounted for 38.2% (n = 13) of the included participants. Baseline characteristics of the participants are shown in Table 1. In Pearson correlation analysis, phase angle significantly negatively correlated with body mass index, ASM/(height)2, haemoglobin, albumin, and K-MASA (Figure 1).
Conclusions: In this study, phase angle was significantly associated with K-MASA, one of the dysphagia evaluation tool including different aspects of swallowing, including oral motor function, sensation, pharyngeal swallowing, and laryngeal function. Phase angle may be utilized as feasible biomarker that may be associated with post-stroke dysphagia severity. Future studies with larger population are needed to support the result.
3-06
Screening for malnutrition, sarcopenia, and physical frailty in liver transplant recipients: a long-term cross-sectional study
Amal Trigui1,2, Mélanie Tremblay2, Christopher F. Rose1,2 and Chantal Bémeur1,2
Introduction: Despite the relative high survival rate after liver transplant (LT), malnutrition, sarcopenia and frailty are present in 47%, 80% and 59%, respectively, 3 months after surgery. These complications are associated with adverse clinical outcomes and decreased quality of life after LT. However, there are no data regarding malnutrition, sarcopenia, and frailty in the long term after LT. The primary objective is to determine the prevalence of malnutrition, sarcopenia, and frailty at 1, 2 and 3 years after LT. The secondary objectives aim to describe muscle function, quality of life and employment status in LT recipients.
Methods: Cross-sectional observational study is conducted including 65 patients transplanted between 2019 and 2021. A single virtual meeting is performed with each patient during which nutritional risk (Canadian Nutrition Screening Tool), sarcopenia (SARC-F questionnaire), frailty (FRAIL questionnaire), muscle function (chair stand test), quality of life (SF-36) and employment status are assessed.
Results: To date, 64 patients (27 in 2019, 13 in 2020 and 24 in 2021) have completed the study (40 men and 24 women, mean age is 58.8 ± 10.2 years). 12.5%, 15.4% and 11.1% of LT recipients were at risk of malnutrition in the cohort of 1, 2 and 3 years after LT, respectively. In LT recipients, 8.3%, 30.8% and 18.5% were at risk of sarcopenia in the cohort at 1, 2 and 3 years after LT, respectively. In addition, 1 year after LT, 50.0% and 12.5% were prefrail and frail, respectively. At 2 years after LT, 46.2% and 30.8% were prefrail and frail, respectively, whereas, at 3 years after LT, 44.4% and 18.5% were prefrail and frail, respectively. Muscle function was impaired at 1 year after LT (15.8 ± 5.5 s vs. 12.6 s in healthy people) and the score remained unchanged until 3 years after LT. Regarding quality of life, the score of physical heath (62.6% ± 22.1) was slightly below normal and the scores remain unchanged until 3 years after LT. Finally, 68.4% of patients were unemployed, of which 46.2% were in early retirement for a liver disease-related cause.
Conclusions: Up to 3 years after LT, patients are still at risk of malnutrition, sarcopenia, and frailty. The physical component score of their quality of life score is below the score of the general population. The results of this project may help identify appropriate interventions in the long term after LT.
3-08
Sarcopenia is uncommon, despite significant loss of weight and skeletal muscle, in patients undergoing oesophagogastric cancer surgery
Lisa Murnane1,2, Adrienne Forsyth1,3, Audrey Tierney1,4 and Paul Burton5,6
1School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, Australia;2Department of Nutrition and Dietetics, Alfred Health, Melbourne, Australia;3School of Behavioural and Health Sciences, Australian Catholic University, Melbourne, Australia;4School of Allied Health, Health Implementation Science and Technology Centre, Health Research Institute, University of Limerick, Limerick, Ireland;5Department of Surgery, Monash University, Melbourne, Australia;6Oesophagogastric Bariatric Surgery Unit, Alfred Health, Melbourne, Australia
Introduction: Low skeletal muscle is prevalent and associated with poorer outcomes after oesophagogastric (OG) cancer surgery. However, sarcopenia, including strength and function, is less commonly assessed. Therefore, we aimed to describe the prevalence of sarcopenia and changes in diagnostic criteria within 1 year of OG cancer surgery.
Methods: This prospective observational study included patients who had surgical resection of OG cancer between 2018 and 2021 at a tertiary hospital in Melbourne, Australia. Sarcopenia was defined using the EWGSOP2 definition. Body composition assessment using computed tomography (CT) measured skeletal muscle area (cm2) and density (Hounsfield Units, HU). Low skeletal muscle index (SMI) was <52.4 cm2/m2 for males and <38.5 cm2/m2 for females. Low muscle density (myosteatosis) was defined using pre-determined HU and BMI thresholds. Bioimpedance spectroscopy (BIS) quantified muscle as fat-free mass (FFM, kg). Low fat-free mass index (FFMI) was <17 kg/m2 for males and <15 kg/m2 for females. Hand grip strength (HGS, kg) and 6-metre walk test (m/s) measured strength and function. Sarcopenia was assessed preoperatively and up to 1-year postoperatively using CT (Sarc-CT) and BIS (Sarc-BIS) muscle measurements. Weight (kg) was recorded at each time point.
Results: Fifty patients, predominantly male (62%) and mean age of 64 years, were included preoperatively, with 32 patients at 1 year. The prevalence of Sarc-CT was 7.1% preoperatively and 10.7% at 1 year (P = 0.32), with a significant reduction in SMI (47.2 vs. 44.16 cm2/m2, P = 0.03) between time points. Low SMI (46%) and myosteatosis (50%) were prevalent preoperatively and remained unchanged at 1 year (both P = 0.21). The prevalence of Sarc-BIS was 2% preoperatively and 3.3% at 1 year (P = 0.60). Figure 1 shows changes in weight and FFM. Low FFMI occurred in 8% preoperatively and 12% at 1 year (P = 1.00). Few patients met the low HGS (16%) and low walk speed (8%) criteria preoperatively without significant postoperative changes (both P = 0.50).
Conclusions: Despite the high preoperative prevalence of low SMI and myosteatosis and the significant loss of weight and skeletal muscle after surgery, sarcopenia was uncommon. The low prevalence of sarcopenia is predominantly attributable to the high number of patients with HGS above the low strength threshold. These results indicate that loss of skeletal muscle, without corresponding decline in strength or function, is a prominent feature in this patient cohort. Considering the known negative impact of low skeletal muscle on surgical complications and survival, muscle assessment remains a valuable and clinically meaningful measure.
3-11
Sarcopenic obesity is predictive of critical weight loss in patients with head and neck cancer
Belinda Vangelov1, Robert Smee1,2,3 and Judith Bauer4
1Department of Radiation Oncology, Nelune Comprehensive Cancer Centre, Prince of Wales Hospital, Sydney, Australia;2School of Clinical Medicine, Randwick Campus, Faculty of Medicine and Health, University of New South Wales, Sydney, Australia;3Department of Radiation Oncology, Tamworth Base Hospital, Tamworth, Australia;4Department of Nutrition, Dietetics and Food, School of Clinical Sciences, Monash University, Melbourne, Australia
Introduction: Patients with head and neck cancer (HNC) are at high risk of malnutrition and critical weight loss (CWL), either as a result of the tumour, and/or toxicities of treatment modalities. Evaluation of skeletal muscle (SM) loss via computed tomography (CT) (CT-defined sarcopenia), has become an important nutrition assessment tool. We investigated predictors of CWL during radiotherapy (RT) and the impact of sarcopenia on overall survival (OS).
Methods: This retrospective study included adult patients with newly diagnosed HNC who completed radiotherapy (RT) (± other modalities) in our facility. SM was measured using PET-CT scans or RT planning CT scans at the third lumbar vertebra (L3) where available, and at the third cervical (C3) and second thoracic (T2) vertebra in patients with no visible L3 landmark. Validated equations were applied to C3 and T2 SM cross-sectional area (CSA) to predict L3-CSA. SM index (SMI, cm2/m2) was applied to determine sarcopenia, stratified by sex and body mass index (BMI). Predictors of CWL (≥5% during RT) were determined, and the impact of sarcopenia on OS was investigated with Kaplan Meier analysis.
Results: Scans of 415 patients were analysed (majority male 84%, mean age 60 years). Oropharynx cancer was the most prevalent (52%), with concurrent chemoRT used to treat 47% of patients. Sarcopenia was present in 43% (n = 177), with 61% (n = 116) also being overweight or obese (BMI ≥ 25 kg/m2). CWL was experienced by 58% (n = 239), and 29% of these patients also had sarcopenic obesity at baseline. Patients with sarcopenic obesity were found to be 4.2 times more likely to experience CWL (OR 4.16, 95% CI 1.84–9.42, P = 0.001). Other predictors on multivariate analysis were: concurrent chemoRT (OR 4.9, 95% CI 2.65–9.08, P < 0.001), oropharynx tumour (OR 2.8, 95% CI 1.46–5.39, P = 0.002), nasopharynx tumour (OR 3.6, 95% CI 1.32–9.97, P = 0.012) and females (OR 2.17, 95% CI 1.05–4.49, P = 0.037). Patients without sarcopenia at presentation were less likely to have CWL when not categorized by BMI (OR 3.9, 95% CI 1.76–8.62, P = 0.001). Neither sarcopenic obesity or CWL significantly impacted on OS, however, sarcopenia without BMI categorisation was associated with worse OS (Log Rank P = 0.006), median survival 8.4 versus 10.1 years (95% CI 4.00–12.00).
Conclusions: Patients with HNC who are overweight or obese are at risk of CWL during RT, and evaluation of SM prior to treatment may assist in early identification and appropriate nutrition intervention planning.
3-12
Body composition phenotype sarcopenic obesity is associated with poor physical fitness assessed by cardiopulmonary exercise testing in patients undergoing colorectal cancer surgery
Jason Rai1, Edward T. Pring1, Katrina Knight2, Henry Tilney3, Fiona Taylor4, Laura E. Gould1, Dinh V.C. Mai1, Ioanna Drami1, Campbell Roxburgh2 and John T. Jenkins1
1BiCyCLE Research Group, St Mark's Academic Institute, St Mark's Hospital, Harrow, UK;2University of Glasgow School of Medicine Dentistry and Nursing, Glasgow, UK;3Frimley Health NHS Foundation Trust, Frimley Park Hospital, Frimley, UK;4Barts Health NHS Trust, Whipps Cross University Hospital, London, UK
Introduction: Preoperative risk assessment for major colorectal cancer (CRC) surgery remains a challenge. Body composition (BC) analysis and objective physical fitness assessment can be used to evaluate risk. We aim to investigate if BC is associated with poor performance on cardiopulmonary exercise test (CPET) in CRC patients.
Methods: Stage I-III CRC patients undergoing CPET were identified between 2010 and 2020. BC analysis was done using a single axial slice preoperative CT image at third lumbar vertebra.
Sarcopenia was defined according to BMI < 25 skeletal muscle index (SKMi) < 43 cm2/m2 in men, <41 cm2/m2 in female, while BMI ≥ 25 SKMi <53 cm2/m2 in men and <41 cm2/m2 in female. Sarcopenic obesity was defined as having sarcopenia and BMI > 30. Myosteatosis was defined as skeletal muscle mean attenuation in Hounsfield unit <41 in men and <33 in female. Visceral obesity was defined as visceral fat area >164 cm2 in men and >80 cm2 in female. CPET variables were oxygen uptake at anaerobic threshold (AT) < 11.1 mL/kg/min and peak oxygen uptake (peak VO2) < 18.2 mL/kg/min.
Relationships between clinicopathological, BC and CPET variables were investigated using binary logistic regression. Variables with a P-value <0.05 on univariate analysis were entered into the multivariate model.
Results: 218 CRC patients were identified from two different UK hospitals. On univariate analysis gender (0.32, 95% CI 0.18–0.59, P < 0.001), ASA (3.52, 95% CI 1.90–6.52, P < 0.001) and TNM (2.12, 95% CI 1.19–3.79, p 0.011) were associated with reduced AT. On multivariate analysis gender, ASA and TNM were independently associated with reduced AT.
On univariate analysis age (3.22, 95% CI 1.83–5.69, P < 0.001), gender (0.32, 95% CI 0.18–0.59, P < 0.001), ASA (3.08, 95% CI, 1.66–5.70, P < 0.001), TNM (3.64, 95% CI 2.06–6.42, P < 0.001), myosteatosis (2.28, 95% CI 1.28–4.05, p 0.005) and sarcopenic obesity (2.48, 95% CI 1.18–5.24, p 0.017) were associated with reduced peak VO2. On multivariate analysis age, gender, ASA, TNM and sarcopenic obesity were independently associated with reduced peak VO2.
Conclusions: We present novel finding that sarcopenic obesity is associated with poor physical fitness when objectively assessed with CPET in CRC patients.
3-14
Sexual dimorphism in masseter thickness as anthropometric prognostic biomarker in head & neck cancer cachexia: a retrospective cross-sectional study
Julián Balanta-Melo1,2, Alexander J. Jones3, Michael G. Moore3 and Andrea Bonetto4
1Department of Anatomy, Cell Biology & Physiology, Indiana University School of Medicine, Indianapolis, IN, USA;2Department of Otolaryngology – Head & Neck Surgery, Indiana University School of Medicine, Indianapolis, IN, USA;3Universidad del Valle School of Dentistry, Cali, Colombia;4Department of Pathology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Introduction: Cancer cachexia (CA-CX) is characterized by progressive loss of skeletal muscle, with or without loss of fat, that cannot be reversed by nutritional support. Criteria for CA-CX include either one or a combination of: weight loss >5% (last 6 months; no starvation), Body Mass Index (BMI) < 20 + weight loss >2% and appendicular skeletal muscle index (ASMI) indicating sarcopenia + weight loss >2%. ASMI is generally obtained from computerized tomography (CT). However, full body CT is rarely available in head & neck cancer (HNC) patients. Here we analyse the masseter muscle thickness as an alternative method to discriminate between HNC-cachexia and non-cachexia (NCX) in adult males and females.
Methods: 60 HNC CT datasets (DICOM) from sex-, race-, height- and age-matched white males and females were analysed. For three-group comparison, per sex, patients fulfilling all three criteria for CA-CX (CA-CX; n = 10) and patients with cancer but no CX (CA-NCX; n = 10) were analysed relative to no cancer, non-cachectic, healthy control patients (CTRL; n = 10). For two-group comparison we included: CA-CX and NCX (CA-NCX + CTRL) groups. Left masseter muscle was segmented with a 3D-imaging software. 3D distribution of masseter thickness (MT), body weight, and BMI were quantified. Area under the curve (AUC) of the receiver operating characteristics (ROC) analysis was calculated. All statistical analyses were blinded. Male and female cohorts were analysed separately.
Results: For both males and females, CA-CX subjects exhibited reduced body weight and BMI. Only in the male cohort, CA-CX MT was significantly reduced (95% CI: 2.33–3.38) relative to both CTRL (95% CI: 3.19–4.42) and NCX (95% CI: 3.33–4.06). When CA-CX relative to NCX, AUC-ROC (males, 0.88, 95% CI: 0.70–1.0; females, 0.74, 95% CI: 0.55–0.93) was significant (P < 0.05), with sensitivity (males, 66.7%, 95% CI: 30.0–94.1; females, 50.0%, 95% CI: 23.7–76.3), specificity (males, 90.0%; 95% CI: 59.6–99.5; females, 90.0%, 95% CI: 69.9–98.2) and likelihood ratio (males, 13.3; females, 5.0), at a MT cut-off <9.68 (males) and <8.80 (females).
Conclusions: MT showed a sexual dimorphism as an anthropometric prognostic biomarker to discriminate between CA-CX and NCX in HNC patients and represents a promising tool that will need validation in larger cohort studies including other ethnicities, both sexes and different age groups.
3-17
Height-adjusted appendicular skeletal muscle mass is overestimated due to height loss in Japanese middle-aged and older women: the Japanese Population-based Osteoporosis (JPOS) study
Kazuki Kaji1, Jun Kitagawa2, Takahiro Tachiki3, Kouji Tsuda4, Masayuki Iki5, Junko Tamaki4, Katsuyasu Kouda6, Naonobu Takahira2, Etsuko Kajita7 and JPOS Study Group4
1Kitasato University Kitasato Institute Hospital, Tokyo, Japan;2Kitasato University, Tokyo, Japan;3University of Kochi, Kochi, Japan;4Osaka Medical and Pharmaceutical University, Osaka, Japan;5Kindai University, Osaka, Japan;6Kansai Medical University, Osaka, Japan;7Chukyo Gakuin University, Gifu, Japan
Introduction: Both EWGSOP 2 and AWGS 2019 use height-adjusted appendicular skeletal muscle mass (ASM/ht2) as a cut-off value for a definitive diagnosis of sarcopenia. However, the 2020 US Sarcopenia Definitions and Outcomes Consortium dispenses with ASM entirely, either absolute or after adjusting for body size, because there are no clear associations between ASM and adverse health-related outcomes.
We focused on age-related height loss (HL) that might cause overestimation of ASM/ht2, attenuating the predictive value for poor clinical outcomes in the elderly.
The purpose of this study was to examine the effects of HL over the past 15 years on the absolute level of ASM and indices adjusted for body size in different ways, using height squared (ASM/ht2), weight (ASM/weight), and body mass index (ASM/BMI) in Japanese middle-aged and older women.
Methods: This study was part of the 15/16-year follow-up survey of the Japanese Population-based Osteoporosis (JPOS) cohort study conducted in 2011/2012. The JPOS cohort study was started in 1996. The subjects of the 15/16-year follow-up were 762 women (mean: 67.4 years). Subjects were divided into quartiles by HL over the past 15 years (Q1 was the lowest; Q4 was the highest). ASM was measured by dual X-ray absorptiometry, and we calculated ASM/ht2, ASM/weight, and ASM/BMI. Grip strength (kg) was measured as an indicator of muscle strength. Trend tests were used to examine the difference among quartiles of HL.
Results: The mean HL value over the past 15 years in all subjects was 1.95 cm. A trend test showed a significant increase in mean age from the lowest to highest quartile. While ASM and ASM/BMI were significantly decreased from Q1 to Q4, ASM/ht2 was significantly increased from Q1 to Q4. There was no significant difference in ASM/weight among quantiles. Grip strength was significantly decreased from Q1 to Q4.
We compared differences among quartiles in each index of ASM after adjusting for age. There were no significant differences in ASM and ASM/weight among groups. ASM/ht2 and ASM/BMI retained significant differences after adjusting for age.
These results indicate that middle-aged and older women who exhibit a greater HL show higher ASM/ht2 along with low muscle strength.
Conclusions: This study suggests that ASM/ht2 is overestimated due to HL in Japanese middle-aged and older women.
3-18
Functional physical parameters are more associated with falls than with the diagnosis of sarcopenia by EWGSOP2
Renata Gonçalves Pinheiro Correa1, Anna Raquel Silveira Gomes2 and Victoria Zeghbi Cochenski Borba3
1Federal University of Paraná, Curitiba, Paraná, Brazil;2Prevention and Rehabilitation in Physical Therapy Department, Federal University of Paraná, Curitiba, Paraná, Brazil;3Internal Medicine Department, Endocrine Division (SEMPR), Federal University of Paraná, Curitiba, Paraná, Brazil
Introduction: Aging are associated with osteoporosis and progressive loss of muscle mass and quality. The risk of falls is especially troublesome in women with osteoporosis.
Objectives: to evaluate the presence of sarcopenia and the relationship of its components with the history of falls and fractures.
Methods: Cross-sectional study with women aged ≥65 years recruited during their visit to the osteoporosis clinic or from the community. Those with unstable chronic diseases or under medications, except treatment for osteoporosis, that could interfere with the assessment were excluded. The included participants answered a questionnaire (demographics, diseases characteristics, lifestyle and history of falls and fractures), performed functional and isometric strength tests including ankle evaluation (peak isometric strength (PIS), muscle architecture and muscle thickness [MT]. Muscle architecture was evaluated by ultrasound and the DXA exam (lumbar spine, femur, total body) was performed. Sarcopenia was diagnosed based on EWGSOP2. Participants were divided in sarcopenia group (SG) and non-sarcopenia group (NSG).
Results: Out of 340 screened, 116 were included (71.54 ± 3.19 years, body mass index 26.10 ± 3.66 kg/m2). Although 50% of individuals had low performance or strength, only 6.89% was diagnosed with sarcopenia (SG: 8; NSG: 108) following the EWGSOP2 criteria. Bone mineral density on all sites was lower in SG versus NSG, P < 0.005 for all. The most affected performance test was the gait speed (GS) - 32.78% followed by the short physical battery test (23.27%). The seat to stand test was low in 46.55% of the individuals, while the hand grip strength was low only in 11.2%. All individuals had compromised ankle function. Surprisingly, more subjects had low calf circumference compared to appendicular lean mass index (ALMI) 20.3% versus 13.7%, respectively, limiting sarcopenia diagnosis. Previous falls were negatively correlated with dorsiflexor range of motion (ROM) (R = −0.212, P = 0.017) and PIS (R = −0.212, P = 0.023). The PIS was related to the number of falls (R = - 0.194, P = 0.049) and fractures (R = −0.219, P = 0.019). Similarly, the plantiflexion ROM correlated negatively with GS (R = −0.182, P = 0.047) and ALMI (R = −0.256, P = 0.005).
Conclusions: sarcopenia prevalence was low despite the high percentage of functional impairments; possibly the EWGSOP2 criteria may be underdiagnosing sarcopenia in Brazilian elderly women. Functional assessments, including ankle function, should be incorporated into the evaluation of sarcopenia and falls.
3-19
Validation of accuracy and reliability of automated segmentation of body composition from single-slice CT images at L3 level using data analysis facilitation suite (DAFS) in patients with non-metastatic colorectal cancer
Mushfiqus Salehin1, Vincent Tze Yang Chow2, Parsa Moheban3, Hyunwoo Lee4, Bette J. Caan5, Elizabeth M. Cespedes Feliciano5, Da Ma6, Mirza Faisal Beg2 and Karteek Popuri1
1Department of Computer Science, Faculty of Science, Memorial University of Newfoundland, St. John's, Canada;2School of Engineering, Simon Fraser University, Vancouver, Canada;3Department of Biomedical Engineering, University of British Columbia, Vancouver, Canada;4Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, Canada;5Division of Research, Kaiser Permanente Northern California, Oakland, CA, USA;6Department of Internal Medicine Section of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA
Introduction: Assessing body composition using computed tomography (CT) can help predict clinical outcomes of cancer patients as it can be related to surgical complications, chemotherapy toxicity, and survival. However, manual segmentation of whole-body CT images is labour-intensive and requires expertise in body anatomy and composition, which may lead to a significant amount of inter-observer variability. To overcome this limitation, automated methods such as the Data Analysis Facilitation Suite (DAFS) software have been developed to segment body tissues in 3D CT scans. In this study, we validate the accuracy and reliability of DAFS in segmenting body composition from single-slice CT images.
Methods: The study analysed single-slice CT images at the third lumbar vertebra (L3) level of patients with non-metastatic colorectal diagnosis at Kaiser Permanente. The cohort for analysis consists of CT images taken from 9067 subjects. Segmentation of skeletal muscle mass (SKM), visceral adipose tissue (VAT), and subcutaneous adipose tissue (SAT) at L3 were performed both manually and automatically using DAFS. Areas were calculated for these three tissue types. The accuracy of DAFS vis-a-vis manual segmentation was assessed by the Dice index, reliability was assessed by intra-class correlation coefficients, and agreement between automatic and manual segmentations was assessed by Bland–Altman analysis.
Results: The accuracy of automatic segmentation compared to manual analysis was high for all three tissue types, as indicated by the Dice scores and intra-class correlation coefficients (Table 1). The Bland–Altman plots (Figure 1) indicated that automated measurements tended to underestimate the tissue areas compared to the manual analysis for all three tissue types, with mean differences (±2 standard deviations) of −5.87 (4.68, −16.43) cm2, −5.45 (4.85, −15.75) cm2, and −6.30 (7.58, −20.18) cm2, respectively.
Conclusions: The study validates that automated L3 segmentation using the DAFS platform is an accurate, reliable, and efficient method for measuring body composition that closely matches the manual segmentation in patients with non-metastatic colorectal cancer. This may help overcome the bottleneck of manual training and effort needed to measure body composition and may serve as a useful tool in assessing markers of sarcopenia, muscle loss, and adiposity, as well as in predicting clinical outcomes.
3-20
Deep learning-driven volumetric CT body composition analysis: new metrics for long-term postoperative risk stratification in colorectal cancer patients
Dinh V.C. Mai1,2, Ioanna Drami1,2, Edward T. Pring1,2, Laura E. Gould1,2, Jason Rai1, Philip Lung1,2, Vincent Chow3, Karteek Popuri4, Mirza Beg3, Thanos Athanasiou2 and John T. Jenkins1,2
1St Mark's Academic Institute, St Mark's Hospital, Harrow, UK;2Department of Surgery and Cancer, Imperial College London, London, UK;3Department of Computer Science, Memorial University of Newfoundland, St John's, Canada;4School of Engineering Science, Simon Fraser University, Burnaby, Canada
Background: A 2D single L3 CT slice has been de facto for studying body composition (BC) in cancer, with sarcopenia and myosteatosis predicting poorer short and long-term colorectal cancer (CRC) outcomes. Relationships with adipose tissue is less clear. The Data Analysis Facility Suite (DAFS) is a deep learning software enabling volumetric BC assessment from 3D regional CT scans. DAFS was used to study relationships between volumetric BC and CRC overall (OS) and disease-free survival (DFS) outcomes.
Method: Patients were sourced from a database of curative surgical resections for primary and non-complex CRC at a UK tertiary centre between 2006 and 2013. DAFS segmented preoperative CT scans, providing abdominopelvic volumes of skeletal muscle (SM), subcutaneous, visceral, and total adipose tissue (SAT, VAT, TAT). This was defined from superior-most L1 to inferior-most coccyx. Division by abdominopelvic length and patient height2 provided an abdominopelvic index (Figure 1). Tissue radiodensity was quantified by mean Hounsfield attenuation (MA). Continuous metrics were categorized by quartiles, whilst additional literature cut-offs were applied to SM index. Multivariate Cox regression analysed relationships between BC and outcomes. Intravenous contrast use was included as a co-variate.
Results: At 60 months, 219 of 750 patients had died (29.2%). Reduced OS was predicted by sarcopenia (HR = 1.309, CI 95% 1.027–1.668, P = 0.029), the lowest quartile of TAT index (HR = 1.466, CI 95% 1.1132–1.898, P = 0.004), and myosteatosis (HR = 1.334 CI 95% 1.025–1.736, P = 0.032). The highest quartile of mean SAT (HR = 1.390, 95% CI 1.065–1.814, P = 0.015) or VAT MA (1.402, 95% CI 1.077–1.826, P = 0.012) also had an elevated risk. Patients with simultaneous sarcopenia and low TAT index had a particularly heightened mortality: a 48% 5-year rate (HR = 1.650, CI 95% 1.194–2.279, P = 0.002). Excluding metastatic disease, 125 of 659 (18.9%) suffered recurrences. Reduced DFS was independently associated with sarcopenia (HR 1.706, 1, 1.005–2.896, P = 0.048) and the highest quartile of VAT MA (HR 1.576, 1.060–2.344, P = 0.025).
Conclusions: Increased VAT MA could be a novel predictor of CRC mortality and recurrence. Additionally, low TAT quantity is associated with mortality, particularly in combination with sarcopenia. Further research is required to validate concordance of regional CT scan BC with true whole body, allowing for standardized methodology in future volumetric BC studies.
3-21
Automated volumetric BC quantification by the data analysis facility suite (DAFS): external validation for preoperative CT abdomen and pelvis in colorectal cancer
Dinh V.C. Mai1,2, Jason Rai1, Ioanna Drami1,2, Edward T. Pring1,2, Laura E. Gould1,2, Philip Lung1,2, Vincent Chow3, Karteek Popuri4, Mirza Beg3, Thanos Athanasiou2 and John T. Jenkins1,2
1St Mark's Academic Institute, St Mark's Hospital, Harrow, UK;2Department of Surgery and Cancer, Imperial College London, London, UK;3Department of Computer Science, Memorial University of Newfoundland, St. John's, Canada;4School of Engineering Science, Simon Fraser University, Burnaby, Canada
Introduction: The Data Analysis Facility Suite (DAFS) is a deep learning-driven software capable of automated segmentation of 3D clinical CT scans. This is relevant to researchers and clinicians interested in body composition (BC) as volumetric measures of skeletal muscle (SM) and subcutaneous, visceral and intermuscular adipose tissue (SAT, VAT, IMAT) are provided. This is the first external validation of DAFS' performance in quantifying of SM, SAT, VAT and IMAT.
Method: The validation test was conducted in a UK tertiary hospital, where 13 male and 13 female patients were randomly selected from a colorectal cancer database. The 26 CT abdomen and pelvis scans were segmented by DAFS. We calibrated DAFS to focus on the abdominopelvic region, defined from the superior-most aspect of the L1 vertebra to the inferior coccyx. Abdominopelvic volumes of SM, SAT, VAT, and IMAT were then produced without manual verification.
The segmentation files were then duplicated. Two clinicians checked through the automated segmentation for errors using the inbuilt manual annotation and segmentation tool. After corrections were made and saved, tissue volumes were reproduced for each clinician. Clinician interobserver agreement was assessed. Mean volumes of SM, SAT, VAT, and IMAT volumes between the two clinicians were calculated and compared to DAFS' initial unverified measurements by Bland–Altman plots. Volume percentage differences with 95% C. I limits of agreement (LoA) were also calculated.
Results: The Bland–Altman plots for clinician versus clinician and clinician versus DAFS interobserver agreements are shown in Figures 1 and 2. There was strong clinician versus clinician agreement for SM, SAT, VAT and IMAT volumes, with mean percentage differences of 0.06 ± 1.61%, 0.09% ± 1.18%), 0.13 ± 1.15%), and 0.06 ± 1.39%, respectively.
Mean volumes of each tissue were then derived the two sets of clinician-verified measurements and compared to the unverified DAFS measurements. Mean percentage differences were 0.09 ± 0.6%, 0.07 ± 1.23%, 0.03 ± 1.07%, and 0.03 ± 1.39% for SM, SAT, VAT, and IMAT, respectively.
Conclusions: There was high agreement between unverified and clinician-verified DAFS measurements of SM, SAT, VAT, and IMAT volumes from the abdominopelvic CT scans in this single UK colorectal cancer hospital. We recommend this as a convenient methodology for external validation of DAFS in other in other institutions.
3-22
Compared to single lumbar slice, volumetric body composition analysis from regional CT scans is more representative of skeletal muscle and adipose tissue volume and radiodensity
Dinh V.C. Mai1,2, Ioanna Drami1,2, Edward T. Pring1,2, Laura E. Gould1,2, Jason Rai1, Philip Lung1,2, Vincent Chow3, Karteek Popuri4, Mirza Beg3, Thanos Athanasiou2 and John T. Jenkins1,2
1St Mark's Academic Institute, St Mark's Hospital, Harrow, UK;2Department of Surgery and Cancer, Imperial College London, London, UK;3Department of Computer Science, Memorial University of Newfoundland, St. John's, Canada;4School of Engineering Science, Simon Fraser University, Burnaby, Canada
Background: Body composition (BC) in the context of colorectal cancer (CRC) outcomes is a keen area of research. Using a single third lumbar (L3) CT slice has been a surrogate estimate of whole skeletal muscle (SM), subcutaneous and visceral adipose tissue (SAT, VAT) quantity. The Data Analysis Facility Suite (DAFS) is a deep learning software allowing 3D BC analysis of entire scans. Our group utilized DAFS to examine relationships between thoracic BC and outcomes in patients undergoing surgery for complex and recurrent CRC. We also assessed relationships between 2D SM, VAT and SAT L3 surface areas, with 3D volumes thoracic and abdominopelvic volumes on CT.
Methods: A 2009–2019 complex CRC database at St Mark's Hospital was reviewed. DAFS segmented preoperative CT thorax/abdomen/pelvis according to BC tissues. Segmentations were checked by a clinician. SM, SAT and VAT were quantified as three-dimensional thoracic (T2 to T11) and abdominopelvic (L1 to coccyx) volumes, and as surface areas at the mid-L3 level. Tissue radiodensity was measured by mean Hounsfield attenuation (MA) per 3D or 2D region.
Results: In 186 patients, thoracic and abdominopelvic volumetric BC strongly correlated (r = 0.905, 0.929, 0.845, all P < 0.001, for SM, SAT and VAT, respectively). Comparatively, L3 surface areas correlated weakly with thoracic SM (r = 0.187, P = 0.02), SAT (r = 0.200, P = 0.013), and VAT (r = 0.237, P = 0.003) volumes, and with abdominopelvic volumes (SM, r = 0.188, P = 0.014; SAT, r = 0.251, P = 0.001; VAT, r = 0.178, P = 0.020). Whilst both abdominopelvic volumes and L3 surface area predicted thoracic BC, the abdominopelvic volume linear regression model had markedly stronger fit (SM R2 = 0.820 vs. 0.032; SAT R2 = 0.830 vs. 0.060; VAT R2 = 0.706 vs. 0.033).
3D L1-coccyx tissue MA were compared with 2D L3 surface area. Weak correlation existed for SM (r = 0.276, P < 0.001) and VAT (r = 0.156, P = 0.041), and no relationship was observed for SAT (r = 0.059, P = 0.439). On comparing 3D thoracic and abdominopelvic regions, there was strong correlation for SM (r = 0.892, P < 0.001) and SAT (r = 0.875, P < 0.001), and moderate relationship for VAT (r = 0.676, P = 0.041) MA.
Conclusions: Volumetric BC from regional CT scans could be more representative of SM and AT volume and radiodensity.
3-23
Elevated epicardial adipose tissue and aortic calcification, quantified from volumetric regional CT scans, are associated with postoperative complications in complex rectal cancer
Dinh V.C. Mai1,2, Ioanna Drami1,2, Edward T. Pring1,2, Laura E. Gould1,2, Jason Rai1, Philip Lung1,2, Vincent Chow3, Karteek Popuri4, Mirza Beg3, Thanos Athanasiou2 and John T. Jenkins1,2
1St Mark's Academic Institute, St Mark's Hospital, Harrow, UK;2Department of Surgery and Cancer, Imperial College London, London, UK;3Department of Computer Science, Memorial University of Newfoundland, St. John's, Canada;4School of Engineering Science, Simon Fraser University, Burnaby, Canada
Introduction: Body composition (BC) research in colorectal cancer commonly focuses on measurements from the abdominal cavity. The Data Analysis Facility Suite (DAFS) is a deep learning-driven software platform capable of automated body composition analysis of three-dimensional (3D) regional CT scans. We used DAFS to study assessed relationships between volumetric thoracic BC and early postoperative outcomes in a cohort of patients undergoing surgery for complex rectal cancers (RC) at St Mark's Hospital.
Method: A database of resections of locally advanced or recurrent RC from 2009–2022 was reviewed. Available CT thorax scans were automatically segmented DAFS and visually checked by a clinician. Skeletal muscle (SM), aortic calcification (AC), thoracic and epicardial adipose tissue (ThAT, EpiAT) volumes were quantified from a 3D slab (a 3D region of multiple CT slices) between T2 and T11. Volumes were divided by slab length and patient height2, excluding AOC which was divided by thoracic aortic volume. Each tissue index was divided into sex-specific tertiles for comparison.
Results: In 206 patients, postoperative cardiovascular events were significantly increased in the highest tertile of ThAT (11.8% vs. 1.4% P = 0.036), and EpiAT index (11.8% vs. 1.4% P = 0.36). Major wound complications were increased in the highest tertile of EpiAT (35.3% vs. 16.7% P = 0.032). Moderate correlation was observed between ThAT and EpiAT indexes (r = 0.769, P < 0.001).
Patients in the highest tertile of AOC were significantly likelier to suffer postoperative cerebrovascular events (14.7% vs. 0%, P = 0.01), and anastomotic leakage (8.8% vs. 0%, P = 0.11). Individuals in the highest tertile of SM index benefited from reduced rates of pelvic collection (8.8% vs. 27.8, P = 0.027), or any collection requiring radiological drainage (2.9% vs. 18.1%, P = 0.034).
Conclusions: ThAT, EpiAT and AC could be novel predictors of cardiovascular, cerebrovascular and anastomotic complications after complex RC surgery. In the context of abdominal pathology, thoracic BC should be additionally studied now that technology allows for analysis of 3D regional CT. EpiAT would be missed if focusing on the abdomen alone. Further study with a larger sample is required, allowing for multivariate logistic regression to confirm whether these observations are independent.
3-24
Evaluation of body composition at L3 from computed tomography (CT) images using DAFS software, a 3D fully automated multi-slice multi-organ extraction platform
Michelle V. Dietz1, Karteek Popuri2, Lars Janssen1, Mushfiqus Salehin3, Da Ma2,5, Vincent Tze Yang Chow2, Hyunwoo Lee4, Cornelis Verhoef1, Eva V.E. Madsen1, Mirza Faisal Beg2 and Jeroen L.A. van Vugt5
1Department of Surgical Oncology, Erasmus MC Cancer Institute, Rotterdam, The Netherlands;2School of Engineering, Simon Fraser University, Vancouver, Canada;3Department of Computer Science, Faculty of Science, Memorial University of Newfoundland, St. John's, Canada;4Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, Canada;5Department of Internal Medicine Section of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA
Introduction: Measures of body composition can be used to evaluate the nutritional status of patients, which may affect the clinical outcomes. To facilitate accurate and time-efficient body composition measurements, fully automated whole-body 3D computed tomography (CT) segmentation methods have been developed. The aim of the current study was to evaluate the performance of automated segmentation by the Data Analysis Facilitation Suite (DAFS) in an independent dataset.
Methods: The current study used preoperative CT scans of patients who had undergone cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal peritoneal metastases or pseudomyxoma peritonei from appendicular origin (n = 165) from March 2014 to May 2019 at the Erasmus MC Cancer Institute, Rotterdam, Netherlands. Manual and automated measurements of skeletal muscle mass (SMM), visceral adipose tissue (VAT), subcutaneous adipose tissue (SAT), and intramuscular adipose tissue (IMAT) were performed at the third lumbar vertebra (L3). Segmentation accuracies of the automated measurements were evaluated based on their Jaccard index and intra-class correlation coefficients with the manual measurements.
Results: Median age was 64 years (IQR 55–71) and 50.3% of the patients were men. Automatic segmentation provided accurate measurements compared to manual analysis, as indicated by Jaccard scores coefficients of 97.9 for SMM, 98.4 for VAT, 99.1 for SAT, and 79.4 for IMAT. In accordance, intra-class correlation coefficients ranged from 0.98 to 1.00. The Bland–Altman plots (Figure 1) showed that automated measurements on average overestimated SMM and SAT areas compared to manual analysis, with mean differences (±2 standard deviations) of 1.10 cm2 (−1.91, 4.11) and 1.61 cm2 (−2.26, 5.48), respectively. For VAT and IMAT, automated measurements on average underestimated the areas with mean differences of −1.24 cm2 (−3.35, 0.87) and −0.93 cm2 (−5.20, 3.35), respectively.
Conclusions: The current study showed that the commercially available DAFS software provides similar results compared to manual measurements of body composition at the level of L3. This software provides accurate and time-efficient body composition measurements, both of which are necessary for implementation in clinical practice. Cervical and thoracic measurements will be added shortly.
3-25
Mosamatic: a user-friendly, web browser-based platform for automatic analysis of body composition using CT scans
Ralph Brecheisen1, David P.J. van Dijk1, Sander S. Rensen1, Leonard Wee1,2, Andre Dekker2 and Steven W.M. Olde Damink1
1Department of Surgery, Maastricht University, Maastricht, The Netherlands;2Department of Radiotherapy (MAASTRO) School of Oncology and Reproduction, Maastricht University, Maastricht, The Netherlands
Background: Body composition assessment using abdominal computed tomography (CT) images is increasingly applied in clinical and translational research for assessing cachexia, sarcopenia, mortality risk, etc. Manual segmentation of body compartments on L3 CT images is time-consuming and requires significant expertise. Robust high-throughput automated segmentation is key to assessing large patient cohorts and, ultimately, to support implementation of body composition measures into routine clinical practice.
Methods: We trained a deep learning neural network (DLNN) on several clinical cohorts of various cancer types (>3400 patients) with expert-annotated ground truth images and performed external validation on another large independent cohort from a single centre (>2500 patients).
Results: Mosamatic was implemented in Python 3.9 and uses packages like Django, pydicom, TensorFlow, NumPy, Pandas, Redis and Django RQ. The application is wrapped inside a Docker container for easy deployment on any platform. The web interface of Mosamatic is shown in Figure 1. The website for submitting requests to have your L3 CT images analysed by us is www.mosamatic.com. Note this is not the URL of the web application.
Conclusions: Mosamatic makes body composition analysis faster and more easily available. This will enable faster future implementation in clinical settings. We believe that body composition can have a major impact on treatment decisions in oncology applications. We encourage clinical researchers in the field to contact us and try out Mosamatic. For academic purposes the tool will be free of charge.
3-26
Using MRI to measure head muscles: an innovative method for opportunistically determine muscle mass and detect sarcopenia
Miguel German Borda1,2,3, Gustavo Duque4,5, Mario Ulises Pérez-Zepeda6,7, Jonathan Patricio Baldera1,8, Eric Westman9, Anna Zettergren10, Jessica Samuelsson10, Silke Kern10,11, Lina Rydén10, Ingmar Skoog10,11 and Dag Aarsland1,12
1Centre for Age-Related Medicine (SESAM), Stavanger University Hospital, Stavanger, Norway;2Semillero de Neurociencias y Envejecimiento, Aging Institute, Medical School, Pontificia Universidad Javeriana, Bogota ́, Colombia;3Faculty of Health Sciences, University of Stavanger, Stavanger, Norway;4Research Institute of the McGill University Health Centre, Montreal, Canada;5Dr. Joseph Kaufmann Chair in Geriatric Medicine, Department of Medicine, McGill University, Montreal, Canada;6Instituto Nacional de Geriatría, Mexico DF, Mexico;7Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. de México;8Escuela de Estadística de la Universidad Autónoma de Santo Domingo, Santo Domingo, República Dominicana;9Division of Clinical Geriatrics, Center for Alzheimer Research, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden;10Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden;11Department of Psychiatry, Cognition and Old Age Psychiatry, Sahlgrenska University Hospital, Mölndal, Sweden;12Department of Old Age Psychiatry, Institute of Psychiatry, Psychology, and Neuroscience, King's College London, London, UK
*Shared last authors.
Background: Sarcopenia is associated with multiple negative outcomes. Traditional methods to determine low muscle mass for the diagnosis of sarcopenia are mainly based on Dual-energy X-ray absorptiometry (DXA), whole-body MRI and Bioelectrical Impedance Analysis. These tests are not always available and are rather time consuming and expensive. However, many brain and head diseases require taking a head MRI. Therefore, in this study, we aim to bring a more accessible way to detect sarcopenia by comparing the traditional method of DXA lean mass estimation versus the tongue and the masseter muscle mass assessed in a standard brain MRI.
Methods: The H70 study is a longitudinal study of older people living in Gothenburg, Sweden. In this cross-sectional analysis, we included 791 participants, aged 70 year at baseline, with data and MRI images available. We used the appendicular lean soft tissue index (ALSTI) in DXA images as our reference measure of lean mass. Images from the masseter and tongue were analysed and segmented using 3Dslicer. For the statistical analysis spearman correlation coefficient was used and concordance was estimated with the Kappa coefficient.
Results: The sample was constituted of 52.3% females. We found a significant correlation coefficient between both tongue 0.26 and masseter 0.33 with ALSTI P < 0.001. Confirmed sarcopenia prevalence using the alternative muscle measure in MRI was similar to when calculated using ALSTI (tongue = 2.0%, masseter = 2.2%, ALSTI = 2.4%). Concordance between the different muscle measures with ALSTI as reference was close to 1 using both techniques.
Conclusions: ALSTI was significantly correlated with tongue and masseter muscle mass. In addition, when performing the sarcopenia diagnostic algorithm, the prevalence of sarcopenia calculated with head muscles did not differ from sarcopenia calculated using DXA and almost all participants were correctly classified using both methods.
3-27
Assessing the accuracy of estimating whole body SKM from L3 single slice and whole illiopsoas SKM
Morteza Golzan1, Telex M.N. Ngatched2, Lihong Zhang1, Maciej Michalak3, Janusz Hałka4, Da Ma5, Vincent Chow6, Hyunwoo Lee7, Mirza Faisal Beg6 and Karteek Popuri8
1Department of Electrical and Computer Engineering, Faculty of Engineering and Applied Science, Memorial University of Newfoundland, St. John's, Canada;2Department of Electrical and Computer Engineering, Faculty of Engineering, McMaster University, Hamilton, Canada;3Diagnostic Imaging Department, Warmian-Masurian Cancer Center of the Ministry of the Interior and Administration's Hospital, Department of Oncology, The University of Warmia and Mazury, Olsztyn, Poland;4Department of Clinical Haematology, Warmian-Masurian Cancer Center of the Ministry of the Interior and Administration's Hospital in Olsztyn, Olsztyn, Poland;5Department of Internal Medicine, Section of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA;6School of Engineering Science, Simon Fraser University, Vancouver, Canada;7Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, Canada;8Department of Computer Science, Faculty of Science, Memorial University of Newfoundland, St. John's, Canada
Introduction: Analysis of skeletal muscle (SKM) is important for assessing the presence of sarcopenia and has important ramifications in the oncology workflows for optimal intervention design for the individual patient. Since whole body computed tomography (CT) images are not routinely available, researchers have sought simpler proxy measurements, such as single-slice L3-mid SKM cross-sectional area (CSA) [1], or the psoas muscle CSA at the L3-mid level [2]. While regression-based analysis is accurate for group association studies as the group mean is preserved, of interest is if this regression-based approach can accurately estimate whole body measurements at the individual patient level measurements of the psoas. We hypothesize that multi-slice measurements of the psoas will be a better predictor of the whole body measurements compared to single-slice psoas CSA measurements, with larger multi-slice slabs offering increasingly more accurate estimation at the individual level.
Methods: From a whole body CT scan database, we measured SKM for the whole body as well as the entire illiopsoas muscle volume and psoas CSA at the L3-mid slice for each individual whole body CT image. The non-contrast conventional dose scans of 106 patients (42 males and 64 females) analysed were acquired on a Siemens Somatom CT at 100 KVP covering the full body, from head to toe, including the arms with axial resolution of 0.97 × 0.97 × 1.6 mm for each scan. Average age was 65.94
12.1 years for males and 66.26
11.7 for females. A linear regression model was fitted between L3-mid, Lumbar, and whole body measurements.
Results: Figure 1 shows that single L3-mid psoas CSA measurements and whole psoas volume measurements are correlated to whole body SKM measurements, with the correlation R2 being higher for psoas volumetric measurements indicating stronger linear relationship, and reduced spread around the regression line for the volumetric measures, which decreases the ambiguity of estimating whole body measurements. Figure 2 shows the percentage error of estimating whole body SKM using L3-mid psoas CSA within a regression framework indicating errors from −29.37% to 58.87% with higher errors for females than males. For the whole illiopsoas measurement, the percentage of error computed using the regression line in Figure 1 shows lower errors in estimating whole body SKM as compared to using single-slice.
Conclusions: Psoas CSA at L3-mid single-slice estimation of whole body SKM showed errors ranging up to 36.58% for males and 58.87% for females indicating that single-slice psoas CSA measurements may not be accurate enough for individual assessment. Assessment of whole iliopsoas muscle volume-based estimation of whole body SKM showed errors up to 25.55% for males and 37.25% for females, which are lower than single-slice based estimation. These findings have important implications for clinical research and practice, highlighting the need to carefully consider the selection of regions of interest when assessing body composition for individual patient assessment.
[1] Shen, W, Punyanitya, M, Wang, ZM, Gallagher, D, St.-Onge, MP, Albu, J, Heymsfield, SB, Heshka, S, Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol.2004; 97(6): 2333–8.
[2] Jones, K.I., Doleman, B., Scott, S., Lund, J.N., Williams, J.P.Simple psoas cross-sectional area measurement is a quick and easy method to assess sarcopenia and predicts major surgical complications. Colorectal disease, 2015; 17(1), pp. O20-O26.
3-28
Is single-slice (L3-mid) regression-based assessment of SKM, VAT, SAT accurate for individual patient level analysis?
Mirza Faisal Beg1, Morteza Golzan2, Lihong Zhang2, Telex M.N. Ngatched3, Maciej Michalak4, Janusz Hałka5, Da Ma6, Vincent Chow1, Hyunwoo Lee7 and Karteek Popuri8
1School of Engineering Science, Simon Fraser University, Vancouver, Canada;2Department of Electrical and Computer Engineering, Faculty of Engineering and Applied Science, Memorial University of Newfoundland, St. John's, Canada;3Department of Electrical and Computer Engineering, Faculty of Engineering, McMaster University, Hamilton, Canada;4Diagnostic Imaging Department, Warmian-Masurian Cancer Center of the Ministry of the Interior and Administration's Hospital, Department of Oncology, The University of Warmia and Mazury, Olsztyn, Poland;5Department of Clinical Haematology, Warmian-Masurian Cancer Center of the Ministry of the Interior and Administration's Hospital in Olsztyn, Olsztyn, Poland;6Department of Internal Medicine Section of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA;7Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, Canada;8Department of Computer Science, Faculty of Science, Memorial University of Newfoundland, St. John's, Canada
Introduction: Analysis of skeletal muscle (SKM), visceral adipose tissue (VAT), and subcutaneous adipose tissue (SAT) is important for assessing the presence of sarcopenia or visceral obesity and has important ramifications in the oncology workflows for optimal intervention design for the individual patient. Since whole body computed tomography (CT) images are not routinely available, using a single-slice based assessment of body composition, typically at the L3-mid level, is considered the established standard based on the high correlation of L3-mid-based measurements and whole body measurements using linear regression [1]. While regression based analysis is accurate for group association studies as the group mean is preserved [1], of interest is if this regression-based approach can accurately estimate whole body measurements at the individual patient level. We hypothesize that multi-slice measurements will be a better predictor of the whole body measurements compared to single slice L3-mid measurements, with larger multi-slice slabs offering increasingly more accurate estimation at the individual level.
Methods: From a whole body CT scan database, we measured SKM, VAT and SAT for the whole body as well as at a single L3-mid slice and Lumbar (L1 - Sacrum) multi-slice slab for each individual whole body CT image. The non-contrast conventional dose scans of 106 patients (42 males, 64 females) analysed were acquired on a Siemens Somatom CT at 100 KVP covering the full body, from head to toe, including the arms with axial resolution of 0.97 × 0.97 × 1.6 mm for each scan. Average age was 65.94
12.1 years for males and 66.26
11.7 for females. A linear regression model was fit between L3-mid, Lumbar, and whole body measurements.
Results: Figure 1 shows that single L3-mid and multi-slice L1-Sacrum SKM, VAT, SAT measurements are correlated to whole body measurements with the correlation R2 being higher for multi-slice measurements indicating stronger linear relationship, and reduced spread around the regression line, which decreases the ambiguity of estimating whole body measurements from multi-slice measurements. Figure 2 shows the percentage error of estimating whole body SKM from the regression equation [1] indicating errors from −18.5% to 47.4% with higher errors for females than males. For the L1-Sacrum slab, the percentage of error computed using the regression line in Figure 1 shows lower errors in the range −21% to +22.1% in estimating whole body SKM as compared to using single-slice.
Conclusions: L3 single-slice based estimation of whole body SKM, VAT and SAT showed errors ranging from −18.5% to 47.4% for individual assessment indicating single-slice measurements may not be accurate enough for individual assessment. These findings have important implications for clinical research and practice, highlighting the need to carefully consider the selection of regions of interest when assessing body composition for individual patient assessment.
[1] Shen, W, Punyanitya, M., Wang, Z.M., Gallagher, D., St.-Onge, M.P., Albu, J., Heymsfield, S.B., Heshka, S., Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol.2004; 97(6): 2333–8.
3-29
Automated preoperative body composition may predict pancreatic fistula risk after whipple surgery
Chet W. Hammill1, Mohammadali Mirmojarabian2, Hyunwoo Lee3, Sanghee Lee1, Rohit Srivastava1, Da Ma4, Vincent Chow5, Mirza Faisal Beg5 and Karteek Popuri2
1Department of Surgery, School of Medicine, Washington University in St. Louis, St. Louis, MO, USA;2Department of Computer Science, Faculty of Science, Memorial University of Newfoundland, St. John's, Canada;3Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, Canada;4Department of Internal Medicine Section of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA;5School of Engineering Science, Simon Fraser University, Vancouver, Canada
Introduction: Postoperative pancreatic fistulas (POPF) pose a serious adverse risk for patients after Whipple surgery (pancreatoduodenectomy). Therefore, an accurate assessment of POPF risk is crucial for predicting recovery and ensuring positive postoperative outcomes. While conventional predictors of POPF risk include small pancreatic duct, soft pancreas, high-risk pathology, and excessive blood loss [1], recent evidence suggests that incorporating computed tomography (CT) imaging-based measures may better predict fistula risk scores [2]. Body composition measures, such as skeletal muscle (SKM), visceral adipose tissue (VAT), subcutaneous adipose tissue (SAT), and intramuscular adipose tissue (IMAT), reflect nutritional status and overall fitness level. We hypothesized that a lower proportion of muscle (i.e., SKM) and a higher proportion of body fat (i.e., VAT, SAT, and IMAT) are associated with an increased risk of POPF. Given the inherent sex-related differences in body composition, we further hypothesized a differential association between males and females.
Methods: The survey included 108 patients, with 57 males and 51 females, stratified in terms of having a higher risk of fistula (Fistula Risk+; Fistula risk score of 3 or above) or a lower risk of fistula (Fistula Risk-; risk score of 2 or below). Males in the Fistula Risk+ group had a mean age of 62, compared to 68 in the Fistula Risk- group. The corresponding values for females were 60 and 65, respectively. Using CT scans acquired prior to Whipple surgery, we measured SKM, VAT, SAT, and IMAT for the whole body. General linear models (GLM) were used to conduct the comparisons. Covariates included age and Charlson co-morbidity index (CCI). GLM was fitted separately for males and females.
Results: For males, significantly higher VAT (P = 0.044), SAT (P = 0.025), and IMAT (P = 0.044) volumes were associated with higher fistula risk scores (Fistula Risk+). SKM volumes were similar between the Fistula risk groups. Associations between body composition and fistula risk were not observed in females. See Table 1.
Conclusions: Males with higher risk for fistula were associated with higher body fat proportion (VAT, SAT, and IMAT), but not associated with higher muscle proportion (SKM). The lack of similar associations in females suggests a potential sex-related effect that may stem from the different body composition between the sexes. Our findings suggest that automated CT-based markers of body composition may not only serve as a predictor of fistula risks, but also as a useful tool to investigate possible sex differences in outcome after pancreatic Whipple surgery.
1. Callery, MP, Pratt, WB, Kent, TS, Chaikof, EL, Vollmer, CMA prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. J Am Coll Surg.2013 Jan; 216(1): 1–14. https://doi.org/10.1016/j.jamcollsurg.2012.09.002. Epub 2012 Nov 2. PMID: 23122535.
2. Jin, J, Xiong, G, Li, J, Guo, X, Wang, M, Li, Z, Zhu, F, Qin, R. Predictive factors of postoperative pancreatic fistula after laparoscopic pancreatoduodenectomy. Ann Transl Med.2021 Jan; 9(1): 41. https://doi.org/10.21037/atm-20-1411. PMID: 33553334; PMCID: PMC7859741.
3-30
Validation of a deep learning model for automatic segmentation of skeletal muscle and adipose tissue on L3 abdominal CT images
David P.J. van Dijk1,2, Leroy F. Volmer3, Ralph Brecheisen1,2, Ross D. Dolan4, Adam S. Bryce5,6, David K. Chang5,6, Donald C. McMillan4, Jan H.M.B. Stoot7, Malcolm A. West8, Sander S. Rensen1,2, Andre Dekker2, Leonard Wee‡, 2 and Steven W.M. Olde Damink‡, 1,2,9
1Department of Surgery, Maastricht University Medical Centre, Maastricht, The Netherlands;2NUTRIM School of Nutrition and Translational Research in Metabolism, Maastricht University, The Netherlands;3Department of Radiotherapy (MAASTRO), School of Oncology and Reproduction, Maastricht University, Maastricht, The Netherlands;4Academic Unit of Surgery, School of Medicine, University of Glasgow, Glasgow Royal Infirmary, Glasgow, UK;5Wolfson Wohl Cancer Research Centre, School of Cancer Sciences, University of Glasgow, Glasgow, UK;6West of Scotland Pancreatic Unit, Glasgow Royal Infirmary, Glasgow, UK;7Department of Surgery, Zuyderland Medical Centre, Sittard-Geleen, UK;8Academic Unit of Cancer Sciences, Faculty of Medicine, University of Southampton, Southampton, UK;9Department of General, Visceral and Transplant Surgery, University Hospital Aachen, Aachen, Germany
†Contributed equally as first authors.
‡Contributed equally as last authors.
Background: Body composition assessment using abdominal computed tomography (CT) images is increasingly applied in clinical and translational research. Manual segmentation of body compartments on L3 CT images is time-consuming and requires significant expertise. Robust high-throughput automated segmentation is key to assess large patient cohorts and ultimately, to support implementation into routine clinical practice. By training a deep learning neural network (DLNN) with several large trial cohorts and performing external validation on a large independent cohort, we aim to demonstrate the robust performance of our automatic body composition segmentation tool for future use in patients.
Methods: L3 CT images and expert-drawn segmentations of skeletal muscle, visceral adipose tissue, and subcutaneous adipose tissue of patients undergoing abdominal surgery were pooled (n = 3187) to train a DLNN. The trained DLNN was then externally validated in a cohort with L3 CT images of patients with abdominal cancer (n = 2535). Geometric agreement between automatic and manual segmentations was evaluated by computing two-dimensional Dice Similarity (DS). Agreement between manual and automatic annotations were quantitatively evaluated in the test set using Lin's Concordance Correlation Coefficient (CCC) and Bland–Altman's Limits of Agreement (LoA).
Results: The DLNN showed rapid improvement within the first 10 000 training steps and stopped improving after 38 000 steps. There was a strong concordance between automatic and manual segmentations with median DS for skeletal muscle, visceral adipose tissue, and subcutaneous adipose tissue of 0.97 (interquartile range, IQR: 0.95–0.98), 0.98 (IQR: 0.95–0.98), and 0.95 (IQR: 0.92–0.97), respectively. Concordance correlations were excellent: skeletal muscle 0.964 (0.959–0.968), visceral adipose tissue 0.998 (0.998–0.998), and subcutaneous adipose tissue 0.992 (0.991–0.993). Bland–Altman metrics (relative to approximate median values in parentheses) indicated only small and clinically insignificant systematic offsets: 0.23 HU (0.5%), 1.26 cm2/m−2 (2.8%), −1.02 cm2/m−2 (1.7%), and 3.24 cm2/m−2 (4.6%) for skeletal muscle average radiodensity, skeletal muscle index, visceral adipose tissue index, and subcutaneous adipose tissue index, respectively. Assuming the decision thresholds by Martin et al. for sarcopenia and low muscle radiation attenuation, results for sensitivity (0.99 and 0.98, respectively), specificity (0.87 and 0.98, respectively), and overall accuracy (0.93) were all excellent.
Conclusions: We developed and validated a deep learning model for automated analysis of body composition of patients with cancer. Due to the design of the DLNN, it can be easily implemented in various clinical infrastructures and used by other research groups to assess cancer patient cohorts or develop new models in other fields.
4-01
Involvement of the CXCR4/CXCL12 axis in skeletal muscle dysfunction in an early murine model of COPD
Pauline Henrot1,2, Pierre Schilfarth1,2, Marilyne Campagnac1, Elise Maurat1, Marina Gueçamburu1,2, Pauline Estèves1, Jean-William Dupuy3, Maéva Zysman1,2, Patrick Berger1,2 and Isabelle Dupin1
1Centre de Recherche Cardio-thoracique de Bordeaux, Univ-Bordeaux, Pessac, France;2Service d'exploration fonctionnelle respiratoire, CHU de Bordeaux, Pessac, France;3Plateforme Protéome, Univ. Bordeaux, Bordeaux, France
Introduction: Chronic Obstructive Pulmonary Disease (COPD) is a vastly prevalent respiratory disease, currently the third leading cause of death, and is now considered as a systemic inflammatory disease. Sarcopenia affects up to 35% of the patients and increases mortality up to ten-fold. However, no effective treatment is available to date and triggering pathophysiological mechanisms remain unclear. The implication of the CXCL12/CXCR4 axis has been suggested in COPD development. We aimed here at studying its role in COPD skeletal muscle dysfunction.
Methods: We developed a murine model of early-phase COPD by exposing C57BL/6 mice for 10 weeks to cigarette smoke (CS) and intranasal instillations of poly-IC to mimic exacerbations, thereby leading to bronchial obstruction, peri-bronchial fibrosis and right ventricle thickening (Dupin et al, submitted). A conditional inactivation of CXCR4 was also generated via a tamoxifen-inducible Cre/Lox system in CS and poly-IC-exposed mice. Skeletal muscle function was assessed using the grip test (muscle force) and the hanging test (muscle endurance), and skeletal muscle tissues were harvested for histological and proteomic analysis.
Results: There was no difference in muscle mass or muscle force between control and exposed mice, underlying the absence of sarcopenia features in this early-phase model. However, we evidenced a decreased endurance in exposed mice, which was not present in CXCR4−/− exposed mice (Figure 1A). In agreement, the proportion of type IIx glycolytic myofibres was significantly increased in the Soleus of exposed mice, and was similar to controls in CXCR4−/− exposed mice (Figure 1B). Capillarization was unchanged between the three groups. However, we evidenced moderately increased inflammation in Soleus muscle, evidences of moderate hypoxia, as well as indirect evidences of neuromuscular junction (NMJ) degeneration in exposed mice. Proteomic analysis evidenced inversely regulated contractile and inflammatory pathways in exposed mice and CXCR4−/− exposed mice, as well as an increase in mitochondrial proteins (Figure 1C).
Conclusions: Decreased endurance linked to increased glycolytic myofibres proportion might be the initial event preceding sarcopenia in COPD, and is prevented by CXCR4 deletion. The fibre-type switch is likely to be multifactorial and linked both to inflammation, NMJ degeneration and hypoxia, which might initially be compensated by an increased in mitochondrial proteins. These results provide a framework to study the CXCL12/CXCR4 axis and implicated cells in COPD early skeletal muscle dysfunction.
4-02
A novel in vitro model of senescent murine myoblasts and sarcopenic myotubes to highlight skeletal muscle involvement in the aging phenotype
Laura Gerosa and Marta Gomarasca and Amir Mohammad Malvandi and Martina Faraldi and Veronica Sansoni and Giovanni Lombardi
Laboratory of Experimental Biochemistry and Molecular Biology, IRCCS Ospedale Galeazzi Sant'Ambrogio, Milano, Italy
Introduction: Although impairment of muscle mass and strength almost invariably features the human aging phenotype, availability of in vitro models of skeletal muscle senescence is limited and, where available, these models recapitulate only a restricted panel of phenotypic features of the senescent cells in vivo. Further, no studies have defined the role of muscle-bone crosstalk in the aging of the muscle-skeletal apparatus. With this work, we aimed at developing a new in vitro model of senescent myoblasts and sarcopenic-like myotubes to be used for the identification of biomarkers associated with sarcopenia that concurred to muscle-skeletal frailty phenotype of the elderly.
Methods: C2C12 mouse myoblasts were treated for 72 h with 0 μM, 0.4 μM, 1 μM and 2 μM SYUIQ-5, an inhibitor of telomerase activity. Senescent myoblasts were differentiated into myotubes for 4 and 7 days by supplementing the medium with horse serum (2%). The senescent phenotype of myoblasts and myotubes was characterized. Then, MC3T3 murine pre-osteoblasts were differentiated for 14 days, in presence or not of conditioned media derived from senescent myoblasts, and the osteogenic differentiation potential was analysed.
Results: 2 μM SYUIQ-5 treatment resulted cytotoxic for myoblasts, while increasing concentration of SYUIQ-5 significantly decreased myoblasts proliferation; 1 μM SYUIQ-5 for 72 h induced the expression of the typical hallmarks of senescence in myoblasts: enhanced expression of p21 transcript and protein, enhanced p53 and histone H2AX phosphorylation (ƴ-H2AX), accumulation of nuclear foci enriched in ƴ-H2AX, upregulation of senescence-associated β-galactosidase (SA-βgal) activity.
Confocal microscopy analysis revealed the impaired potential of senescent myoblasts to differentiate into myotubes and these resulting cells showed typical features of sarcopenic myotubes: downregulation of myosin heavy chain (MYHC), upregulation of MurF1 and atrogin, two markers of muscle catabolism, and reduced mitochondria content.
Supernatants from sarcopenic-like myotubes were enriched in myostatin, muscle growth inhibitor, and impoverished of osteoprotegerin, inhibitor of osteoclasts differentiation, as muscle-specific hallmarks of the senescence-associated secretory phenotype (SASP).
Finally, preliminary experiments showed that the osteoblastic differentiation of murine pre-osteoblasts cultured with conditioned media of senescent murine myoblasts was impaired.
Conclusions: Here we describe an in vitro model of senescent murine myoblasts recapitulating the main hallmarks of senescence and myotubes expressing a sarcopenic phenotype. Our model can be useful in future studies aimed at identifying the molecular mechanisms of muscle senescence and at finding out SASP markers with relevant roles in bone-muscle crosstalk during aging.
4-03
The effect of doxorubicin on skeletal muscle mass and myokine expression in Lewis lung cancer bearing mice
Birgit Van Asbroeck1, Dorien Dombrecht1, Emeline Van Craenenbroeck2,3, Pieter-Jan Guns4 and Eric Van Breda1
1Department of Rehabilitation Sciences & Physiotherapy, Research Group MOVANT, University of Antwerp, Antwerp, Belgium;2Research Group Cardiovascular Diseases, University of Antwerp, Antwerp, Belgium;3Department of Cardiology, Antwerp University Hospital, Antwerp, Belgium;4Laboratory of Physiopharmacology, University of Antwerp, Antwerp, Belgium
Introduction: Cancer cachexia is characterized by severe skeletal muscle mass loss. Chemotherapeutic treatment with Doxorubicin (DOX) worsens skeletal muscle mass loss but the underlying mechanisms through which DOX exerts its catabolic effect remain incompletely understood. Moreover, the role of myokines, secreted by skeletal muscle and involved in muscle homeostasis, is unknown. We examined the effect of DOX on myokine expression and pathways regulating skeletal muscle protein degradation in a Lewis lung carcinoma (LLC) mice model.
Methods: Sixteen 9 week-old C57BL6/J male mice were divided into: (1) Control, (2) LLC and (3) LLC receiving DOX groups. LLC mice were subcutaneously injected with 5 × 105 LLC cells into the flank. DOX was administered intraperitoneally (2×/week 2.5 mg/kg) up to a cumulative dose of 10 mg/kg. Twenty-one days after tumour inoculation, mice were euthanized and the extensor digitorum longus (EDL), soleus (SOL) and gastrocnemius (GAS) muscle were collected (Figure 1). Myokine expression of myostatin, decorin and irisin and key proteins of skeletal muscle proteolysis (FOXO3a, MURF-1 and Atrogin-1) were evaluated by Western blotting (Figure 2). Differences between groups were considered significant if P < 0.05(*).
Results: DOX-treated LLC mice showed a non-significant decrease in body weight that could be partly attributed to skeletal muscle mass loss, as shown by lower muscle/body weight ratios for GAS* and EDL. As anticipated, DOX treated mice developed smaller tumours (−35% tumour volume and weight). Interestingly, expression levels of myostatin*, FOXO3a*, MURF-1* and Atrogin-1* in the EDL were found to be increased in DOX-treated LLC mice compared to control and/or LLC mice. Additionally, a decrease of decorin* in the EDL was found for both DOX-treated and untreated LLC mice. Irisin levels were unchanged. For the SOL no alterations in myokine expression and protein degradation were observed.
Conclusions: We show that DOX increases protein degradation despite its important therapeutic effect in tumour reduction, revealing an effect of DOX to muscle wasting observed with cancer. Moreover, altered expression of myokines are likely to contribute to the development of muscle wasting. Finally, the catabolic effect of DOX seems to be muscle type dependent.
4-04
The Rho GTPase inhibitor, RhoGDIα is a negative regulator of muscle mass and upregulated in sarcopenic human muscle
Lisbeth L.V. Møller1,2, Kevin I. Watt3,4, Jakob Agergaard5,6, Anders Karlsen5,6,7, Nicoline R. Andersen2, Peter Schjerling5,6, Hongwei Qian8, Michael Kjær5,6, Paul Gregorevic8, Erik A. Richter2 and Lykke Sylow1,2
1Molecular Metabolism in Cancer and Aging, Endocrinology and Metabolism, Department of Biomedical Sciences, University of Copenhagen, Copenhagen, Denmark;2The August Krogh Section for Molecular Physiology, Department of Nutrition, Exercise and Sports, Faculty of Science, University of Copenhagen, Copenhagen, Denmark;3Novo Nordisk Foundation Center for Stem Cell Medicine, reNEW Melbourne, Melbourne, Australia;4Dept of Anatomy and Physiology, University of Melbourne, Melbourne, Australia;5Institute of Sports Medicine Copenhagen, Department of Orthopedic Surgery, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark;6Center for Healthy Aging, Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark;7Xlab, Center for Healthy Aging, Department of Biomedical Sciences, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark;8Center for Muscle Research, Department of Physiology, University of Melbourne, Melbourne, Australia
Introduction: Maintaining skeletal muscle mass is mandatory for upholding an independent lifestyle and muscle strength is inversely associated with all-cause mortality. Despite this, there are no clinically approved drugs to improve muscle growth and strength. Determining new molecular mechanisms regulating muscle mass would help identify new candidates for treatment. Rho GTPase signalling is one of the most regulated pathways in response to resistance exercise. Since resistance exercise potently increases muscle growth, Rho GTPases are exciting, yet, largely unexplored candidates for muscle mass control. Rho GTPases are promiscuously inhibited by the molecular chaperone Rho guanine nucleotide dissociation inhibitor α (RhoGDIα). By transgenically up- or down-regulating RhoGDIα muscle protein content (inhibiting or activating Rho GTPases, respectively), we investigated the role of Rho GTPases in muscle mass regulation and mechanisms of action.
Methods: RhoGDIα was overexpressed or knocked down specifically in the skeletal muscle of C57BL/6JBomTac mice after a single intramuscular injection using recombinant adeno-associated virus (rAAV)-mediated delivery of DNA or shRNA targeting RhoGDIα, respectively. Muscle mass was measured and by proteomic analysis and immunoblotting techniques, molecular markers of muscle wasting and hypertrophy were investigated. Human vastus lateralis muscle from healthy untrained young (age 20–30 years), elderly (age 60–75 years) and old, sarcopenic (age 83–94 years) men were analysed for RhoGDIα protein content.
Results: RhoGDIα overexpression reduced muscle mass (TA: −8%), while knockdown of RhoGDIα increased muscle mass (EDL: +20%, TA: +7–9%; Gast: +8%). Proteomics analyses revealed significant changes in the ubiquitin-proteasome system, which is involved in the regulation of skeletal muscle mass. Moreover, RhoGDIα overexpression-induced atrophy was associated with downregulation of the Hippo pathway-YAP/TAZ protein content with no changes in mTORC1 signalling. In contrast, RhoGDIα knockdown-induced hypertrophy was, despite reduced mTORC1 signalling and unchanged YAP/TAZ protein content, potentially partly explained by downregulated E3 ubiquitin ligase, MuRF1 protein content and autophagy indicator LC3-II protein content. Further suggesting a role for RhoGDIα in age-induced muscle wasting, RhoGDIα protein content was upregulated (+45%) in human skeletal muscle from old, sarcopenic patients and RhoGDIα protein content tended (P = 0.0877) to be negatively correlated with type II fibre cross-sectional area.
Conclusions: Altogether these data identify RhoGDIα as a negative regulator of muscle mass and possibly a mediator of age-induced muscle wasting. Accordingly, resolving the molecular mechanisms of RhoGDIα-induced muscle mass regulation can potentially provide novel pharmacological targets and therapeutic interventions, which are important because of the demographic evolution of an increasing proportion of elderly citizens.
4-05
ADAR2 deficiency alleviates muscle atrophy in HFD-induced obese mice
Chia-Chi Lin and Yun-Wen Chen
Department of Pharmacology, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Introduction/Background: Obesity is an extremely prevalent chronic disease that can induce metabolic syndrome and is associated with a more risk of muscular atrophy. Adenosine-to-inosine (A-to-I) editing, catalysed by adenosine deaminase acting on RNA (ADAR), is an important post-transcriptional modification of genome-encoded RNA transcripts. Three fundamentally related members of ADAR family including ADAR1, ADAR2 and ADAR3 have been identified. In this study, we aim to investigate the role of ADAR2 in skeletal muscle atrophy.
Methods: ADAR2+/+ (wild type, WT) and ADAR2−/− (ADAR2 KO) mice were subjected to feed with standard chow or high-fat-diet (HFD) for 20 weeks at the age of 5 weeks. Muscle mass, muscle strength, cross-sectional area, markers of protein synthesis/degradation, glucose/insulin tolerance were measured.
Results: ADAR2 KO alleviated the fasting blood glucose, insulin resistance and glucose intolerance in HFD-induced obese mice. ADAR2 KO increased muscle mass, muscle strength, and muscle endurance in HFD-induced obese mice. Muscle cross-sectional analysis of gastrocnemius revealed increases in fibre size distribution in ADAR2 KO mice fed with HFD. ADAR2 KO attenuates HFD-induced local skeletal muscle tissue Inflammation. Moreover, muscle atrophy-associated transcripts, such as FOXO1, MAFbx/Atrogin-1, MuRF1/TRIM63, were decreased in ADAR2 KO mice fed with HFD compared to HFD-WT mice.
Conclusions: These results provide novel evidence that ADAR2 KO may mediate the protective effect of obesity-induced muscle wasting and weakness.
4-06
Urocortin 2 modulates muscle mass associated with insulin/IGF-1 signalling pathway stimulation in skeletal muscles of obese and denervated mice
Natalia Lautherbach1, Dawit Albieiro Pinheiro Gonçalves2, Ana Paula Assis1, Rafael Rossi Valentim3, Lilian do Carmo Heck3, Luiz Carlos Carvalho Navegantes3 and Isis do Carmo Kettelhut1,3
1Department of Biochemistry/Immunology, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, Brazil;2Department of Physical Education, Federal University of Minas Gerais, Belo Horizonte, Brazil;3Department of Physiology, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, Brazil
Introduction: Urocortin 2 (Ucn2) modulates skeletal muscle (SM) mass of rodents, however, the intracellular mechanisms responsible for these findings remained unclear. We have recently demonstrated that the hypertrophic effect promoted by Ucn2 in vivo was associated with a crosstalk, probably mediated by Epac, between urocortinergic canonic signalling pathway (cAMP/PKA/CREB) and insulin pathway (Akt/mTOR/S6; Akt/Foxo) in SM of normal mice. The objective of this work is to investigate the effects of Ucn2 in SM in a model of insulin resistance induced by diet and also in an atrophic model induced by motor denervation.
Methods: C57Bl/6J male mice (8 weeks) received hyperlipidic diet (HL; 35% of lipids) for 3 months and to induce muscle atrophy, male mice (8 weeks) were surgically denervated (DEN). Using electroporation technique, empty vector (pcDNA3.1+) or Ucn2 plasmid was transfected in vivo into tibialis anterior (TA) muscles of obese (14 days before euthanasia) and 14-days-DEN mice (the transfection occurred in the same day of the denervation surgery). Then, TA were excised and processed to determine the expression of genes and proteins of interest. Protein synthesis was analysed by the SUnSET method. Student's t-test was used to analyse data. Ethic committee approval: 063/2014.
Results: HL diet induces body gain mass, hyperglycaemia, hyperinsulinaemia and a tendency in decrease muscle mass indirectly measured by total protein content associated with a propensity in increase protein synthesis. HL diet reduces the phosphorylation levels of Akt (Ser473; Thr308), S6 (Ser235/236; Ser240/244) and FoxO1 (Ser256) and these effects were completed reverted by Ucn2 overexpression in TA of obese mice. Ucn2 in vivo reduced the protein expression of E3-ligases (atrogin and MuRF-1) in TA muscles of obese mice. In addition, HL diet decreases the protein content of LC3-II, an autophagy marker, and this effect were completed reverted by Ucn2 overexpression suggesting inhibition of lysosomal-autophagic proteolytic system. Ucn2 in vivo increased the protein expression of slow myosin heavy chain associated with an augmented in PGC1-α protein content in TA of obese mice. Unc2 partially reverted the atrophy induced by denervation measured by TA weight in DEN mice.
Conclusions: Ucn2 exerts its effects in SM of insulin resistant and atrophic models probably through insulin/IGF-1 signalling pathway stimulation. This research rises up new perspectives for the development of therapeutic strategies to protect muscle mass and also to cope with insulin resistance induced by HL diet.
4-07
Cyp27b1 ablation in skeletal muscle impairs muscle regeneration
Hiu-tung Jessica Lo1,2, Tszlam Yiu1,2, Daniel Kam-Wah Mok3,4,5, Man-Sau Wong3,4,5 and Wayne Yuk-wai Lee1,2,6,7,8
1Musculoskeletal Research Laboratory, SH Ho Scoliosis Research Laboratory, Department of Orthopaedics & Traumatology, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China;2Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong SAR, China;3State Key Laboratory of Chinese Medicine and Molecular Pharmacology (Incubation), The Hong Kong Polytechnic University Shenzhen Research Institute, Shenzhen, China;4Research Centre for Chinese Medicine Innovation, The Hong Kong Polytechnic University, Hong Kong SAR, China;5Department of Applied Biology and Chemical Technology, The Hong Kong Polytechnic University, Hong Kong SAR, China;6Joint Scoliosis Research Centre of the Chinese University of Hong Kong and Nanjing University, The Chinese University of Hong Kong, Hong Kong SAR, China;7Center for Neuromusculoskeletal Restorative Medicine, CUHK InnoHK Centres, Hong Kong Science Park, Hong Kong SAR, China;8Key Laboratory for Regenerative Medicine, Ministry of Education, School of Biomedical Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, Hong Kong
Introduction: Muscle regeneration involves various cellular and molecular mechanisms. Vitamin D is important in muscle function and repair. Cyp27b1 activates vitamin D into 1,25-dihydroxyvitamin-D3 inside mitochondrial inner membrane, which promotes muscle contraction velocity and strength. (Girgis, Clifton-Bligh, Hamrick, Holick, & Gunton, 2013). The local effects of cyp27b1 in muscle and extra-renal activation of vitamin D are not well understood. Global knockout cyp27b1 mice results in decreased muscle mass due to increased oxidative stress (Yu et al., 2021). Understanding the relationship between cyp27b1 and mitochondrial function may provide insights into underlying mechanisms of muscle degeneration.
Method:In vivo cyp27b1 knockdown was induced in male cyp27b1 floxed mice (3.5 months old) via bilateral gastrocnemius (GAS) intra-muscular injection of AAV9-CMV-CRE-GFP virus (100 μL, 2 × 1012 μg/mL). After 10 days, GAS was collected for fibre type analysis, ex vivo functional testing, and qPCR. (n = 3). Muscle injury was induced via I.M. injection of BaCl2 (1.2% w/v, 50 μL) in bilateral gastrocnemius 10 days after virus injection and observed for 7 days to evaluate muscle regeneration by H&E staining and qPCR. C2C12 myoblasts was used in loss-of-function and gain-of-function studies (n = 3). One-way ANOVA and two-way ANOVA were used for the animal and cellular studies, respectively. The level of significance was set at P < 0.05.
Results:In vivo knockdown of cyp27b1 reach up to 90% efficiency by qPCR. The knockdown resulted in significant changes in muscle fibre type distribution, i.e., type I (WT: 0.36%; KD 11.9%) and type IIA (WT: 23.5%; KD: 46.4%) /IIB (WT: 76%; KD: 41.6%) and decrease in muscle force, specifically reduction in specific twitch force (−16%) and specific tetanic force (−29%). KD group showed lower mitochondrial biogenesis marker expression than the control, as indicated by qPCR and western blot. Following injury, there was decreased gene expression related to muscle regeneration and mitochondria biogenesis, delayed regeneration and increased immune cell infiltration were also observed. Cyp27b1 knockdown in C2C12 suppressed myogenic and mitochondrial biogenesis marker expression and proliferation, while overexpression had the opposite effect.
Discussion: Our findings suggest cyp27b1 plays a critical role in muscle regeneration after injury, likely due to its extra-renal effect on vitamin D metabolism in muscle tissues. The findings suggest potential for developing new therapeutic strategies for treating muscle damage, including the discovery of novel Cyp27b1 activators that could extend to other muscular disorders.
Girgis, C. M., Clifton-Bligh, R. J., Hamrick, M. W., Holick, M. F., & Gunton, J. E. (2013). The Roles of Vitamin D in Skeletal Muscle: Form, Function, and Metabolism. Endocrine Reviews, 34(1), 33–83. https://doi.org/10.1210/er.2012-1012
Yu, S., Ren, B., Chen, H., Goltzman, D., Yan, J., & Miao, D. (2021). 1,25-Dihydroxyvitamin D deficiency induces sarcopenia by inducing skeletal muscle cell senescence. American journal of translational research, 13(11), 12638–12649. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34956479https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8661220/
4-08
Role of mechanosensitive components in the regulation of myogenic differentiation
Alexander Pacolet1,2, Mathias Vanmunster2,3, Inge Derese1, Maxime Smits4,5, Lies Langouche1 and Rik Gijsbers4,5
1Laboratory of Intensive Care Medicine, Department of Cellular and Molecular Medicine, KU Leuven, Leuven, Belgium;2Exercise Physiology Research Group, Department of Movement Sciences, KU Leuven, Leuven, Belgium;3Skeletal Biology and Engineering Research Center, Department of Development and Regeneration, KU Leuven, Leuven, Belgium;4Molecular Virology and Gene Therapy, Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium;5Leuven Viral Vector Core, Biomedical Sciences, KU Leuven, Leuven, Belgium
Introduction: Mechanosensors are a class of proteins, capable of sensing mechanical forces and transmitting signals to the cytosol and nucleus, initiating changes in gene expression and other cellular processes. In muscle cells, these mechanosensors are potentially not only important in response to mechanical loading/unloading but also during differentiation and regeneration. A critical role is attributed to the mechanosensitive integrins, a family of transmembrane receptors that provide the interaction between the extracellular matrix and the cytoskeleton. Processes of integrin activity, clustering and signalling are regulated by various cytoplasmic proteins including integrin-linked-kinase-1 (Ilk1 gene) and kindlin2 (Fermt2 gene). This study aims to enhance understanding of the role of Ilk1 and Kindlin2/Fermt2 during mouse muscle cell differentiation.
Methods: Mouse myoblast C2C12 cells were transduced by lentiviral vectors expressing microRNA-based shRNA (miR) targeting Ilk1 or Fermt2. miR-fLuc was used as control. Differentiation medium (DMEM, 2% horse serum, 1% Pen-Strep) was added to transduced cells at 90% confluency in 6-well plates. At start and 1, 3, 5, and 7 days after differentiation initiation, cells were stained for DAPI and MyHC to determine myoblast fusion index (number of nuclei inside myotubes divided by total number of nuclei). Knockdown efficiency and mRNA expression of differentiation markers (Pax7, MyoD, MyoG, Myh1, Acta1) and mechanosensory components (Ilk1, Fermt2, Itgb1, Itga7) were evaluated by qPCR. All measurements were done in triplicates.
Results: Lentiviral delivery of Ilk1 miR caused a stable 10-fold knockdown (P < 0.0001) of Ilk1 expression and reduced myotube differentiation with a 3-fold-lower fusion-index at day 7 (P < 0.001) relative to miR-fLuc. Ilk1 knockdown elevated expression of myogenic differentiation markers Pax7, MyoD, MyoG, and Acta1 at D0 (P ≤ 0.0001), but the differentiation-induced further increase was blunted (P ≤ 0.0001 at D7). Increased expression of Itga7 was similarly blunted throughout differentiation (P ≤ 0.01), whereas Itgb1 or Fermt2 were not affected by differentiation or Ilk1 knockdown. In contrast, in Fermt2-KD cells, Fermt2 expression rapidly increased from a 1.45-fold reduction (P < 0.0001) at differentiation initiation reaching similar expression levels as controls from D1 onwards. Differentiation markers were not affected, but both Ilk1 and Itga7 expression increased with Fermt2 knockdown.
Conclusions: The mechanosensing components Ilk1 and Itga7 are affected in myogenic differentiation in C2C12 cells. Whether the lack of effect of Fermt2 knockdown on myogenic differentiation was due to its upregulation during differentiation or to compensatory upregulation of Ilk1 and Itga7 has to be further investigated.
4-09
MRI-based characterization of muscles in aging mice fed on high-energy diet and sedentary lifestyle
Beatrice Matot and Ericky Caldas de Almeida Araujo and Pierre-Yves Baudin and Harmen Reyngoudt and Benjamin Marty and Yves Fromes
NMR Laboratory, Neuromuscular Investigation Center, Institute of Myology, Paris, France
Introduction: The investigation of age-induced alterations in humans is time consuming and resource intensive. One important question for the evaluation of aging is how similar changes over a lifetime are between humans and mice. Our primary goal was to assess leg muscle's trophicity and structure based on Magnetic Resonance Imaging (MRI) and function in a cohort of mice exposed to a high-energy diet and a sedentary lifestyle.
Methods: In this preliminary longitudinal study, C57Bl/6JRj male mice were used, fed ad libidum with high-energy diet (Safe®; EM Pig 3237 kcal/kg). Ten mice were scanned on a 7 T MRI Bruker system with a surface cryoprobe positioned next to the Tibialis anterior (TA) muscle from 2.5 to 22 months of age (m). The MRI study included high-resolution anatomical images and T2 maps to evaluate muscle cross-sectional area (CSA) and muscle T2, respectively. Muscle strength was evaluated at 4.5, 12 and 19 m by a grip test. ANOVA and t-test were used to analyse MRI and functional data, respectively (P-value < 0.05 for statistical significance).
Results: A Kaplan–Meier curve pointed out an increased mortality in our cohort with a survivorship of 50% around 20 m unlike data commonly reported for this strain. In parallel, mice body weight (g) increased in a normal range with age (2.5 m: 26.9 ± 2.1; 22 m: 33.0 ± 2.5).
Grip tests emphasized a negative effect of age on force with a significant decrease of the maximal force normalized by BW (g/g) between 4.5 and 12 m (4.5 m: 7.2 ± 1.35; 12 m: 5.2 ± 1; P < 0.05). Mean CSA (mm2) of TA tended to increase until 9 m then decreased with age (2.5 m: 7.6 ± 0.4; 9 m: 8 ± 0.4; 12 m: 7.6 ± 0.3; P = 0.069). Finally, muscle T2 increased with age (P < 0.05) mainly during growth.
Conclusions: High-energy diet and sedentary lifestyle have negative effects on life expectancy that could not be linked in our study to overweight as BW increased in a normal range with age. Additional individuals are necessary to investigate if the loss of muscle function after growth is due to muscle wasting and/or to changing in muscle tissue structure as T2, related to inflammation and muscle architecture, is increased with age. C57Bl/6 mice may represent a well-suited model to explore aging and muscle wasting.
4-10
MR-based characterization of aging in human muscles
Alfredo Lopez and Béatrice Matot and Jean-Marc Boisserie and Sophie Jouan and Ericky Caldas and Pierre-Yves Baudin and Benjamin Marty and Harmen Reyngoudt and Yves Fromes
Institute of Myology, Neuromuscular Investigation Center, NMR Laboratory, Groupe Hospitalier Pitié-Salpêtrière, Paris, France
Introduction: The typical adult will lose muscle mass with age; the loss varies according to sex and the level of muscle activity. Our primary goal was to assess leg muscle's trophicity, structure, function and biochemistry based on quantitative MR examination in a prospective open label study to benchmark various outcome measures.
Methods: Inclusion criteria were based on clinical screening, absence of any chronic disorder, age >20 years. Physical activity assessment, grip test, gait speed were evaluated. 3T MRI scanner, homemade magnetic ergometer and a standardized exercise protocol for plantar flexion were used. Cross sectional area, fat fraction and water T2 were measured. Interleaved MR sequences were developed to assess perfusion; BOLD-effect used deoxygenated haemoglobin as endogenous contrast; deoxymyoglobin (dMb) provided a means to monitor the oxygenation state of muscle. Descriptive statistics express results as mean ± SEM. Group comparison was based on T test and ANOVA.
Results: We present preliminary results on N = 61, aged 20 to 81 years, M/F ratio: 31:30. Volunteers were stratified as young (>35 years; N: 15), middle-aged (35–60 years; N: 25) and elderly (>60 years; N: 18). Of our cohort, 84% were either active or very active. Handgrip strength normalized by BMI changed only marginally over time. Gait speed normalized by height slightly decreased. Maximum plantar flexion force normalized by height did not change significantly.
Cross-sectional areas of triceps surae barely changed with age. Intramuscular fat fraction increased with age (0.11 ± 0.03; 0.16 ± 0.04; 0.19 ± 0.04, respectively). Intrinsic T2 values (ms) increased with age (36.5 ± 1.6; 37.3 ± 1.9; 38.8 ± 1.5, respectively).
Exercise induced most significant increase in the gastrocnemius muscles. Relative increase of perfusion was most important in mild-aged individuals. Increase in workload induced a raise in T2*, mostly in the gastrocnemius muscles, mainly in younger individuals. Whereas, dMb showed higher values at work in elderly people.
Conclusions: NMR provides interesting tools to assess not only structural aspects of the aging muscles, but our innovative set-up allows to investigate functional and biochemical aspects also. Fatty infiltration of skeletal muscles appears to increase with age, as do T2 values. The dynamic range of blood perfusion rate in skeletal muscle is significantly higher than in any other organ. Adjustments occur as age progresses and can be monitored non-invasively. Regular activity seems to preserve muscle mass and function, but more subtle changes can be observed by MRI.
4-12
Long-term musculoskeletal consequences of chemotherapy in paediatric mice
Joshua R. Huot1,2,3, Fabrizio Pin1,2,3, Nicholas A. Jamnick4, Patrick D. Livingston4 and Andrea Bonetto4,5
1Department of Anatomy, Cell Biology & Physiology, Indiana University School of Medicine, Indianapolis, IN, USA;2Simon Comprehensive Cancer CenterIndiana University School of Medicine, Indianapolis, IN, USA;3Indiana Center for Musculoskeletal Health, Indiana University School of Medicine, Indianapolis, IN, USA;4Department of Pathology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA;5University of Colorado Comprehensive Cancer Center, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Introduction: Thanks to the recent progress in cancer research, nowadays most children treated for cancer survive into adulthood. Nevertheless, little is known about the long-term consequences of anticancer agents, especially in the paediatric population. We and others have shown that routinely administered chemotherapeutics can drive musculoskeletal alterations consistent with loss of muscle mass and strength, as well as bone decay, which altogether contribute to increased treatment-related toxicity and long-term morbidity and negatively impair cancer survival. Yet, the mechanisms responsible for enduring muscle and bone defects following anticancer treatments and whether these can potentially impact growth and quality of life in young individuals remain to be elucidated. Here, we aimed at investigating the late musculoskeletal effects of Folfiri, a chemotherapy regimen which we previously extensively characterized, in paediatric mice.
Methods: Three-week-old male C57BL6/J mice were administered Folfiri (5-FU, leucovorin, irinotecan; n = 10) or vehicle (n = 5) intraperitoneally for up to 5 weeks and followed up for up to 4 weeks after cessation of the treatment. Body composition, plantarflexion force and EMG were assessed at baseline and at regular intervals. At time of sacrifice, skeletal muscle, bones and other tissues were collected, processed and stored for further analyses.
Results: Body weight gain was significantly delayed in the mice receiving chemotherapy, resulting in progressively lower carcass weight at sacrifice, diminished lean and fat mass, as well as significantly smaller skeletal muscles. Consistently, muscle function was progressively impaired in the mice exposed to chemotherapy. BMC and BMD were also reduced upon 5 weeks of treatment with Folfiri, in line with loss of trabecular bone. Interestingly, 4 weeks after cessation of the treatment, the animals exposed to chemotherapy showed persistent musculoskeletal defects, consistent with lower bone mass, decreased lean and fat content and reduced muscle weights and function, in agreement with reduced levels of muscle mitochondrial proteins.
Conclusions: Our data supports the idea that anticancer treatments may lead to long-lasting musculoskeletal complications in actively growing paediatric mice. Further studies are needed to determine the mechanisms responsible for these complications, so that new therapies to prevent or diminish chemotherapy-related toxicities can be identified.
4-13
Extracellular vesicles are possible mediators of the liver-muscle axis in sarcopenia associated to liver disease
Laura Barberi1, Manuela Merli1, Simone di Cola1, Cristiana Porcu2, Stefano Fonte1, Lorenzo Ridola1 and Antonio Musarò2
1Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2DAHFMO, Unit of Histology and Medical Embryology, Sapienza University of Rome, Rome, Italy
Introduction: A loss of muscle mass and strength, referred as sarcopenia, is a condition highly prevalent in patients with chronic liver disease (CLD), in particular in alcoholic (ALD) patients. Although many factors contributing to skeletal muscle loss have been identified, mechanisms underlying sarcopenia in chronic liver diseases are still not completely understood as the mediators of the liver-muscle axis are not yet known.
As hepatic cells in pathological conditions, especially in ALD, release in circulation a large number of extracellular vesicles (EVs) and these have a key role in crosstalk between liver and other metabolic organs, including skeletal muscle, we aimed to investigate whether circulating EVs could induce muscle atrophy, mediating sarcopenia in liver disease.
Methods: C2C12 cell culture were exposed to EVs isolated from serum of a mouse model of ALD, obtained feeding mice for 2 months with Lieber-De Carli 5% (v/v) ethanol diet, and compared with cell culture exposed to EVs derived from control diet (CD)- mice. First, C2C12 cells were examined for ability to uptake circulating EVs, exposing them with PK26-stained serum EVs; then, C2C12 cell culture, treated with EVs isolated from ALD- and CD- mice, were analysed on 2nd and 6th day in differentiation medium for their capacity to fuse, differentiate and activate muscle synthetic or catabolic processes. Finally, to verify hepatic origin of circulating EVs, we isolated extracellular vesicles directly from liver tissue, investigating whether they affect C2C12 cell culture similarly to serum-derived EVs.
Results: We demonstrated, by confocal fluorescence analysis, that circulating EVs were efficiently internalized by C2C12 cells and myotubes. Moreover, ALD mice-derived EVs, in comparison with EVs isolated from CD mice, were able to cause in vitro muscle atrophy, inducing a decrease in muscle differentiation and in anabolic process accompanied by an increase in protein degradation: this was revealed by a reduced area and length of myotubes, downregulated expression of myogenin and myosin, decreased phosphorylation of Akt and mTOR, that are relevant markers of muscle protein synthesis, and upregulated mRNA expression of the muscle-specific atrophy-related markers MuRF1 and Atrogin1. Similar effects were observed with EVs isolated from liver, suggesting a hepatic origin of the circulating EVs contributing to muscle atrophy.
Conclusions: Circulating and liver tissue-derived EVs in CLD could induce muscle atrophy, suggesting their role as mediators of the liver-muscle axis in sarcopenia associated to liver disease.
4-14
Skeletal muscle transcriptional dysregulation of genes involved in senescence is associated with prognosis in severe heart failure
Eric Rullman and Alen Lovric and Michael Melin and Rodrigo Fernandez-Gonzalo and Thomas Gustafsson
Division of Clinical Physiology, Department of Laboratory Medicine, Karolinska, Institutet, and Unit of Clinical Physiology, Karolinska University Hospital Huddinge, Stockholm, Sweden
Introduction: The skeletal muscle hypothesis refers to a vicious cycle of successive deterioration of left ventricular function, skeletal muscle remodelling, and functional capacity in patients with heart failure. The mechanisms involved in these processes in skeletal muscle are still largely unclear.
Methods: In the present study, a coexpression network was constructed based on RNA sequencing of muscle samples from 66 patients with severe symptomatic heart failure with reduced ejection fraction (NYHA III-IV, left ventricular ejection fraction ≤ 30%). A transcriptomic network was defined in skeletal muscle and validated in two independent cohorts.
Results: The final network consists of 14 communities with transcripts involved in well-established biological processes in human skeletal muscle. Compared with age-matched controls and consistent with the known skeletal muscle phenotype in heart failure, lower expression was observed for communities related to mitochondrial beta-oxidation, extracellular matrix remodelling, oxidative phosphorylation, and contractile elements. Several earlier suggested external stimuli and biological processes in the skeletal hypothesis was shown to influence network expression in the skeletal muscle hypothesis, but to different degrees, suggesting differential importance. By correlating with clinical features and prognosis, three network communities (extracellular matrix remodelling, fatty acid beta-oxidation, and p53 signalling) were identified as plausible key processes, with the latter two also having prognostic potential shown by a significant, independent association with mortality.
Discussion: The strongest association to mortality was the p53-signalling community. This community was, in contrast to the other network communities, upregulated in HF patients compared with controls, and higher expression was associated with worse prognosis. The p53 signalling community was enriched for genes associated with senescence but not physical activity, bed rest, or cancer cachexia. This indicates that altered cell-cycle control at the skeletal muscle level is a process of prognostic relevance and that is not primarily influenced by physical inactivity, general deconditioning or negative energy balance. The significant enrichment of genes associated with cellular senescence, together with the strong correlation with mortality in the current study, seem to indicate that cell senescence in skeletal muscle is involved in the pathophysiology of HF and that this dysregulation is also of significant prognostic importance.
4-15
Cachexia, sarcopenia, and bone markers in patients with heart failure and hyperkalaemia: results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF)
Guglielmo Fibbi1, Tania Garfias-Veitl1,2, Mirela Vatić1,2, Ryosuke Sato1, Wolfram Doehner3,4,5, Stefan D. Anker3,5,6 and Stephan von Haehling1,2
1Department of Cardiology and Pneumology, University Medical Center Goettingen, Georg-August University, Goettingen, Germany;2German Center for Cardiovascular Research (DZHK), partner site Goettingen, Goettingen, Germany;3Berlin Institute of Health-Center for Regenerative Therapies (BCRT), Charité Universitaetsmedizin Berlin, Berlin, Germany;4Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany;5German Center for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany;6Division of Cardiology and Metabolism - Heart Failure, Cachexia & Sarcopenia, Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany
Introduction: Co-morbidities in heart failure (HF) have a major impact on prognosis. Hyperkalaemia (usually defined as serum potassium >5 mmol/L) is most prevalent in patients with diabetes mellitus, chronic kidney disease and in those taking inhibitors of the renin-angiotensin-aldosterone system. Patients with HF also present with cachexia, sarcopenia and have lower bone mineral density (BMD). The role of several regulators of bone remodelling, such as receptor activator of nuclear factor κB ligand (RANKL), osteoprotegerin and sclerostin in HF is not yet fully understood. We aimed to assess bone status, weight loss and muscle wasting in patients with HF and hyperkalaemia.
Methods: A total of 266 patients from SICA-HF with available baseline potassium measurements were retrospectively included in this analysis. Study subjects were divided into two groups according to potassium levels < or ≥5 mmol/L. Dual energy X-ray absorptiometry was used to evaluate BMD and body composition. Cachexia was defined as weight loss ≥5% over a 1-year period. Sarcopenia was defined as appendicular skeletal muscle mass index <7.26 kg/m2 in males and <5.45 kg/m2 in females.
Results: Patients with hyperkalaemia were more symptomatic (54 vs. 37% with NYHA class III-IV, P = 0.037) and were more likely to have diabetes (58 vs. 38%, P = 0.016) and an estimated glomerular filtration rate <60 mL/min/1.73 m2 (73 vs. 30%, P < 0.001). No differences could be seen regarding cachexia and sarcopenia between the two groups. Interestingly, patients with HF and hyperkalaemia had increased levels of osteoprotegerin (5.8 vs. 4.7 pmol/L, P = 0.009) and sclerostin (92 vs. 74 pmol/L P = 0.022), lower levels of RANKL (5920 vs. 20 200 pg/mL, P = 0.006) and higher total body BMD (1.25 ± 0.11 vs. 1.21 ± 0.12 g/cm2, P = 0.027) and Z-score (the number of standard deviations away from the mean total body BMD of a healthy person of same age and sex, 0.79 ± 1.41 vs. 0.36 ± 1.27, P = 0.045). Using univariate logistic regression, osteoprotegerin (OR 1.218 95% CI [1.036–1.433], P = 0.017), sclerostin (OR 1.014 95% CI [1.003–1.025], P = 0.014), RANKL (OR 0.6 95% CI [0.388–0.928], P = 0.022) and total body BMD (OR 1.455 95% CI [1.039–2.036], P = 0.029) were all associated with hyperkalaemia. In the multivariate model, osteoprotegerin and total body BMD remained as independent predictors of hyperkalaemia (adjusted OR 1.305, 95% CI [1.058–1.610], P = 0.013; adjusted OR 1.792, 95% CI [1.105–2.905], P = 0.018, respectively).
Conclusions: We found an association between higher total body BMD and hyperkalaemia in patients with HF. More data on the link between bone status and potassium levels are needed.
4-18
Metabolic remodelling during skeletal muscle hypertrophy: role of glycolysis-derived intermediates in anabolic pathways
Philipp Baumert1, Sakari Mäntyselkä†, 2, Martin Schönfelder†, 1, Marie Heiber1, Anandini Swaminathan3, Petras Minderis3, Mantas Dirmontas4, Karin Kleigrewe5, Chen Meng5, Michael Gigl5, Tomas Venckunas3, Hans Degens3,6, Aivaras Ratkevicius3,4, Juha J. Hulmi2 and Henning Wackerhage1
1Department of Sport and Health Sciences, Technical University of Munich, Munich, Germany;2Faculty of Sport and Health Sciences, Neuromuscular Research Center, University of Jyväskylä, Jyväskylä, Finland;3Lithuanian Sports University, Institute of Sport Science and Innovations, Kaunas, Lithuania;4Department of Health Promotion and Rehabilitation, Lithuanian Sports University, Kaunas, Lithuania;5Bavarian Center for Biomolecular Mass Spectrometry, Technical University of Munich, Munich, Germany;6Department of Life Sciences, Manchester Metropolitan University, Manchester, UK
†These authors contributed equally to this work
Introduction: Proliferating cancer cells shift their metabolism towards glycolysis even in the presence of oxygen to generate glycolytic intermediates as substrates for anabolic reactions. However, whether and how a controlled growing muscle reprograms its metabolism in a similar manner is poorly researched. We hypothesize that a similar metabolic remodelling occurs during skeletal muscle hypertrophy.
Methods: We used mass spectrometry in hypertrophying muscles both in C2C12 muscle cells in vitro and plantaris mice muscle in vivo and assessed metabolomic changes and the incorporation of stable isotope [U-13C6]glucose tracer. We performed enzyme inhibition for further mechanistic analysis and a systematic review to align any changes in metabolomics during muscle growth with previous findings.
Results: The metabolomics analysis in C2C12 muscle cells revealed altered metabolite concentrations in anabolic pathways such as in the pentose phosphate (ribose-5-phosphate/ribulose-5-phosphate: +40%; P = 0.01) and serine synthesis pathway (serine: −36.8%; P = 0.009) to build up biomass, as well as in the hexosamine biosynthetic pathway that serves as a basis for the post-translational so-called O-linked glycosylation modification. L-carnosine and UDP-N-acetylgalactosamine metabolites were decreased and increased in both hypertrophied muscles in mice in vivo (−25.9% and +252%) as well as in C2C12 myotubes in vitro (−44.1% and +75.6%), respectively (all P < 0.042). The systematic review showed that 12 of 20 identified metabolites associated with muscle hypertrophy were directly related to glycolysis and to its linked anabolic pathways. We demonstrated that labelled carbon from [U-13C6]glucose is increasingly incorporated by ~13% (P = 0.001) into the non-essential amino acids in hypertrophying myotubes. The inhibition of the key enzyme phosphoglycerate dehydrogenase (Phgdh) supressed muscle protein synthesis by 74.9% (P = 0.008) highlighting the importance of the serine pathway for maintaining muscle size.
Conclusions: Understanding the mechanisms that regulates skeletal muscle mass will help in developing effective treatments against muscle weakness. Our results provide evidence for metabolic rewiring of glycolytic intermediates into anabolic pathways during muscle growth, such as in the serine synthesis and hexosamine biosynthetic pathways.
4-19
Vitamin D signalling plays an inhibitory role in intramuscular adipogenesis of FAPs
Tohru Hosoyama1, Minako Kawai-Takaishi1, Hiroki Iida1, Tsuyoshi Watanabe2, Yasumoto Matsui2, Akiyoshi Uezumi3 and Ken Watanabe1
1Department of Musculoskeletal Disease, National Center for Geriatrics and Gerontology, Fukuoka, Japan;2Center for Frailty and Locomotive Syndrome, National Center for Geriatrics and Gerontology, Fukuoka, Japan;3Medical Institute of Bioregulation, Kyushu University, Fukuoka, Japan
Introduction: Recent studies indicate an importance of muscle quality in Sarcopenia pathophysiology in addition to muscle quantity. Intramuscular adipose tissue (IMAT), which is known to be originated from fibro/adipogenic progenitors (FAPs) in adult skeletal muscle, is one of the key factors affecting muscle quality in elderlies, suggesting that to control IMAT formation is promising therapeutics for Sarcopenia. However, the molecular mechanism underlying IMAT formation in elderlies has not been clarified so far. We recently found that vitamin D receptor (VDR) is highly expressed in FAPs in comparison to myogenic cells, indicating a potential role of vitamin D signalling in FAPs. In this study, we aimed to clarify the role of vitamin D signalling in FAP's kinetics particularly focusing on adipogenesis.
Methods: FAPs isolated from mouse skeletal muscles were applied to adipogenic differentiation condition with or without vitamin D (1α,25(OH)2D3), and then adipogenicity was evaluated by expression of adipogenic markers. For in vivo analysis, tamoxifen-inducible FAP-specific Vdr-deficient (VdrFAPcKO) mice were newly developed to investigate whether lack of vitamin D signalling in FAPs was involved in IMAT formation.
Results: Vitamin D treatment almost completely inhibited adipogenesis of FAPs through direct transcriptional control of adipogenic genes, whereas Vdr-deficient FAPs differentiated into adipocytes in the presence of vitamin D. In consistent with in vitro studies, VdrFAPcKO mice exhibited fat deposition.
4-22
Inhibiting serine synthesis pathway by PHGDH inhibition reprograms skeletal muscle cell metabolism and impairs anabolic processes
Sakari Mäntyselkä1, Kalle Kolari1, Philipp Baumert2, Laura Ylä-Outinen1, Lauri Kuikka3, Suvi Lahtonen4, Perttu Permi4,5,6, Henning Wackerhage2, Elina Kalenius5, Riikka Kivelä1,7,8 and Juha J. Hulmi1
1Faculty of Sport and Health Sciences, NeuroMuscular Research Center, University of Jyväskylä, Jyväskylä, Finland;2Department for Sport and Health Sciences, Technical University of Munich, Munich, Germany;3Central Finland Health Care District Hospital District, Jyväskylä, Finland;4Department of Biological and Environmental Science, University of Jyväskylä, Jyväskylä, Finland;5Department of Chemistry, University of Jyväskylä, Jyväskylä, Finland;6Institute of Biotechnology, Helsinki Institute of Life Science, University of Helsinki, Helsinki, Finland;7Stem Cells and Metabolism Research Program, Research Programs Unit, Faculty of Medicine, University of Helsinki, Helsinki, Finland;8Wihuri Research Institute, Helsinki, Finland
Introduction: Skeletal muscle mass maintenance and growth require amino acids, nucleotides, and lipids for macromolecule and cell organelle synthesis. Some of these essential building blocks can be de novo synthesized from intermediates of the glycolysis in serine synthesis and pentose phosphate pathways. However, the knowledge of the importance of these metabolic pathways in muscle size regulation is poorly understood. The aim of this study was to identify enzymes from these metabolic pathways that limit myotube size, growth, and proliferation in cultured muscle cells.
Methods: We first tested the effect of inhibition of key enzymes of glycolysis, pentose phosphate pathway, and serine synthesis pathway on muscle cell protein synthesis. This small-scale screen led us to focus on studying the importance and mechanisms of the serine synthesis pathway using two different inhibitors of an essential enzyme phosphoglycerate dehydrogenase (PHGDH). We investigated murine C2C12 and human primary skeletal muscle cells by using a wide variety of analysis methods including EdU and radiolabelling, western blotting, confocal microscopy, qPCR, and nuclear magnetic resonance (NMR) spectroscopy and liquid chromatography-mass spectrometry (LC–MS) metabolomics. In addition, we screened several potential exogenous compounds that could reverse the effects of PHGDH inhibition.
Results: We found that the inhibition of the serine synthesis pathway through PHGDH inhibition decreased protein synthesis in a dose-responsive manner and decreased myoblast proliferation and myotube size without affecting cell viability. The inhibition of PHGDH decreased glucose-derived carbon incorporation into proteins, RNA, and lipids in myotubes and myoblasts. Further, we found that PHGDH inhibition accelerated glycolysis and altered amino acid, nucleotide, and lipid metabolism without a major effect on mitochondrial parameters. In addition, PHGDH inhibition increased adenosine monophosphate (AMP) content and AMPK signalling, and unfolded protein response accompanied by decreased mTORC1 signalling in myotubes, which was associated with decreased muscle protein synthesis. Lastly, we found that antioxidant/redox modulator N-acetylcysteine supplementation partially rescued the decreased protein synthesis and mTORC1 signalling induced by PHGDH inhibition.
Conclusions: The results suggest that the serine synthesis pathway and especially its first enzyme PHGDH is essential for the maintenance of biomass in skeletal muscle cells and that this is connected to mTORC1 signalling and changes in oxidative stress and redox balance. In further studies, the role of the serine synthesis pathway and its mechanisms in vivo should be studied in sarcopenia and muscle-wasting diseases.
4-23
Antisense oligonucleotides as a potential therapy in muscle wasting disorders
Andrea García-Rey1,2,3, Estefanía Cerro-Herreros1,2,3, Mouli Chakraborty1, Nuria Barquero1, Isabel Campillo1, Sheila Soriano Santafé1, Judit Núñez-Manchón4, Neia Naldaiz-Gastesi5, Marc Carrascosa-Sàez3, Irene González-Martínez1,2, Adolfo López de Munain5, Mònica Suelves4, Gisela Nogales-Gadea4, Rubén Artero2,3 and Beatriz Llamusí1
1ARTHEx Biotech. Parque Científico de la Universidad de Valencia, Paterna, Valencia, Spain;2University Research Institute for Biotechnology and Biomedicine (BIOTECMED), Universidad de Valencia, Valencia, Spain;3Translational Genomics Group, INCLIVA Biomedical Research Institute, Valencia, Spain, Valencia, Spain;4Neuromuscular and Neuropediatric Research Group, Institut d'Investigació en Ciències de la Salut Germans Trias i Pujol (IGTP), Campus Can Ruti, Universitat Autònoma de Barcelona, Badalona, Spain;5Neuromuscular Diseases Group, Neurosciences Area, Biodonostia Health Research Institute, Donostia/San Sebastián, Spain
Introduction: Muscle atrophy, or muscle wasting, is characterized by a significant shortening or thinning of muscle fibres and loss of overall muscle mass. It is a common symptom of several disorders. It can appear due to illnesses such as cancer, cardiac dysfunction, sarcopenia, or genetic muscular dystrophies. The role of microRNAs (miRNAs) in skeletal muscle is under study. MyomiRs, muscle-rich miRNAs, are essential for proper myocyte differentiation, protein turnover and skeletal muscle development and differentiation. Specifically, miR-23b is a myomiR belonging to the miR-23b/27b/24-1 cluster and the effects of its misregulation has been studied in myotonic dystrophy type I (DM1), a neuromuscular disorder characterized by loss of strength, muscle wastage and atrophy. Arthex Biotech is developing an antimiR (ATX-01) to inhibit the activity of miR-23b as treatment of DM1 patients. This ASO has been chemically modified to increase its specificity and bio-distribution to muscle. ATX-01 therapeutic activity on muscle wasting-related phenotypes has been tested in human DM1 myotubes and in adult DM1 mouse model HSALR.
Methods: Primary and immortalized myotubes from DM1 patients were treated with ATX-01 at 50 nM. Rescue of the differentiation defects that characterized these cellular models, was determined by measuring area of fibres, their fusion index, and quantifying the splicing pattern of BIN1, which has been linked to muscle weakness phenotype in DM1 patients. HSALR mice were injected intravenously with ATX-01 at 12 mg/kg and sacrificed at day 14. The therapeutic potential of ATX-01 in skeletal muscle was measured by grip strength, body weight and mass muscles of animals. Myopathy was determined by quantifying central nuclei in muscle fibres and the amount of compound in muscles were determined by ELISA.
Results: Inhibition of miR-23b with ATX-01 increases the area and fusion index of myotubes after differentiation. Treated HSALR mice showed an increase in muscle mass and strength and decreased central nuclei in muscle fibres suggesting an improvement of muscle structure. Treatment with ATX-01 rescues the alternative splicing of BIN1 in both mice and cells. Finally, the quantification of ATX-01 in muscle confirms that our delivery strategy importantly increase the amount of antimiRs in muscle.
Conclusions: ATX-01 is a lead compound for DM1, able to improve muscle wasting phenotypes in vitro and in vivo models. The PK/Pd data obtained with ATX-01 in the in vivo model supports its further development into clinics and validates our delivery strategy to target muscle tissue with antimir molecules.
4-24
Sex-specific molecular features of clear cell renal cell carcinoma are associated with muscle loss
Robab Hassanvand Jamadi1,2, Cynthia Stretch2, Victoria Armstrong2, Mathias T. Bathe2, Iphigenia Tzameli3, Evanthia Pashos3, Junjie Li3, Olivier Bezy4, Vickie E. Baracos5 and Oliver F. Bathe1,2,6
1Arnie Charbonneau Cancer Research Institute, Cumming School of Medicine, University of Calgary, Calgary, Canada;2Department of Medical Sciences, University of Calgary, Calgary, Canada;3Internal Medicine Research Unit, Pfizer Worldwide Research, Development & Medical, Cambridge, MA, USA;4Cellarity Inc., Somerville, MA, USA;5Department of Oncology, University of Alberta, Edmonton, Canada;6Departments of Surgery and Oncology, University of Calgary, Calgary, Canada
Introduction. Renal cell carcinoma (RCC) is the most common type of kidney cancer. Clear cell renal cell carcinoma (ccRCC) is the most common variant, with about 100 000 deaths annually. In RCC, low muscle mass (sarcopenia), with a prevalence in about 40–60% of patients, is associated with shorter survival. However, the underlying molecular mechanism is unknown. The hypothesis is that the changes in the molecular features of the tumour drive the phenotype. The aim is to characterize these features.
Methods: RNA-Seq and clinical data for ccRCC patients annotated by The Cancer Genome Atlas (TCGA; N = 539) and the Clinical Proteomic Tumour Analysis Consortium (CPTAC; N = 185) were accessed. Preoperative CT scans for 200 of the TCGA cases were accessed for body composition analysis from The Cancer Imaging Archive (TCIA). Muscularity was assessed at the level of L3 using SliceOmatic. Because height information was unavailable, sarcopenia was defined as the lowest tertile of skeletal muscle area. Sarcopenia-associated genes were identified by comparing gene expressions in the highest and lowest tertile. Due to sexual dimorphism in the molecular features of RCC, differentially expressed genes (DEGs) associated with sarcopenia were separately identified in males and females. Since sarcopenia is associated with advanced stages of ccRCC, DEGs associated with advanced T and M stages were excluded.
Results: Sarcopenia was associated with worse survival (HR = 2.546; P-value < 0.0001). In males, 231 DEGs comprised the molecular signature of the sarcopenia-associated variant of ccRCC. In females, 60 sarcopenia-specific DEGs were identified. Using these genes, classifiers were generated for the male and female sarcopenia-associated variants. As in patients with CT scans, in TCGA patients without a CT scan, and in CPTAC patients, survivals were significantly worse in individuals with the sarcopenia-associated variant. We performed gene set enrichment analysis (GSEA) to determine the biological features of sarcopenia-associated variants. In males, there was a positive enrichment of epithelial-mesenchymal transition (EMT), proliferative pathways, inflammatory pathways, and glycosaminoglycan metabolism. In females, there was an enrichment of TGF-β signalling, EMT, bile acid metabolism, and steroid metabolism. Interestingly, there was a negative enrichment in the inflammatory gene sets in females.
Conclusions: Sarcopenia is associated with worse survival in ccRCC. We have identified molecular features in ccRCC that are associated with sarcopenia. There is sexual dimorphism in these features. Future work will focus on other RCC subtypes to see if the same features appear and how they are related to sarcopenia.
4-25
Influence of IGF-I serum concentration on muscular regeneration capacity in patients with sarcopenia
Michael Drey1, Stefanie Jarmusch1, Lisa Baber1, Martin Bidlingmaier4, Fabian Hofmeister1, Stefan Hintze2, Stefan Mehaffey3, Peter Meinke2, Carl Neuerburg3 and Benedikt Schoser2
1Department of Medicine IV, Geriatrics, University Hospital of LMU, Munich, Germany;2Friedrich-Baur-Institute, Department of Neurology, University Hospital of LMU, Munich, Germany;3Department of General-, Trauma- and Reconstructive Surgery, University Hospital of LMU, Munich, Germany;4Department of Medicine IV, Endocrinological Laboratory, University Hospital of LMU, Munich, Germany
Introduction: Previous research has described a neuroprotective effect of IGF-I, supporting neuronal survival, axon growth and proliferation of muscle cells. Therefore, the association between IGF-I concentration, muscle histology and electrophysiological markers in a cohort of patients with sarcopenia dares investigation.
Methods: Measurement of serum concentrations of IGF-I and binding partners, electromyographic measurements with the MUNIX (Motor Unit Number Index) method and muscle biopsies were performed in 31 patients with acute hip fracture older age 60 years. Molecular markers for denervation (neural cell adhesion molecule NCAM) and proliferation markers (Ki67) were assessed by immunofluorescence staining of muscle biopsy tissue. Skeletal muscle mass by bioelectrical impedance analysis and hand-grip strength were measured to assess sarcopenia status according to EWGSOP2 criteria.
Results: Thirty-one patients (20 women) with a mean age of 80.6 ± 7.4 years were included. Concentrations of IGF-I and its binding partners were significantly associated with sarcopenia (ß = − 0.360; P = 0.047) and MUNIX (ß = 0.512; P = 0.005). Further, expression of NCAM (ß = 0.380; P = 0.039) and Ki67 (ß = 0.424; P = 0.022) showed significant associations to IGF-I concentrations.
Conclusions: The findings suggest a pathogenetic role of IGF-I in sarcopenia based on muscle denervation.
4-26
Dynapenic abdominal obesity as a risk factor for the incidence of metabolic syndrome in individual 50 years of age or older: evidence from the English Longitudinal Study of Aging
Paula Camila Ramírez1,2, Roberta de Oliveira Máximo1, Dayane Capra de Oliveira1, Aline Fernanda de Souza1, Mariane Marques Luiz1, Maicon Luís Bicigo Delinocente3, Andrew Steptoe4, Cesar de Oliveira4 and Tiago da Silva Alexandre1,3,4,5
1Programa de Pós-Graduação em Fisioterapia, Universidade Federal de São Carlos, São Carlos, Brazil;2Escuela de Fisioterapia, Universidad Industrial de Santander, Bucaramanga, Colombia;3Programa de Pós-Graduação em Gerontologia, Universidade Federal de São Carlos, São Carlos, Brazil;4Department of Epidemiology & Public Health, University College London, London, UK;5Departamento de Gerontologia, Universidade Federal de São Carlos, São Carlos, Brazil
Introduction: The reduction in neuromuscular strength (dynapenia) can coexist with obesity among older people. Adipose tissue and muscle are endocrine organs, and the co-occurrence of the two conditions in the same individual may increase the likelihood of the incidence of metabolic syndrome (MetS). The objective was to analyse whether dynapenic abdominal obesity is a risk factor for the incidence of MetS in individuals 50 years of age or older.
Methods: A longitudinal study was conducted with an 8-year follow-up involving 3952 individuals from the English Longitudinal Study of Aging (ELSA) who were free of MetS at baseline. Dynapenic abdominal obesity was defined based on waist circumference (> 102 cm for men and > 88 cm for women) and grip strength (<26 kg for men and < 16 kg for women). The participants were classified as non-dynapenic/non-abdominal obesity (ND/NAO), non-dynapenic/abdominal obesity (ND/AO), dynapenic/non-abdominal obesity (D/NAO) and dynapenic/abdominal obesity(D/AO). The outcome was the incidence of MetS, the development of three or more components of MetS during follow-up: hypertriglyceridemia, hyperglycaemia, low HDL cholesterol, arterial hypertension, and obesity. Poisson regression models were run and controlled for sociodemographic and behavioural variables.
Results: The adjusted model demonstrated that although abdominal obesity was a risk factor for the incidence of MetS (IRR: 2.73; 95% CI: 2.28–3.27), the effect size of the association was greater in AO/D individuals (IRR: 4.09; 95% CI: 2.51–6.66).
Conclusions: Dynapenic abdominal obesity increases the risk of the incidence of MetS with a higher effect size compared to obesity alone. The understanding of this synergic action could guide specific clinical strategies in order to prevent cardiovascular disease, disability and death.
Type II myofibre atrophy is not underpinned by deficits in acute anabolic signalling after resistance exercise and amino acid intake in healthy, lean older adults
Oscar Horwath1, Sebastian Edman2, Henrik Strömlind3, Andrew Philp4 and William Apró3
1Department of Physiology, Nutrition and Biomechanics, The Swedish School of Sport and Health Sciences, Stockholm, Sweden;2Karolinska Institute, Stockholm, Sweden;3The Swedish School of Sport and Health Sciences, Stockholm, Sweden;4Centenary Institute, Sydney, Australia
Introduction: Aging is associated with progressive loss of muscle mass and function. Muscle mass below a certain threshold (sarcopenia) represents a risk-factor for several adverse outcomes, i.e., disability, reduced life quality and mortality. Muscle loss across the lifespan is however not equally distributed among different myofibre types, with specific atrophy of type II myofibres accounting for most of the atrophy. Leaving the muscle with an impaired capacity for fast contractions, this represents an important contributing factor in the development of muscle weakness and may predispose older adults to falls and fall-related injuries. Several mechanisms have been put forward as causal for sarcopenia, one of which is diminished responsiveness to anabolic cues, i.e., exercise and amino acids. Here we investigated whether ‘anabolic resistance’ specific to the type II myofibres may explain their selective atrophy during aging.
Methods: Ten young (22 ± 1 years) and 10 older (70 ± 1 years) healthy, lean men performed 10 sets of unilateral resistance exercise (RE). Muscle biopsies were obtained before and immediately after RE, and 60 and 180 min after intake of essential amino acids (EAA) in both the rested and the exercised leg. Myofibre characteristics were determined on muscle-cross sections using immunohistochemistry. Individual myofibres were dissected from freeze-dried muscle samples, fibre typed using the THRIFTY protocol, and pooled together according to their myofibre type. Phosphorylation of proteins downstream of mTORC1 were measured using immunoblotting. Statistics were performed using mixed-effect analysis with Bonferroni correction.
Results: At baseline, older adults had fewer and smaller type II myofibres and less satellite cells and capillaries associated with type II myofibres compared to young adults (P < 0.05). In the rested leg, EAA induced phosphorylation of S6K1Thr389 and 4EBP1Ser65 similarly in both myofibre types (P < 0.05), an effect that was greater in old than young adults (P < 0.05). In the exercised leg, phosphorylation of S6K1Thr389 and 4EBP1Ser65 was increased compared to baseline in both myofibre types (P < 0.05), however, this effect was similar in young and older adults. Phosphorylation of 4EBP1Ser65 was consistently higher in type I than type II myofibres across conditions and time points (P < 0.05).
Conclusions: Type II myofibre atrophy during aging is not associated with diminished mTORC1-signalling in healthy, lean older adults in response to high-dose EAA and high-volume RE. Other factors such as decreased satellite cell content and/or impaired blood flow to these myofibres may instead contribute to this selective atrophy.
4-28
Autophagosomes and protein aggregates accumulation in the skeletal muscle of septic patients, a pilot study
Charlotte Schonhart1, Håkan Rundqvist2, Olav Rooyackers1 and Nicolas Tardif1,3
1Division of Anesthesiology and Intensive Care, CLINTEC, Karolinska Institute, Stockholm, Sweden;2Division of Clinical Physiology, Karolinska Institute, Stockholm, Sweden;3Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden
Introduction: We have previously shown, in a model of human primary myotubes incubated with serum from intensive care patients, that serum from only 15% of the patients were able to block autophagy (1). This blockade was associated with an accumulation of autophagosomes, indicating a defect in the autophagy fusion step (1). Like neuronal cells, skeletal muscle is a postmitotic tissue that is highly dependent on autophagy. Blockade of autophagy has been well studied in neurodegenerative diseases and is associated with the accumulation of protein aggregates. In this pilot study, we aimed to investigate whether accumulation of autophagosomes and protein aggregates can be detected in skeletal muscle from critically ill septic patients treated in the ICU.Methods: We analysed cryosections from the vastus lateralis of 15 septic ICU patients and 8 age-matched control patients from a previous study (2). These cryosections were processed to measure colocalization of LC3 and p62 by proximal ligation assay (PLA) staining as a measure of autophagosomal vesicles. In addition, we measured the accumulation of phosphorylated Tau proteins by immunofluorescent staining.
Results: As expected, we observed a significantly lower fibre size area in the septic ICU patients compared to the control group (3530 ± 672 vs. 2703 ± 756 μm2; Control vs. ICU, P = 0.0085). The septic ICU patients had a higher fraction of their fibres covered by autophagosomes in comparison with the controls (0.04 ± 0.01% vs. 0.07 ± 0.02%; Control vs. ICU, P = 0.0144). We did not detect a higher number of phosphorylated tau per fibre between control and septic ICU patients. However, as with autophagosomes, the percentage of fibre surface covered by phosphorylated tau aggregates was significantly higher in the septic ICU group (0.20 ± 0.17% vs. 0.44 ± 0.33%; Control vs. ICU, P = 0.046).
Conclusions: In this pilot study, we observed a higher accumulation of autophagosomes, replicating our previous in vitro observations. We also observed a higher accumulation of phosphorylated TAU, indicating a defect in proteostasis in skeletal muscle of septic ICU patients. Moreover, phosphorylated TAU and autophagosomes were already present in muscle of some of the age-matched controls, indicating a potential age-related impairment of autophagy and pathways associated with proteostasis.
1. Tardif, N, Polia, F, Tjäder, I, Gustafsson, T, Rooyackers, O. Autophagy flux in critical illness, a translational approach. Sci Rep2019; 9:10762.
2. Tjäder, I, Klaude, M, Hssain, AA, Guillet, C, Nennesmo, I, Wernerman, J, et al. Variability in skeletal muscle protein synthesis rates in critically ill patients. Nutrients2022; 14:3733.
4-30
Validation of a bedside ergometer dedicated to longitudinal evaluation of neuromuscular function in intensive care unit patients
Djahid Kennouche1, Éric Luneau1, Arthur Pflieger1, Robin Souron1,2, Nicolas Thierry3, Thomas Lapole1, Julien Gondin4, Guillaume Y. Millet1,5 and Jérôme Morel1,3
1Laboratoire Interuniversitaire de Biologie de la Motricité, Université Jean Monnet Saint-Etienne, Lyon 1, Université Savoie Mont-Blanc, Saint-Etienne, France;2Motricity, Interaction, Performance Laboratory, Université de Nantes, Nantes, France;3Département Anesthésie Réanimation, Centre Hospitalier Universitaire de Saint-Etienne, Saint-Etienne, France;4Unité de Physiopathologie et Génétique du Neurone et du Muscle, Université de Lyon, CNRS 5261, INSERM U1315, Institut NeuroMyoGène (INMG), Lyon, France;5Institut Universitaire de France (IUF), Paris, France
*These authors equally contributed.
Introduction: Around 30% of intensive care unit (ICU) patients develop ICU-acquired weakness (ICUAW). To date, ICUAW diagnosis is delayed because it relies on the Medical Research Council score based on voluntary force evaluation which can only been performed in awaked patients. An early diagnosis of ICUAW using evoked force measurements could be a promising approach.
Methods: An innovative bedside adjustable ergometer, encompassing a force transducer on a moveable and gradable platform to fit the patient's morphology, was designed for the study (Figure 1).
Thirty-seven sedated patients with an expected duration of mechanical ventilation ≥ 3 day (SOFA: 8 ± 3; SAPSII: 54 ± 15) were evaluated in the early phase (i.e. at day 2–4), the late phase (i.e. > day 4) of ICU admission and at awakening. For each evaluation, measurements were initially performed (H0) and then repeated 1 h (H1) later by a first experienced investigator. For the early evaluation, a second novice investigator completed the protocol 2 h (H2) after the initial measurements). Force was recorded in response to stimulation of the femoral nerve using single (Tw) and paired (Db100) electrical and magnetic stimulations (ES and MS, respectively) (Figure 2). Reliability was assessed using the intra-class correlation coefficients (ICC) and coefficients of variation (CV).
Results: Reliability measurements of electrically-evoked force production was comparable whatever phase, investigator or number of stimuli (Table 1). Out of the 37 patients included, only 2 were tested during the 3 phases. No mechanical response was observed in response to MS in 6 patients. This is likely due to high body fat and/or generalized gross oedema.
Conclusions: The present study shows that measuring force at bedside in sedated patients using an innovative ergometer provided good-to-excellent reliability whatever the timing of testing or the experience of the investigator. These promising results should allow reliable measurements to track deconditioning and quantify early neuromuscular function alterations during ICU stay. This should provide early, quantitative and longitudinal force measurements in sedated patients that would be of utmost importance to refine the diagnosis of ICUAW.
4-31
Electrical stimulation (ES) exhibits a local and systemic restoring effect on muscular disarrangements associated with critical illness myopathy (CIM)
Ya Wen1, Xiang Zhang1, Nicola Cacciani1, Meishan Li1, Yvette Hedström1 and Lars Larsson1,2
1Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden;2Viron Molecular Medicine Institute, Boston, MA, USA
Introduction: Critical illness myopathy (CIM) negatively influences the prognosis, morbidity, mortality, and health care costs in intensive care unit (ICU) patients. CIM has prevalence of 30% in the general ICU population and 100% in some ICU subpopulations, but there is currently no effective therapy available targeting the pathogenesis mechanism of CIM. Electrical stimulation (ES) has emerged as a safe and efficient substitute for physical exercise and has been applied to clinical settings to mitigate muscle wasting in patients with limited mobility and prolonged bed rest. In the present study, we aim to explore the therapeutic effect of ES against CIM.
Methods: A unique experimental ICU (ExICU) allowing for the study of CIM pathophysiology was employed in the present study. ExICU rats were exposed to 8-day ICU conditions (i.e., deep sedation, postsynaptic neuromuscular blockade, and mechanical ventilation) with or without unilateral direct ES of the soleus muscle. RNAseq-based transcriptomics (soleus) and Olink-based plasma proteomics were conducted to evaluate the therapeutic effects of ES in animals exposed to the ICU conditions.
Results: Transcriptomics analysis demonstrated dramatic muscular disarrangements in the soleus muscle, some of which were partially restored by ES, such as genes involved in ‘muscle system process’, ‘fatty acid metabolic process’, ‘extracellular matrix organization’, etc. An unexpected observation was a similar restoring effect in the unstimulated contralateral soleus muscle, referred to as the crossover effect. Based on plasma proteomic analysis, we identified several differentially expressed proteins in plasma after 8-day ICU conditions (Erbb4, Notch3, Il17a, etc.) and ES intervention (Yes1, Tgfb1, Ccl3, etc.), respectively. These circulating factors are forwarded as playing a significant role in CIM pathophysiology and in the crossover effect.
Conclusions: Results from this study demonstrate dramatic muscular disarrangements and plasma protein profile alterations of importance for our understanding of CIM pathophysiology. A local and systemic restoring effect was observed of ES which has the potentials to maintain muscle function in immobilized and unconscious mechanically ventilated ICU patients. Further, the circulating factors identified in plasma after 8-day ICU conditions and ES intervention may provide important biomarkers for CIM and potential targets for pharmacological interventions against CIM.
Keywords: critical illness myopathy; electrical stimulation intervention; local and systemic restoring effect; soleus muscle; multiomics approach.
4-32
The effect of awakening on leg muscle size in patients with critical illness who received early functional rehabilitation
Thomas C. Rollinson1,6,7, Bronwen Connolly2,3,4,6, Linda Denehy, Graham Hepworth5 and David J. Berlowitz1,6,7 and Sue Berney1,6,7
1Department of Physiotherapy, Division of Allied Health, Austin Health, Melbourne, Australia;2Wellcome-Wolfson Institute for Experimental Medicine, Queen's University Belfast, Belfast, UK;3Lane Fox Clinical Respiratory Physiology Research Centre, Guy's and St. Thomas' NHS Foundation Trust, London, UK;4Centre for Human and Applied Physiological Sciences, King's College London, London, UK;5Statistical Consulting Centre, The University of Melbourne, Melbourne, Australia;6Department of Physiotherapy, The University of Melbourne, Melbourne, Australia;7Institute for Breathing and Sleep, Melbourne, Australia
Introduction: Time to awakening is a variable time point for patients who are intubated and ventilated in the ICU. It remains a confounder to the implementation of active early mobilization in clinical trials. Non-volitional exercise such as neuromuscular electrical stimulation may address this gap however it is unknown whether this treatment effects muscle wasting prior to awakening. Therefore, we aimed to examine the effect of awakening on the rate of change of rectus femoris cross-sectional area in patients with critical illness receiving early functional electrical stimulation-cycling, recumbent cycling, or usual care.
Methods: This was an exploratory analysis of data not previously reported from a randomized controlled trial. Adults with critical illness who required >48 h of mechanical ventilation, diagnosed with sepsis and/or systemic inflammatory response syndrome, expected to remain in intensive care for more than 4 days and safe to commence exercise were included. The intervention group received up to 60 min of recumbent cycle ergometry with functional electrical stimulation (FES) in one leg, the other receiving cycling alone. The control group received usual care rehabilitation. The primary outcome was rate of change in rectus femoris cross-sectional area (mm2/day) measured using skeletal muscle ultrasound in the intensive care unit prior to awakening, post awakening and post intensive care unit discharge.
Results: Seventy-two participants were included (35 intervention; 37 control). Rectus femoris cross-sectional area declined prior to awakening (−14 mm2/day [95% CI, −19 to −9]), increased post-awakening (6 mm2/day [95% CI, 0 to 12]) with mean difference 20 mm2/day [95% CI, 12 to 29]; P < 0.0001) and decreased post intensive care unit discharge (−4 mm2/day [95% CI, −10 to 1]. There was no statistically significant difference in rate of change of muscle size between groups (P = 0.864).
Conclusions: Awakening is an important and under-explored time point in recovery from critical illness when the rate of muscle decline could be arrested. The rate of muscle decline was not modified with early recumbent cycling, including FES-cycling, compared with usual care alone. These results indicate that timing of awakening may be pivotal in arresting muscle loss during critical illness and challenges the effectiveness of rehabilitation interventions in sedated patients.
4-34
Long Covid: a combination of self-reported symptoms, lower muscle function and disrupted inflammation
Gabriela Salim de Castro1, Leonardo dos Reis Gama2, Alexandre Ferreira Ramos2,3, Guilherme Gatti da Silva1, Alessandro Rodrigo Belon1, Marta Imamura4, José Pinhata Otoch5, Linamara Battistella6, Geraldo Busatto7,8 and Marilia Seelaender1
1Cancer Metabolism Research Group, Departamento de Cirurgia e LIM 26-HC Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil;2Departamento de Radiologia e Oncologia & Instituto do Câncer do Estado de Sao Paulo, Universidade de Sao Paulo, Sao Paulo, Brazil;3Escola de Artes, Ciências e Humanidades, Universidade de Sao Paulo, Sao Paulo, Brazil;4Departamento de Medicina Legal, Bioetica, Medicina do Trabalho e Medicina Fisica e Reabilitacao, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, Brazil;5Universidade de Sao Paulo Hospital Universitario, Sao Paulo, Brazil;6Instituto de Medicina Fisica e Reabilitacao, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, Brazil;7Diretoria Executiva dos LIMs, Faculdade de Medicina da Universidade de São Paulo, Sao Paulo, Brazil;8Departamento e Instituto de Psiquiatria, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo HCFMUSP, São Paulo, Brasil
Introduction: Long COVID may be defined as a condition in which persistent alterations occur after SARS-CoV 2 infection not explicated by other diagnosis. Fatigue appears as the most frequently symptom. Increased and sustained systemic inflammation seems to be involved in the pathogenesis of Long COVID. Objectives: We evaluated several circulating cytokines together with physical performance tests in 228 participants, who were hospitalized in 2020 due to acute COVID-19 and came back for a follow-up assessment 5–12 months after hospitalization.
Methods: The participants were separated in three groups: a Control group (n = 77), who reported low frequency of self-reported symptoms in the follow-up assessment; a Self-Reported Symptoms group (SR, n = 97), in which participants presented several symptoms, such as fatigue and muscle weakness; and the Self-Reported Symptoms with Lung Lesions group (SRLL, n = 54), comprised by patients declaring self-reported symptoms concomitant with diagnosed pulmonary lesions. In the follow-up assessment, participants answered questionnaires, performed physical tests, and blood was collected, for serum cytokine assessment. The variation in follow-up interval assessment was considered in the statistical analysis.
Results: In relation to Control, SRLL presented lower IL-10 and IL-4 (q = 0.0170 and q = 0.0208, respectively); lower IFNa2 and G-CSF (q = 0.0059 and q = 0.0175, respectively) and higher MIP-1β compared with SR (q = 0.0191). SR presented lower MCP-1 compared with Control (and q = 0.0381) and lower CCL11 levels, compared with Control and SRLL (q = 0.0109 and q = 0.0007, respectively). Female participants in SR and SRLL showed lower handgrip strength (q = 0.0623 and q = 0.0015, respectively) than women in the control group. Male participants in SR and SRLL needed more time to complete the timed up-and-go test (q = 0.0302 and q = 0.0078, respectively) in relation to controls.
Conclusions: Individuals with Long Covid presented lower muscle function in parallel with disrupted inflammatory markers and persistent self-reported symptoms, including fatigue. Heterogeneous long COVID symptom phenotypes are accompanied by distinct inflammatory markers in the circulation. The findings pointing to lower muscle function may have long-lasting consequences for health and quality of life and must be considered as an important sequela.
5-01
The association between protein intake and skeletal muscle parameters in patients with localized renal cell cancer
Mark Nieuwenhuis1, Jake S.F. Maurits1, J.P. Michiel Sedelaar2, Katja K.H. Aben1,3, Lambertus A.L.M. Kiemeney1 and Alina Vrieling1
1Department for Health Evidence, Radboud University Medical Center, Nijmegen, The Netherlands;2Department of Urology, Radboud University Medical Center, Nijmegen, The Netherlands;3Department of Research and Development, Netherlands Comprehensive Cancer Organization, Utrecht, The Netherlands
Introduction: Low skeletal muscle index (SMI) and low skeletal muscle density (SMD) have been associated with worse survival in several cancer types, including renal cell cancer (RCC). Increasing dietary protein intake may increase skeletal muscle mass, but findings from studies are inconsistent. This study is first to investigate the association of total, animal and plant protein intake with SMI and SMD in patients with localized RCC.
Methods: We included patients treated with a (partial) nephrectomy for stage I-III RCC who were enrolled in the population-based cohort ReLife between January 2018 and March 2020. Dietary intake was assessed with a 163-item food frequency questionnaire (FFQ). Body composition was assessed using diagnostic Computed Tomography (CT) images at the level of the third lumbar vertebra. Nutrient residual and multivariable nutrient density regression models were used to evaluate the independent associations of protein intake with SMI and SMD. All analyses were adjusted for age, sex, total energy, smoking, alcohol intake, moderate-to-vigorous physical activity, and tumour stage.
Results: In total, 199 patients with available dietary information and CT scans were included. Mean age was 61.7 ± 9.6 years, 73% of patients were male, and the majority of patients were overweight (46%) or obese (21%). Mean energy-adjusted protein intake was 0.92 ± 0.17 g/kg body weight/day. An increase of 0.1 g energy-adjusted total protein, animal protein, and plant protein per kg body weight/day was associated with a decrease in SMI (β: −0.88, 95% CI: −1.42, −0.34; β: −0.65, 95% CI: −1.29, −0.02; and β: −1.41, 95% CI: −2.37, −0.45, respectively). In contrast, these measures were associated with an increase in SMD (β: 1.73, 95% CI: 1.09, 2.36; β: 1.06, 95% CI: 0.33, 1.79; β: 3.28, 95% CI: 2.19, 4.37, respectively). No statistically significant associations were found for protein intake in g/day or for protein intake expressed as energy percentage.
Conclusions: These results suggest an inverse association between protein intake and skeletal muscle mass, but a positive association with skeletal muscle quality. Confirmation of these findings in our total ReLife cohort and stratified analyses by sex are planned.
5-02
An evidence based protocol for early identification of nutritional risk patients with cancer
Maurizio Muscaritoli1, Gil Bar-Sela2, Nicolo M.L. Battisti3,4, Borislav Belev5, Jorge Contreras-Martínez6, Enrico Cortesi7, Ione de Brito-Ashurst8, Carla M. Prado9, Paula Ravasco10,11 and Suayib Yalcin12
1Department Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2Oncology Department, Emek Medical Center, Afula, Israel;3Royal Marsden NHS Foundation Trust, London, UK;4Breast Cancer Research Division, Institute of Cancer Research, London, UK;5Clinical Hospital Center, School of Medicine, University of Zagreb, Zagreb, Croatia;6Hospital Regional de Malaga, Malaga, Spain;7Department of Radiological, Oncological and Pathological Sciences, Sapienza University of Rome, Rome, Italy;8Royal Marsden NHS Foundation Trust, London, UK;9Department of Agricultural, Food and Nutritional Science, University of Alberta, Edmonton, Canada;10Faculty of Medicine and Centre for Interdisciplinary Research in Health (CIIS-UCP), Universidade Católica Portuguesa, Lisbon, Portugal;11Centre for Interdisciplinary Research Egas Moniz (CiiEM), Instituto Universitário Egas Moniz, Almada, Portugal;12Department of Medical Oncology, Institute of Cancer, Hacettepe University, Ankara, Türkiye
Introduction: Nutritional and metabolic care in cancer still represents a largely unmet need. A practical protocol for nutritional risk in oncology to enable oncologists to identify patients with or at risk of malnutrition for further evaluation and follow-up is warranted. Such approach should be simple and quick to implement so to fit the oncologist's schedule.
Methods: A panel of nutrition specialists and practicing oncologists identified three factors as essential components to give a rapidly identify patients' nutritional and physical status: (i) body weight, (ii) appetite and food intake, and (iii) strength and mobility, The experts met twice in October 2021, with additional discussions occurring via email, allowing the development of the PROtocol for NuTritional risk in Oncology (PRONTO).
Results: By exploring through three simple questions three different domains, the protocol may allow for the fast identification of patients with or at risk of malnutrition and/or muscle depletion and provides guidance on next steps and is adaptable to multiple settings and countries, making implementation feasible by oncologists, ultimately optimizing patient outcomes.
Conclusions: This protocol could be used in countries/clinical scenarios where a specialized approach to nutrition care is not available. It was devised to give oncologists a simple nutritional protocol for optimization of the patient care pathway, and not to replace the already existing tools for malnutrition screening and assessment. Dissemination, validation testing, and feedback of the protocol are warranted.
Keywords: Cancer, early identification, malnutrition risk, protocol.
5-03
Preoperative supportive nutrition at major cancer surgery in weight-losing patients: effects on muscle transcriptome
Britt-Marie Iresjö and Ulrika Smedh and Cecilia Engström and Jan Persson and Christian Mårtensson and Kent Lundholm
Department of Surgery, University of Gothenburg and Sahlgrenska University Hospital, Göteborg, Sweden
Introduction: Recommendations of strict pre-operative fasting have later on become replaced by provision of carbohydrate rich nutrition drinks prior to surgery. Carbohydrate (cho) drinks are shown to reduce postoperative insulin resistance and thus assumed to improve post-surgical muscle protein metabolism with expectations to reduce morbidity and complication rate, though meta-analyses indicate few clinical benefits. However, such studies investigating skeletal muscle metabolism are lacking. Therefore, our study evaluates skeletal muscle transcriptome alterations with relevance to carbohydrate and protein metabolism, by two different nutrition interventions.
Method: Patients scheduled for major upper gastrointestinal cancer surgery were asked to participate. Mean weight loss in the patient group was 7%. Provision of either oral carbohydrate -rich nutrition drinks (804 kcal cho/96 kcal protein) or provision of peripheral total parenteral nutrition (TPN) (400 kcal cho/180 kcal protein/350 kcal fat) were administered in a 12-h over-night period prior to surgery. The control group received infusion of clear fluids only. Arterial blood samples and abdominal muscle biopsies were collected at operation start (n = 38). Blood amino acids were quantified by LC–MS/MS and muscle mRNA transcripts were analysed with Agilent SurePrint G3 Human GE v3 8x60K Microarrays. Data evaluation was done in Genespring software v.14.9.1.
Results: Statistical analyses indicated ~1200 transcripts as altered among groups (Anova, P < 0.05). Post-Hoc analyses indicated ~500 transcripts as altered by each nutrition protocol with most alterations specific to each treatment. The results indicate that both carbohydrate rich nutrition drinks and total parenteral nutrition influenced muscle glucose metabolism, while transcript alterations related to protein translation were induced by parenteral nutrition only.
Conclusions: Carbohydrate rich drinks were not sufficient to sustainably support muscle metabolism and should not be recommended in combination with major cancer surgery.
5-04
Cancer-associated anorexia: DNA methylation signatures in patients with lung cancer
Giovanni Imbimbo1, Federica Tambaro1, Francesca Ambrosani2, Silvia Udali2, Sara Moruzzi2, Annalisa Castagna2, Michele Melena1, Maurizio Muscaritoli1, Simonetta Friso2 and Alessio Molfino1
1Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy;2Department of Medicine, University of Verona School of Medicine, Verona, Italy
Introduction: Anorexia is an extremely disabling symptom in cancer and its pathogenesis is multifactorial. We aimed at evaluating the potential role of epigenetic regulation on those gene expression marks by analysing changes in methylation on PBMCs DNA of lung cancer patients presenting with poor appetite.
Methods: Genome wide DNA methylation analysis was performed in lung cancer patients at their first diagnosis compared to healthy controls. Anorexia was assessed by FAACT questionnaire. Four groups of genes were identified: hypermethylated repressed, hypermethylated induced, hypomethylated repressed and hypomethylated induced.
Results: The analysis was conducted on 24 participants to compare the DNA methylation status of anorexic cancer patients versus non-anorexic cancer patients and non-cancer controls. In cancer patients, 382 genes were differentially methylated compared to control group. Patients with cancer anorexia presented 586 hypomethylated and 174 hypermethylated genes compared to controls. Two hundred eleven genes were hypomethylated and 90 hypermethylated in anorexic versus non-anorexic cancer patients. When microarray methylation data were merged with RNA sequencing, we observed significant differences in anorexic cancer patients with respect to controls. In this comparison, 42 genes resulted hypomethylated induced, 5 hypermethylated repressed, 10 hypermethylated induced and 15 hypomethylated repressed. The CG sites analysed by targeted bisulfite sequencing in four genes of interest (FLNA, PGRMC1, GNL3L and FHL1) that resulted hypomethylated induced in the anorexic patients compared to healthy controls, allowed to validate the data obtained from DNA methylation analysis. Moreover, the four genes resulted significantly hypomethylated in anorexic patients with respect to non-anorexic patients and to controls (P < 0.0001).
Conclusions: Our data support in humans for the first time that epigenetic mechanisms through DNA methylation are implicated in anorexia in lung cancer patients.
5-05
Combined nutritional and exercise interventions for cachexia in chronic diseases: a systematic review
Masatsugu Okamura1,2,3, Kengo Shirado3,4, Nobuyuki Shirai3,5, Takuma Yagi3,6, Tatsuro Inoue3,7, Masato Ogawa3,8, Erin Stella Sullivan9, Stephan von Haehling10, Jochen Springer11, Stefan D. Anker12,13 and Ryo Momosaki14
1Berlin Institute of Health Center for Regenerative Therapies (BCRT), Charité – Universitätsmedizin Berlin, Berlin, Germany;2Department of Rehabilitation Medicine, Yokohama City University School of Medicine, Yokohama, Japan;3Change Nutrition from Rehabilitation – Virtual Laboratory (CNR), Niigata, Japan;4Department of Rehabilitation, Aso Iizuka Hospital, Fukuoka, Japan;5Department of Rehabilitation, Niigata Rinko Hospital, Niigata, Japan;6Department of Rehabilitation, Hattori Hospital, Miki, Japan;7Department of Physical Therapy, Niigata University of Health and Welfare, Niigata, Japan;8Department of Rehabilitation Science, Osaka Health Science University, Osaka, Japan;9Clinical Nutrition & Oncology Research Group, School of Food & Nutritional Sciences, University College Cork, Cork, Ireland;10Department of Cardiology and Pneumology, University Medical Center Göttingen, Göttingen and German Center for Cardiovascular Research (DZHK), partner site Göttingen, Göttingen, Germany;11Berlin Institute of Health Center for Regenerative Therapies (BCRT); German Center for Cardiovascular Research (DZHK), partner site Berlin; Charité – Universitätsmedizin Berlin, Berlin, Germany;12Department of Cardiology (CVK), Berlin Institute of Health Center for Regenerative Therapies (BCRT); German Center for Cardiovascular Research (DZHK), partner site Berlin; Charité – Universitätsmedizin Berlin, Berlin, Germany;13Institute of Heart Diseases, Wroclaw Medical University, Wroclaw, Poland;14Department of Rehabilitation Medicine, Mie University Graduate School of Medicine, Tsu, Japan
Introduction: Cachexia is a serious condition characterized by weight loss and decreased skeletal muscle mass, often observed in patients with chronic diseases such as cancer and chronic heart failure. As cachexia is associated with nutritional problems, nutritional and exercise interventions are expected to be effective. However, the combined effects of these interventions have not been thoroughly investigated. This systematic review aimed to examine the effects of combined nutritional and exercise interventions on cachexia in patients with chronic diseases.
Methods: We searched databases including MEDLINE (PubMed), Cochrane Central Register of Controlled Trials (Cochrane Library), Embase, CINAHL, PEDro, WHO-ICTRP, and ClinicalTrials.gov for studies up to March 13, 2023. We included studies that investigated the effects of combined nutritional and exercise interventions in patients with cachexia defined by criteria established by Evans et al. or Fearon et al. compared to control groups. We attempted to pool outcomes such as body weight, body composition, mortality, activities of daily living (ADL), physical function, exercise tolerance, and quality of life (QOL).
Results: We identified 1579 records, and ultimately included only two studies investigating the effects of combined interventions on cachexia in patients with cancer (Solheim, 2017 and Rogers, 2020). Despite limited research, these two studies suggested that combined nutritional and exercise interventions may practically alleviate cachexia symptoms. However, conducting a meta-analysis was difficult as these studies had limited data reporting and did not investigate common outcomes. No studies examining the effects of combined interventions on cachexia in other chronic diseases such as chronic heart failure, chronic kidney disease, and chronic obstructive pulmonary disease were included in this review. In addition, through the comprehensive search of databases, we were able to identify several ongoing studies within this field.
Conclusions: Our systematic review included several studies, but drawing definitive conclusions through meta-analysis proved challenging. At the same time, it became clear that there is very limited evidence supporting the expected benefits of combined nutritional and exercise interventions for cachexia. Future research is urgently needed to investigate the effects of combined interventions on cachexia in various chronic diseases. The results of other ongoing investigations are eagerly anticipated, and our research team is currently planning to conduct such a study.
6-01
Exercise decreases catabolic protein signalling in rat skeletal muscle 40 days post-burn
Dorien Dombrecht1, Birgit Van Asbroeck1, Pieter-Jan Guns2, Ulrike Van Daele1 and Eric van Breda1
1Department of Rehabilitation Sciences & Physiotherapy, Research group MOVANT, University of Antwerp, Antwerp, Belgium;2Laboratory of Physiopharmacology, University of Antwerp, Antwerp, Belgium
Introduction: During the hypermetabolic state after a burn injury skeletal muscle mass loss is caused by a negative protein balance. In muscle wasting diseases such as cancer, exercise has been found to counterbalance a negative protein balance by increasing anabolic and decreasing catabolic protein signalling. We examined, in a rat burn model, the effects of exercise on skeletal muscle protein synthesis and breakdown 40 days postburn.
Methods: 22 rats (6 weeks old) received a 40% TBSA burn according to the Walker-Mason model and were assigned to an exercise (E) or non-exercise (NE) group. Animals of the E group were subjected to progressive treadmill training of 60 min for 4 days a week. Forty days postburn, all animals were sacrificed, weighed and m.soleus (SOL) and m.extensor digitorum longus (EDL) were collected. Protein expression of pAkt and eEF2 proteins and of MURF-1, Atrogin-1 and FOXO3a were measured by Western blotting for analysis of protein synthesis and proteolysis, respectively. Protein expressions were normalized for Total Protein content. A linear mixed model was used to test for significant differences (P < 0.05 (*)) (Figure 1).
Results: NE burned rats showed significantly less body weight gain* 40 days postburn compared to E burned rats, characterized by lower muscle weight/body weight ratios for both SOL* and EDL*. In the E group, both SOL and EDL showed less proteolytic activity of MURF-1*, Atrogin-1* and FOXO3A* in comparison to NE rats. Protein synthesis signalling, Akt* and eEF2*, was lower in EDL of E rats, in SOL eEF2 was also lower while Akt* expression was higher in comparison with NE rats.
Conclusions: The most important finding is that exercise postburn increased muscle mass through a shift in protein signalling pathways towards less catabolic protein signalling, in comparison to non-exercising rats.
6-02
Effect of exercise on sarcopenic obesity (SO) patients: research progress and perspectives
Shengqi Huang1, Caihua Huang2 and Yongdong Cai1
1School of Physical Education and Sport Science, Fujian Normal University, Fuzhou, China;2Research and Communication Center for Exercise and Health, Xiamen University of Technology, Xiamen, China
Sarcopenic obesity (SO) is a prevalent and severely health-impairing geriatric syndrome characterized by the accumulation of body fat and a decrease in muscle mass and function. The prevalence of SO is reported to range from 5% to 10%. In 2022, the European Society for Clinical Nutrition and Metabolism (ESPEN) and the European Association for the Study of Obesity (EASO) published the first expert consensus on SO, which clarifies the definition, diagnosis and cut-off values. The pathogenesis of SO focuses on age-related changes in body composition, hormonal alterations, chronic inflammation, and poor lifestyle. The main adverse consequences of SO manifest as metabolic disorders, decreased physical function, increased risk of falls and disability, cognitive impairment, increased incidence of related complications and all-cause mortality. Exercise is well-proven to reduce body fat and increase muscle mass, suggesting it would be efficient for this population. However, guidelines for exercise prescription (ExRx) for SO have yet to be established. This paper aims to examine research on exercise training for SO, with regard to the components of ExRx, which are frequency, intensity, time, and type of exercise (FITT), and to evaluate the primary outcomes. The results show that exercise training improves body composition and function in SO patients. Resistance training is the primary type of exercise intervention, and its combination with aerobic exercise might be more effective in improving functional status in SO. The inadequacy of relevant research poses a challenge in determining the appropriate frequency and duration of exercise for SO. It is worth considering the ACSM ExRx guidelines for older adults, namely 3–5 days of aerobic exercise and at least 2 days of resistance exercise per week. Aerobic exercise needs to be guaranteed for 30–60 min (moderate intensity) or 20–30 min (higher intensity). There is no specific exercise duration recommendation for resistance exercise; however, it is crucial to engage in exercises that involve the major muscle groups during the workout. The intensity of aerobic exercise, mostly reported by rating of perceived exertion (RPE) scale(5–8 points, 1–10 scale). While for resistance training, it recommended to start with a low intensity (e.g. 40–50% of 1-RM) and gradually increase to moderate (e.g. 60–80% of 1-RM). Due to limited evidence, ExRx and its components for SO require further investigation, and the underlying mechanisms by which exercise exerts its effects need further exploration.
6-03
Effect and mechanism of exercise on diabetic sarcopenia: a systematic review
Yongdong Cai1, Caihua Huang2 and Shengqi Huang1
1School of Physical Education and Sport Science, Fujian Normal University, Fuzhou, China;2Research and Communication Center for Exercise and Health, Xiamen University of Technology, Xiamen, China
Introduction: The development of sarcopenia poses a significant threat to the well-being and quality of life of elderly individuals. Research interest is currently directed towards the coexistence of sarcopenia and diabetes as a co-morbid condition, given that sarcopenia is regarded as a potential complication arising from diabetes. A reciprocal relationship exists between sarcopenia and diabetes, forming a vicious cycle. Numerous studies have confirmed that exercise interventions are effective in improving diabetes and sarcopenia, although the underlying mechanisms remain unclear. Therefore, this study analyses studies related to exercise interventions in diabetic sarcopenia according to the FITT principle of exercise prescription and explores the possible mechanisms involved.
Methods: Searches of PubMed, Web of Science, Embase, and Cochrane Library databases were performed for studies published in English from the earliest date available to April 2023. Randomized controlled trial (RCT) studies were reviewed to explore the effects of exercise interventions on individuals with diabetic sarcopenia. The study on exercise intervention was summarized with regard to the FITT principles, encompassing the frequency, intensity, time, and type of exercise. Mechanisms of exercise affecting diabetic sarcopenia study selected reliable experiments and papers for citation. Twelve RCT studies with a total of 652 patients were included in this study.
Results: Aerobic exercise is more effective than resistance exercise in increasing maximal oxygen uptake and improving glycaemic control, and resistance exercise is more effective than aerobic exercise in maintaining and increasing the muscle mass. Aerobic combined resistance exercise combines the advantages of both types of exercise mode. The main possible mechanisms of exercise intervention for diabetic sarcopenia are the inhibition of inflammatory factor expression, increased insulin sensitivity, improved skeletal muscle microvascular function, and activation of mitochondrial autophagy.
Conclusions: This study found, through systematic evaluation, that patients who chose aerobic exercise at an intensity of 60–80% of maximum heart rate or resistance exercise at an intensity of 50–70% of 1RM for 8–12 weeks, at a frequency of 3 times a week for 30–45 min, improved muscle mass, muscle strength, and physical function in patients with diabetes. Sarcopenia and diabetes form a vicious circle, with the adverse effects of sarcopenia and diabetes interacting to exacerbate the patient's condition. Exercise can break this vicious circle by improving insulin sensitivity, blood glucose regulation, and reducing inflammation to treat diabetic sarcopenia.
6-04
Higher fibroblast growth factor 23 levels are associated with low exercise capacity in patients with chronic heart failure: results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF)
Ryosuke Sato1, Tania Garfias-Veitl1,2, Mirela Vatic1,2, Guglielmo Fibbi1, Wolfram Doehner3,4,5, Stefan D. Anker3,5,6 and Stephan von Haehling1,2
1Department of Cardiology and Pneumology, University Medical Center Goettingen, Georg- August University, Goettingen, Germany;2German Center for Cardiovascular Research (DZHK), partner site Goettingen, Goettingen, Germany;3Berlin Institute of Health-Center for Regenerative Therapies (BCRT), Charité- Universitätsmedizin Berlin, Berlin, Germany;4Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany;5German Center for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany;6Division of Cardiology and Metabolism - Heart Failure, Cachexia & Sarcopenia, Department of Cardiology (Virchow Klinikum), Charité University Medical Center Berlin, Berlin, Germany
Introduction: Fibroblast growth factor 23 (FGF-23) is a key regulator of phosphate metabolism, inhibiting phosphate reabsorption and vitamin D activation in the proximal renal tubules. Meanwhile, several studies have shown that higher FGF-23 levels are associated with disease severity and adverse outcomes in heart failure (HF). However, the relationship between FGF-23 levels and exercise capacity in HF with reduced ejection fraction (HFrEF) patients remains unclear.
Methods: A total of 213 patients (67 ± 11 years, 79% men) with HFrEF were evaluated for FGF-23 levels and exercise capacity from the Studies Investigating Co-morbidities Aggravating HF (SICA-HF). The Full-length intact FGF-23 level in the serum samples was detected using Human FGF-23 Enzyme Linked-Immuno-Sorbent Assay Kit (Merck KGaA, Darmstadt, Germany), and patients were divided into lower and higher FGF-23 groups based on the median value of 90 pg/mL. Exercise capacity was assessed by a treadmill cardiopulmonary exercise testing with a modified Bruce protocol for peak oxygen uptake (VO2), with patients divided into low and high exercise capacity using the median value of 16.7 mL/kg/min.
Results: Patients with higher FGF-23 levels were significantly older, had higher New York Heart Association class, lower left ventricular ejection fraction, higher prevalence of sarcopenia, and higher levels of high-sensitivity C-reactive protein (2.4 [1.2–3.9] vs. 1.5 [0.7–3.1] mg/L, P = 0.001), parathyroid hormone (55 [37–91] vs. 38 [31–48] pg/mL, P < 0.0001), and N-terminal pro-B-type natriuretic peptide (926 [374–1936] vs. 315 [152–770] pg/mL, P < 0.0001), and lower levels of haemoglobin (13.1 [12.1–14.4] vs. 13.7 [13.0–14.6] g/dL, P = 0.01) and estimated glomerular filtration rate (57 [43–75] vs. 77 [64–87] mL/min/1.73 m2, P < 0.0001) than those with lower FGF-23 levels. Muscle strength and exercise capacity were significantly lower in patients with higher than those with lower FGF-23 levels (handgrip strength: 36 ± 11 vs. 41 ± 12 kg, P = 0.001; quadriceps strength: 37 ± 11 vs. 44 ± 14 kg, P < 0.0001; peak VO2: 15.2 ± 4.2 vs. 18.8 ± 4.6 mL/min/kg, P < 0.0001). Multivariate logistic regression analysis revealed that higher FGF-23 levels were significantly associated with low exercise capacity (adjusted OR 2.62, 95% CI 1.06–6.44, P = 0.04).
Conclusions: In patients with chronic stable HFrEF, higher FGF-23 levels are significantly associated with low exercise capacity.
6-05
Associations of exercise habits in adolescence and old age with phase angle in older adults: the Bunkyo Health Study
1Sportology Center, Juntendo University Graduate School of Medicine, Tokyo, Japan;2Sports Medicine and Sportology, Juntendo University Graduate School of Medicine, Tokyo, Japan;3Metabolism and Endocrinology, Juntendo University Graduate school of Medicine, Tokyo, Japan;4Center for Healthy Life Expectancy, Juntendo University, Graduate School of Medicine, Tokyo, Japan
Introduction: Phase angle (PhA) is a bioelectrical marker determined through bioelectrical impedance analysis, and higher PhA is associated with better cellular integrity, higher skeletal muscle mass, strength and quality (Silva et al., Sport Sciences for Health, 2022). Earlier studies reported that exercise enhanced phase angle (Martins et al., Arch Gerontol Geriatr, 2022), and we recently showed that older adults with exercise habits in both adolescence and old age exhibited high muscle function (Tabata et al. J. Cachexia Sarcopenia Muscle, 2023). Thus, the present study investigated the associations between exercise habits in adolescence and older age, and their impact on PhA among older adults.
Methods: This study was conducted using data from the Bunkyo Health Study, a cohort study for 65–84 older adults. We included 676 men and 926 women who completed the full data of analysis necessary. In the current study, we defined the lower fifth of the PhA value as a PhA decline. We divided participants into four groups by combination of exercise habits: never exercised (NN), exercised only in adolescence (AN), exercised in old age (NA), and exercised both in adolescence and old age (AA). Logistic regression models adjusted for potential confounders were used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for the prevalence of PhA decline. As potential confounders, we adjusted age, years of education, smoking status, protein intake, and the presence of diabetes mellitus, cardiovascular diseases, and osteoporosis.
Results: The cut-off value of PhA decline is 4.6 in men and 4.1 in women. In men, the ORs (95% CI) for PhA decline were not significantly different among the groups {NA: 1.01 (0.51–2.0), P = 0.975, AN: 1.7 (0.96–3.0), P = 0.069, AA: 0.74 (0.38–1.5), P = 0.388}. In the women, the ORs of the AA group was lower than the NN group {0.51 (0.29–0.88), P = 0.015}, whereas the NA group and the AN group were not significantly different than the NN group {NA: 0.73 (0.45–1.17), P = 0.187, AN: 0.66 (0.42–1.04), P = 0.072}.
Conclusions: Older women, but not older men, with exercise habits in both adolescence and old age were at low risk of PhA decline.
6-06
Loss of hypoxia signalling-mediated PGC-1a expression underlies age-related loss of muscular adaptation to exercise
Yori Endo and Mehran Karvar and Yuteng Zhang and Christina Zhu and Daniel Koh and Indranil Sinha
Brigham and Women's Hospital, Havard Medical School, Boston, MA, USA
Background: Exercise is necessary for the prophylaxis/treatment of aging-associated muscle loss or sarcopenia. However, muscular adaptation to exercise becomes increasingly diminished with aging, limiting the treatment efficacy. This likely reflects aging-related dysregulation of the required myogenic signalling pathways. Our previous studies uncovered loss of hypoxia signalling activation following exercise in aged muscle, accompanied by an elevation of prolyl hydroxylase domain enzyme (PHD)2 responsible for regulating HIF1A, the master transcriptional activator of the hypoxia signalling pathway.
Methods: Young (12–14 weeks old) and old (21 months old) mice were subjected to either 40 min of running training protocol at approximately 70% of VO2 5 times per week for 8 weeks. The mice were tested for physiological performance, muscle functions, and gastrocnemius muscles were evaluated for histological, biochemical, and gene expression changes (Figure 1).
Results: Young, trained mice exhibited a significant increase in maximum distance running (250%, P < 0.001), maximal running speed (23%, P = 0.03), in comparison to age-matched untrained mice. In contrast, both trained and untrained old mice demonstrated similar endurance and maximal speed. Muscle fibre composition of gastrocnemius revealed a 2.5-fold increase (P = 0.02) and 30% increase in the Type I and Type IIa fibres (P = 0.03) in trained young mice, respectively, where these were absent in aged muscles. RNA seq analysis gastrocnemius muscles revealed 96 and 146 to be differentially regulated with exercise treatment in young and old mice, respectively, without any overlap, where 85% of the top 20 most upregulated genes in exercised young mice were the transcriptional targets of HIF1A. The exercise training led to a 50% decrease in PHD2 protein levels (P = 0.006) with corollary increase in the HIF1A and PGC-1a protein levels in muscle of young mice, in contrast to old mice where neither change was present. Muscle-specific ablation of ARNT (transcriptional co-factor of HIF1A) or PHD2 elevation in vivo exhibited reduced response to exercise training, improvement in muscle fatigue, and fibre-type adaptation. Supplementation of old mice and these transgenic mice with ML228, HIF activator, partially reversed these parameters and improved overall physiological and muscular functions (Figure 2).
Conclusions: Age-related elevation of PHD2 hinders PGC-1a mediated fibre type adaptation and gain of muscle endurance by inhibition of HIF1A transcriptional activity in response to exercise. Pharmacological activation of HIF offers a promising method for improving exercise-based therapies for sarcopenia.
6-07
Body cell mass to fat-free mass ratio and extra-to-intracellular water ratio are related to maximal oxygen uptake
Yosuke Yamada and Tsukasa Yoshida and Haruka Murakami and Yuko Gando and Ryoko Kawakami and Harumi Ohno and Kumpei Tanisawa and Kana Konishi and Julien Tripette and Emi Kondo and Takashi Nakagata and Hinako Nanri and Motohiko Miyachi
Department of Physical Activity Research, National Institute of Health and Nutrition, National Institutes of Biomedical Innovation, Health and Nutrition, Osaka, Japan
Fat-free mass (FFM) is a heterogeneous compartment comprising body cell mass (BCM), intracellular water (ICW), extracellular solids, and extracellular water (ECW). The BCM/FFM and ECW/ICW ratios vary among individuals and decrease with age. This study aimed to determine whether BCM/FFM and ECW/ICW ratios are predictors of maximal oxygen uptake (V̇O2peak) independently of age, sex, and objectively measured physical activity (PA). A total of 115 Japanese males and females, aged 55.3 ± 8.0 years (mean ± standard deviation), were included in the study. Anthropometry, explosive leg muscle power, and V̇O2peak were measured, and BCM, FFM, ICW, and ECW were estimated. Step count and PA were objectively measured using a triaxial accelerometer. Blood flow volume was assessed using ultrasonography. BCM and ICW were negatively correlated with age, whereas FFM and ECW were not significantly correlated with age. FFM, ICW/ECW, BCM/FFM, step counts, moderate and vigorous PA, and leg muscle power were positively correlated with V̇O2peak, even after adjusting for age and sex (P < 0.05). Multiple regression analysis indicated that either BCM/FFM or ECW/ICW, leg power, and objectively measured PA were associated with V̇O2peak independent of age, sex, and FFM. Blood flow volume was significantly correlated with ECW (P < 0.05), but not with BCM. The BCM/FFM and ECW/ICW ratios were significant predictors of VO2peak, independent of age, sex, FFM, leg power, and objectively measured PA.
7-01
Anti-RANKL treatment attenuates mitochondria deterioration and suppresses macrophage infiltration during sarcopenia
Can Cui, Yufeng Long, Wujian Lin, Chaoran Liu, Ronald Man Yeung Wong, Ning Zhang and Wing-hoi Cheung
Department of Orthopaedics & Traumatology, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, Hong Kong
Introduction: Sarcopenia is an age-related geriatric syndrome which is associated with subsequent disability and morbidity. Currently there is no promising therapy approved for treatment. The receptor activator of nuclear factor NF-κB ligand (RANKL) is expressed in skeletal muscle and its activation mainly inhibits myogenic differentiation, which leads to skeletal muscle dysfunction. CD206 positive macrophage has been reported to be associated with progressive impairment of skeletal muscle function with aging. The study aims to investigate the effects of an anti-RANKL treatment on sarcopenic skeletal muscle and explore the related mechanisms in mitochondria modulation and the polarization status of macrophages.
Methods: Sarcopenic senescence-accelerated mouse P8 (SAMP8) mice at month 6 were treated intraperitoneally with 10 mg/kg anti-RANKL (Bio X Cell) every 2 weeks and harvested at month 10 (Figure 1A). Senescence accelerated mouse resistant-1 (SAMR1) were collected at month 10 as age-matched non-sarcopenic group. Ex-vivo functional assessment, grip strength, oil red and immunostaining of CD45, F4/80, CD206, iNOS, C/EBPa, and Pax7 were performed. Mitochondria morphology was examined with a transmission electron microscope (Hitachi H7700, Tokyo, Japan). Data analysis was done with one-way ANOVA, and the significant level was set at P ≤ 0.05.
Results: After anti-RANKL treatment, tetanic, twitch force and grip strength were significantly higher than CTL group (P < 0.01, P < 0.01 and P < 0.05, Figure 1B). The SAMP8 mice at month 10 expressed significantly more C/EBPα (intramuscular adipose marker), CD206 (M2 marker) and LYVE1 (macrophage marker) positive area than in SAMR1 (Figure 1C). Anti-RANKL treatment could significantly decrease CD45 (general leukocyte marker), F4/80 (M1 marker), iNOS (M1 Marker), C/EBPα and CD206 positive area and oil red area, and significantly increase PAX7 (MDSC marker) positive cell numbers (Figure 1C and 1E). There was an increase in the number of intermyofibrillar mitochondria and restoration of mitochondria morphology in Anti-RANKL group. The structure of mitochondria and their cristae were more compact, compared with swollen mitochondria in the isotype group (Figure 1D).
Conclusions: These results indicated excessive inflammation and promoted the shift from M1 to M2 in macrophage phenotype during sarcopenia. The anti-RANKL treatment protected against sarcopenic skeletal muscle through suppressing muscle inflammation and modulating mitochondria which may represent a novel therapeutic approach for sarcopenia.
Acknowledgement: Collaborative Research Fund (CRF, Ref: C4032-21GF), CUHK Direct Grant (Ref: 4054690).
7-02
Enhanced glutamine availability exerts different effects on protein and amino acid metabolism in muscles of healthy and septic rats
Milan Holeček and Ludek Šišpera
Department of Physiology, Charles University, Faculty of Medicine Hradec Králové, Czech Republic
Introduction: Glutamine (GLN) supply may affect the catabolism of branched-chain amino acids (BCAAs; valine, leucine, and isoleucine), which play a regulatory role in protein turnover. We examined the effects of enhanced GLN availability on leucine oxidation, amino acid concentrations, and protein metabolism in muscles from healthy and septic rats.
Methods: Cecal ligation and puncture was used as a model of sepsis. Twenty-four hours after surgery, the soleus (SOL, red muscle) and the extensor digitorum longus (EDL, white muscle) were incubated in medium containing 0.5 or 2.0 mM GLN, and L-[1-14C]leucine. Protein breakdown, protein synthesis, and leucine oxidation were determined via 3-methylhistidine release, L-[1-14C]leucine radioactivity in muscle protein, and the radioactivity of released 14CO2, respectively.
Results: In muscles from septic animals, increased proteolysis and leucine oxidation, and decreased protein synthesis were detected. These effects were more pronounced in the EDL. In septic muscles, the addition of GLN decreased leucine oxidation in both muscles and increased protein synthesis in the EDL. In muscles of untreated animals, decreased leucine oxidation after the addition of GLN to the medium was associated with decreased protein synthesis in the SOL and decreased concentrations of serine, glycine, histidine, alanine, arginine, proline, and lysine in both muscles.
Conclusions: White muscle fibres are more sensitive to septic stimuli than red fibres are. In sepsis may enhanced GLN intake ameliorate GLN deficiency, inhibit BCAA catabolism, and stimulate protein synthesis. In the healthy state, surplus of GLN may lead to marked alterations in the intramuscular concentration of several amino acids and impair protein synthesis.
Financial Support: Charles University, the Cooperation Programme, research area METD.
7-03
Exploring lonafarnib's potential for sarcopenia treatment in dexamethasone-induced muscle atrophy models
Sang Hoon Bae1 and Jung Keun Hyun1,2,3
1Department of Nanobiomedical Science & BK21 NBM Global Research Center for Regenerative Medicine, Dankook University, Cheonan, Korea;2Department of Rehabilitation Medicine, College of Medicine, Dankook University, Cheonan, Korea;3Institute of Tissue Regeneration Engineering (ITREN), Dankook University, Cheonan, Korea
Introduction: Sarcopenia, characterized by age-related muscle weakness and a decline in muscle mass, is associated with increased falls, frailty, and mortality. This progressive and generalized skeletal muscle disorder affects the elderly population, leading to functional decline and a reduction in quality of life. Lonafarnib, an FDA-approved drug for Hutchinson-Gilford progeria syndrome and it has been shown to improve cardiovascular and skeletal abnormalities, which suggests that it may have beneficial effects on muscle tissue as well. This study investigated the potential of lonafarnib in treating sarcopenia using dexamethasone-induced muscle atrophy models in C2C12 myoblasts and rats.
Methods: We employed in vitro and in vivo dexamethasone-induced sarcopenia models. C2C12 myoblasts were treated with dexamethasone and lonafarnib, and myotube area, fusion index (FI), and muscle fibre diameter were assessed. Rats were divided into six groups: control without dexamethasone, control with 1 μM or 5 μM lonafarnib, dexamethasone-induced sarcopenia model without lonafarnib, and sarcopenia model with 1 μM or 5 μM lonafarnib. Body weight, grip strength, and electrophysiological studies were performed. After sacrifice, hind limb muscles were analysed using immunohistochemistry for dystrophin and cytochrome C.
Results:In vitro sarcopenia models revealed that optimal concentrations of lonafarnib significantly increased myotube area and FI in dexamethasone-treated C2C12 myoblasts. Additionally, in vivo sarcopenia animal models showed that optimal concentrations of lonafarnib attenuated dexamethasone-induced body weight loss, grip strength reduction, and hindlimb muscle compound muscle action potential amplitude decrease. Lonafarnib also restored dexamethasone-induced cross-sectional area reduction and increased cytochrome C area, indicating its potential to promote functional restoration.
Conclusions: Lonafarnib effectively counteracted dexamethasone-induced muscle atrophy both in vitro and in vivo, demonstrating its potential as a promising therapeutic candidate for sarcopenia. Further research is needed to explore the molecular mechanisms underlying these effects and assess the drug's efficacy in clinical settings (Figures 1 and 2).
Acknowledgement: This study was supported by grants (2022R1A6A3A01086668, 2022M3H4A1A0409882011, RS-2023-00208315) through the National Research Foundation (NRF) and Ministry of Science and ICT (MSIT) funded by the Korean government.
7-04
Muscle protein synthesis with a hybrid dairy and plant-based protein blend (P4) is equal to whey protein in a murine aging model after fasting
Francina J. Dijk1, Zandrie Hofman1, Yvette C. Luiking1, Matthew J.W. Furber1, Justin D. Roberts1,2, Ardy van Helvoort1,3 and Miriam van Dijk1
1Danone Nutricia Research, Utrecht, The Netherlands;2Cambridge Centre for Sport and Exercise Sciences, Anglia Ruskin University, Cambridge, UK;3NUTRIM School of Nutrition and Translational Research in Metabolism, Maastricht University Medical Center+, Maastricht, The Netherlands
Introduction: P4, a specific combination of dairy proteins (whey and casein) and plant-based protein isolates (pea and soy) has been shown to provide a more balanced amino acid (AA) profile than its constituent single proteins [1]; however, less is known about how this translates to muscle protein synthesis (MPS). The aim of this study was to investigate the effect of P4 compared to whey or casein against fasted control on MPS.
Methods: C57/BL6Rj mice, aged 25 months, were fasted overnight, followed by an oral gavage of either whey, P4, casein, or water as a fasted control. Thirty minutes after ingestion, puromycin (0.04 μmol·g−1 bodyweight) was subcutaneously injected; 30-min thereafter, mice were sacrificed. MPS, were measured by SUnSET-method, and signalling proteins were determined in the left-tibialis anterior (TA) muscle by WES-technique. AA-composition was determined in plasma and right-TA muscle. Dried blood spots (DBS) were analysed for postprandial AA-dynamics at 10-20-45-60-min.
Results: MPS was 1.6-fold increased with whey (P = 0.006) and 1.5-fold with P4 compared to fasted (P = 0.008), while no change was seen with casein (see Figure). This was confirmed by a significant increase of phosphorylated/total ratio of 4E-BP1 for both whey (P = 0.004) and P4 (P = 0.003). No changes were observed in p70S6K and mTOR phosphorylation/total ratio with whey or P4, however phosphorylation/total ratio was significantly lower in casein compared to fasted (P = 0.027). Intramuscular leucine levels were lower for P4 (0.71 μmol·g dry weight−1) compared to whey (0.97 μmol·g dry weight−1) (P = 0.0006). Ten minutes postprandial, DBS showed significantly increased blood AA-levels of BCAAs, histidine, lysine, threonine, arginine, and tyrosine for P4 versus fasted.
Conclusions: A mix of dairy and plant-based proteins (P4) resulted in a MPS response that was similar to whey protein in aged mice after fasting. This suggests that other anabolic triggers beyond leucine or the well-balanced amino acid profile and bioavailability of the blend benefit stimulation of MPS (Figure 1).
1. Liu, J.; Klebach, M.; Visser, M.; Hofman, Z.Amino Acid Availability of a Dairy and Vegetable Protein Blend Compared to Single Casein, Whey, Soy, and Pea Proteins: A Double-Blind, Cross-Over Trial. Nutrients2019, 11, doi:https://doi.org/10.3390/nu11112613, 2613.
7-05
A novel first-in-class USP19 inhibitor for the treatment of cancer-induced muscle atrophy
Richard D.A. Wilkinson1, Vignesh Karthikaisamy2, Darren M. O'Hara1, Aaron N. Cranston1, Colin R. O'Dowd1, Xavier Jacq1, Stephanie Burton1, Hayley Gibson1, Joana Costa1, Daniel Longley1, Matthew Helm1, Chris McGivern1, Steven Shepherd1, Christina Bell1, Steven Shepherd1, Peter Hewitt1, Mary McFarland1, Hugues Miel1, Steven Whitehead1, Lauren Proctor1, J.S. Shane Rountree1, Mark Wappett1, Natalie Page1, Mauricio Berriel Diaz2, Stephan Herzig2 and Timothy Harrison1
1Almac Discovery, Health Sciences Building, 97 Lisburn Road, Belfast, Ireland;2Helmholtz Centre Munich, Institute for Diabetes and Cancer (IDC), Neuherberg, Germany
Introduction: Cancer cachexia is a metabolic wasting syndrome characterized by weight loss, anorexia and anaemia as a result of tumour burden, and affects up to 80% of advanced cancer patients #1. Cachexia is particularly prevalent in pancreatic, lung, colorectal and gastrointestinal cancers and can lead to reduced tolerance and responsiveness to chemotherapy, increased treatment-related toxicity and morbidity, and poor overall quality of life. There are currently no approved therapies for cancer cachexia. The development and maintenance of muscle tissue is dependent on the balance between protein synthesis and protein degradation, controlled through various anabolic and catabolic signalling pathways. Dysregulation of these pathways can result in muscle atrophy, which arises in many chronic illnesses. The ubiquitin proteasome system (UPS) has a central role in regulating skeletal muscle physiology. Previous work utilizing USP19 knock out mouse models has demonstrated that USP19 plays an important role in muscle wasting and can protect against denervation-induced muscle atrophy #2. We have previously demonstrated that inhibition of USP19 enzymatic activity spares the muscle wasting observed in limb-casted and denervated mouse models of muscle wasting.
Method: Here, we report the discovery of a novel, highly potent and selective inhibitor of USP19 (ADC-846) and demonstrate its utility in an in vivo Lewis lung carcinoma-induced (LLC) cachexia model of muscle atrophy.
Result: Pharmacological inhibition of USP19 by ADC-846 increased lean muscle and fat mass following oral dosing in an LLC cachexia model and reduced the cachexic index by >60% compared to controls.
Conclusions: These data, in combination with our previous work detailing the effect of USP19 inhibition on muscle force and function, provide a much-needed novel pharmacological strategy for therapeutic intervention in muscle wasting conditions.
#1 Haehling, S, Anker, MS, Anker, SD. Prevalence and clinical impact of cachexia in chronic illness in Europe, USA, and Japan: facts and numbers update 2016. J Cachexia Sarcopenia Muscle.2016 Dec; 7(5): 507–509.
#2 Bédard, N, Jammoul, S, Moore, T, Wykes, L, Hallauer, PL, Hastings, KE, Stretch, C, Baracos, V, Chevalier, S, Plourde, M, Coyne, E, Wing, SS. Inactivation of the ubiquitin-specific protease 19 deubiquitinating enzyme protects against muscle wasting. FASEB J.2015 Sep; 29(9): 3889–98.
7-06
Changes in CaCo-2 mRNA expression pathways affected by in vitro testosterone exposure
Ioanna Drami1,2, Victor Konstantellos1, Nick Powell1, Thanos Athanasiou1, John T. Jenkins1,2, Nikolaos Demertzis1 and Stella Knight1
1Imperial College London, London, UK;2St Mark's Hospital and Academic Institute, Central Middlesex, Acton Lane, London, UK
Introduction: Cohort studies in male populations link reduced testosterone levels to increasing colorectal cancer incidence. Testosterone has been used in the aging population to improve body composition, in different cancer types and in the perioperative timeframe to improve patient related outcomes. So far there is no clear evidence to link the use of perioperative testosterone in colorectal cancer patients, to improve their body composition is affecting the cancer progression. Our aim was to describe differences in mRNA expression patterns in a well-established colon adenocarcinoma cell line, treated with testosterone for 12 and 24-h to identify pathways which could lead to cancer progression.
Methods: CaCo-2 cells (passages 12–20) were cultured in DMEM supplemented with 5% FBS, 2 mM L-glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin, 1% NEAA, at 37°C with 5% CO2. Cells were sub cultured at 70–85% confluence. Evaluation of testosterone-related cytotoxicity was performed by the MTT colorimetric assay to identify the LD50 for the 12-and 24-h treatment. The lower and higher physiological testosterone concentrations as well as the LD50 were added at 70–80% confluent cells. mRNA was isolated from the CaCo-2 cells using the RNAeasy kit (Qiagen). Sequencing was performed using the Illumina PE-150 platform. Following quality control (fastQC & cutadapt) and read mapping/quantification (HISAT2 & featurecounts), the DESeq2 R/Bioconductor pipeline was used to identify differentially expressed genes. Pathway enrichment analysis was performed using overrepresentation (enrichR) and gene set enrichment analysis (GSEA), while the Hallmark, KEGG, Reactome, PID, Wikipathways, HumanCyc, and Biocarta databases were queried.
Results: Pathway enrichment analysis indicated upregulation of lipid metabolism pathways at 12 and 24-h testosterone treatment windows. The inflammatory response remained similar for the physiological doses but was upregulated at LD50, enhancing expression of IL-2, IL-6, and TGFβ. mTORC1 and Wnt/β-catenin signalling reduction at the LD50 for both groups. Genes upregulated by K-ras activation showed heterogeneous changes at the LD50 concentrations for both 12 and 24-h treatments. Hedgehog signalling was significantly reduced at the 24-h treatment. Notch signalling indicated changes at the LD50 concentration for both 12 and 24-h.
Conclusions: Testosterone treatment alters pathways involved in progression, migration and growth in the CaCo-2 cell line. This has shown promising results for clinical utility but ex vivo and in vivo experiments are required to assess safety and efficacy.
7-07
CaCo-2 intracellular calcium changes following testosterone treatment
Ioanna Drami1,2, Viktor Konstantellos1, Nick Powell1, Thanos Athanasiou1, John T. Jenkins1,2, Nikolaos Demertzis1 and Stella Knight1
1Imperial College London, London, UK;2St Mark's Hospital and Academic Institute, London, UK
Introduction: Intracellular calcium (Cai) homeostasis is important for regulating cellular functions. Previous studies in various cancer cell lines have identified changes in the apoptosis, altered cellular responses to stimuli, altered oxidative response and promotion of cell invasion. Testosterone induces a spike on Cai in myocytes and induces apoptosis in neuronal cells. There is no current evidence on how supplementary testosterone for body composition improvement affects the adenocarcinoma progression in patients. The aim of this study is to identify dynamic and endpoint Cai changes in CaCo-2 when treated with both physiological and supraphysiological testosterone concentrations.
Methods: CaCo-2 cells (passages 12–20) were cultured in DMEM supplemented with 5% FBS, 2 mM L-glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin, 1% NEAA, at 37°C with 5% CO2. Cells were sub cultured at 70–85% confluence. Testosterone-related cytotoxicity was performed by the MTT colorimetric assay kit (ab21109). CaCo-2 cells were grown in a 96-well plate, treated with growth media without FBS and with the addition of physiological and supraphysiological (LD50) testosterone concentrations for 12 and 24 h, in order to measure the endpoint calcium homeostasis. The cells were also grown in a 96-well plate in PBS, the physiological and supraphysiological testosterone concentrations were added in order to identify the acute dynamic changes in Cai for the first 2 min while colorimetric measurements were taken at 20 sec intervals Cai concentration was measured using the Fluo- 4NW Calcium Assay Kit (Invitrogen) on a microplate reader (BMG Labtech).
Results: There was statistical significance between the treatment concentrations at 12 h as determined by one-way ANOVA (F = 6.971, P = 0.003), Tukey post hoc test identified differences between the highest physiological testosterone concentration and LD50 at 12 h (P = 0.002) for the endpoint Cai levels. At 24 h treatment, the Cai results one-way ANOVA (F = 9.027, P = 0.0007), Tukey post hoc test showed a difference between the highest physiological concentration and LD50 (P = 0.0005). For the dynamic Cai changes at 12-h and 24-h treatment results are illustrated in Figure 1.
Conclusions: Supraphysiological testosterone levels significantly reduce Cai compared to physiological levels and can induce cell death in CaCo-2 cells when Cai is measured at the end of the in vitro treatment. Dynamic Cai show the highest changes at the LD50 12-h treatment doses. Future studies should concentrate on pathway and membrane receptor expression and changes during the treatment.
7-08
Developing an evidence and theory based multimodal integrative intervention for the management of renal cachexia: a theory of change
Carolyn Blair1, Adrian Slee2, Andrew Davenport3, Denis Fouque4, William Johnston5, Kamyar Kalantar-Zadeh6, Peter Maxwell7, Clare McKeaveney1, Robert Mullan8, Helen Noble1, Sam Porter9, David Seres10, Joanne Shields11, Ian Swaine12, Miles Witham13 and Joanne Reid1
1School of Nursing and Midwifery, Belfast, UK;2Division of Medicine, Faculty of Medical Sciences, University College London, London, UK;3UCL Department of Renal Medicine Royal Free Hospital, University College London, London, UK;4Division of Nephrology, Dialysis and Nutrition, Hôpital Lyon Sud and University of Lyon, Lyon, France;5Northern Ireland Kidney Patients Association, Belfast, UK;6Irvine Division of Nephrology, Hypertension and Kidney Transplantation, University of California, California, CA, USA;7Centre for Public Health, Queen's University Belfast, Belfast, UK;8Renal Unit, Antrim Area Hospital, Northern Health & Social Care Trust, Belfast, UK;9Department of Social Sciences and Social Work, Bournemouth University, Bournemouth, UK;10Institute of Human Nutrition and Department of Medicine, Columbia University Irving Medical Center, New York, NY, USA;11Belfast Health & Social Care Trust, Regional Nephrology Unit, Belfast City Hospital, Belfast, UK;12School of Human Sciences, University of Greenwich, London, UK;13AGE Research Group, NIHR Newcastle Biomedical Research Centre, Campus for Aging and Vitality, Newcastle upon Tyne, UK
Introduction: Many health research advisory bodies have suggested that it is best practice to report on the Theory of Change (ToC) prior to piloting and evaluating an intervention to ensure the context and the effective elements of the intervention are understood. However, there are no previous ToC studies in relation to renal cachexia. Therefore, the aim of this study was use ToC to develop a theoretical framework for a multimodal, integrative, exercise, anti-inflammatory and dietary counselling (MMIEAD) for patients with renal cachexia, to better understand the causal pathways, anticipated outcomes and most suitable evaluation methods.
Methods: We used a Theory of Change (ToC) approach to guide six steps. Step 1 included inputs from a key stakeholder workshop, step 2 included the findings of our mixed-methods study and step 3 included the results from our systematic literature review. In step 4, we used wider research to identify the underlying causal pathways for renal cachexia. In steps 5 and 6, we developed and refined the ToC map in consultation with key stakeholders to illustrate how the intervention components of MMIEAD interact to achieve the intended long-term outcomes and anticipated impact.
Results: The ToC approach to this study provided a theoretical framework which allowed the context and effective elements of an intervention for renal cachexia patients to be better understood. We were able to develop a ToC map which not only allowed the design of a multi-modal intervention, but also delineation of the ‘causal pathway’, ‘ceiling of accountability’, ‘preconditions’ and identification of the ‘ultimate impact’ of the intervention (improved quality of life, optimal symptom management and reduced premature mortality). The ToC map will be used to form the basis of an evaluative cluster randomized controlled trial.
Conclusions: There have not been any previous studies that have used a ToC approach to develop an integrated multi-modal intervention for renal cachexia patients. Our ToC map will provide an evidence base for such integrated interventions aimed at improving quality of life, optimizing symptom management and reducing premature mortality in patients with renal cachexia.
7-09
TERESA feasibility study (TEstosterone REplacement therapy (TRT) in SArcopenic male colorectal cancer patients): lessons from low recruitment numbers
Ioanna Drami1,2, Dinh Mai1,2, Edward T. Pring2, Harry Dean1,2, Christos Kontovounisios1, Adam Stearns3, Channa Jayasena1 and John T. Jenkins1,2
1Imperial College London, Exhibition Rd, South Kensington, London, UK;2Mark's Hospital and Academic Institute, Central Middlesex, Acton Lane, London, UK;3NHS Foundation Trust, Norfolk and Norwich University Hospital, Norwich, UK
Background: Colorectal cancer is the third most common cancer worldwide (WHO data 2018), with rectum being the most commonly affected site. Cancer, via numerous complicated and not fully elucidated molecular pathways, results in sarcopenia and fatty infiltration of the muscle, known as myosteatosis. Colorectal cancer patients may experience sarcopenia with a prevalence of 25–60%, which increases further in metastatic cases. Sarcopenia and myosteatosis occur during chemotherapy, with sarcopenia occurring more in males compared to females.
Male cancer patients, experience either primary or secondary hypogonadism (prevalence 40–90%). Lower androgenicity has been associated with poor survival in the colorectal cancer population. The study's aim is to assess the recruitment and retention of the patients, the acceptability of the treatment (NCT 05367284).
Material and methods: This is a prospective single arm open label non randomized feasibility study. Recruitment takes place during the patient's diagnosis, if booked straight for an operation, or upon completion of chemoradiotherapy. The eligibility criteria, include colorectal cancer patients above the age of 45 years old, sarcopenic as assessed on their diagnostic or monitoring CT preoperatively, with low testosterone on two separate occasions (12 nmol/L), while their surgery is planned 4–8 weeks from recruitment. The exclusion criteria ensure that the patient will not have any major complications from the use of testosterone treatment and included a PSA > 3 ng/mL, a haematocrit higher than 52%, metastatic disease, treatment for hypogonadism and morbid obesity among others. If patients fulfil the eligibility criteria, they are started on a topical testosterone gel (Testogel pump 16.2 mg/g®), applied once daily for a total of 12 weeks. Patients are assessed at two further points during their treatment with regards to the testosterone levels and treatment acceptability, including quality of life, appetite and fatigue questionnaires.
Results: The study is currently open and recruiting at two UK sites, each with a high volume of rectal cancer patients being treated. Recruitment has been challenging due to the multiple visits from the patients and the multiple blood test to establish hypogonadism.
Conclusions: Our hypothesis is that by normalizing the testosterone level, we are improving their post-surgical outcomes by increasing their muscle mass and optimizing their physiological function. The main outcome of the study is to assess the feasibility of introducing testosterone replacement in the perioperative window. Similar future studies should take into consideration the patient visits during the study design.
7-10
Phase 2 study to assess the efficacy, safety, and tolerability of the GDF-15 inhibitor ponsegromab in patients with cancer cachexia
Jeffrey Crawford1, Shannon L. Lubaczewski2, Anil Tarachandani3, Magdalena A. Harrington4, Yan Weng5, Ruolun Qiu5, Susie M. Collins6, Michelle I. Rossulek7 and James H. Revkin7
1Duke Cancer Institute, Duke University Medical Center, Durham, NC, USA;2Early Clinical Development, Biomedicine Artificial Intelligence, Pfizer Inc, Collegeville, PA, USA;3Early Clinical Development, Pfizer Inc, Cambridge, MA, USA;4Global Access and Value, Pfizer Inc, Cambridge, MA, USA;5Clinical Pharmacology, Pfizer Inc, Cambridge, MA, USA;6Global Biometrics and Data Management, Pfizer R&D UK Ltd, Kent, UK;7Internal Medicine Research Unit, Pfizer Inc, Cambridge, MA, USA
Background: Cancer cachexia is a multifactorial metabolic syndrome of wasting characterized by anorexia, unintended weight loss, and decreased skeletal muscle mass, leading to progressive functional impairment, fatigue, diminished quality of life, poor response to anticancer therapy, and reduced survival. One of the biomarkers associated with cancer cachexia is cytokine growth differentiation factor 15 (GDF-15), which is secreted by tumour cells. Preliminary phase 1 data suggest that suppression of GDF-15 may lead to improvement in cachexia-related symptom burden. Ponsegromab is a potent and selective humanized monoclonal antibody that inhibits GDF-15-mediated signalling. The primary objective of this study (NCT05546476) is to assess the effect of ponsegromab on body weight in patients with cancer, cachexia, and elevated circulating GDF-15 concentrations. Secondary objectives include assessing physical activity, gait, anorexia/appetite, nausea and vomiting, fatigue, and safety. Exploratory objectives include evaluating pharmacokinetics, pharmacodynamics, and immunogenicity.
Trial Design: This phase 2 study will enrol approximately 168 adults with non–small cell lung, pancreatic, or colorectal cancers who have cachexia and elevated GDF-15 concentrations. The study will be conducted in 2 parts. The initial 12-week treatment period will be a randomized, double-blind, placebo-controlled study wherein participants who meet eligibility criteria will be randomized 1:1:1:1 to one of 3 dose groups of ponsegromab (administered subcutaneously [SC] every 4 weeks [Q4W]) or placebo. The double-blind period will be followed by optional open-label treatment (OLT) with ponsegromab Q4W SC for up to 1 year. Upon completion of the optional OLT period, there will be a follow-up visit at Week 72. Participants who do not proceed with the optional OLT period will complete the Week 12 visit and a follow-up visit at Week 16. The primary endpoint is the mean change from baseline in body weight at Week 12. A mixed model for repeated measures followed by a Bayesian Emax model will be used for the primary analysis. Secondary endpoints include physical activity and gait measured by remote digital sensors; patient-reported appetite-related symptoms assessed by Functional Assessment of Anorexia-Cachexia Therapy scores; anorexia/appetite, nausea, vomiting, and fatigue evaluated according to questions from the Cancer-related Cachexia Symptom Diary; and incidence of adverse events, safety laboratory tests, vital signs, and electrocardiogram abnormalities.
Ruxolitinib's nutritional effects in patients with myelofibrosis: preliminary results
Silvia Antonini and Alessio Molfino and Maria Ida Amabile and Emilia Scalzulli and Massimo Breccia and Maurizio Muscaritoli
Department of Translational and Precision Medicine, Sapienza University of Rome, Italy
Introduction: Myelofibrosis (MF) is a chronic myeloproliferative neoplasm that can cause cachexia by inducing systemic inflammatory state (IL-6 and TNF-a) and by reducing nutritional intake due to massive splenomegaly. We aimed at evaluating improvement and modifications of nutritional status in MF patients during ruxolitinib therapy, the first JAK1/2-inhibitor available.
Methods: Before (baseline, T0) and during treatment (3 months, T1; 6 months, T2; 12 months, T3) Malnutrition (GLIM criteria), Anorexia (FAACT score), body composition (BIA) were assessed.
Results: We enrolled 23 MF patients (M:13, mean age 64.7 ± 12.5). At baseline, anorexia, malnutrition and unintentional weight loss, were present in 22%, 50% and 70% of them, respectively. During treatment with ruxolitinib, we observed improvement in body weight (BW, kg) (T0 68.6 ± 14.22; T3 77.3 ± 12.4), fat mass (FM, kg) (from T0 15.8 ± 5.8; to T2 20.3 ± 8.11 and to T3 23.4 ± 7.6) (P = 0.04, P = 0.01, respectively) with preservation of lean body mass (LBM, kg) (T0 52.8 ± 12; T2 52.1 ± 12.1; T3 54.3 ± 12.4) (P > 0.05) and increase of anorexia score for all patients (P = 0.0005) and for anorexic ones (T0 26.2 ± 6.3; T1 37.6 ± 6; T2 39.2 ± 6.2) (P = 0.01), irrespective of disease response to therapy according to IWG criteria (11 patients with clinical improvement, 7 and 3 patients with stable and progressive disease, respectively, 2 not evaluable for recent enrolment).
Conclusions: Our preliminary data show that ruxolitinib is associated with improvement of anorexia score and BW in MF patients. The latter is mainly due to increased FM, and preservation of LBM. These data suggest that ruxolitinib may be associated with benefit in nutritional status and body composition, regardless of clinical response in patients with MF.
7-12
Assessing the effect of intra-abdominal malignancy on the impact of a short-term homebased unsupervised exercise on skeletal muscle mitochondrial OXPHOS function
Thomas Smart1,2, Jacob Hatt1,2, Joseph Bass1, Jon Lund1,2 and Bethan Phillips1,2
1Centre of Metabolism, Aging and Physiology, School of Medicine, University of Nottingham, Royal Derby Hospital Centre, Derby, UK;2Department of Surgery and Anaesthetics, Royal Derby Hospital, Derby, UK
Introduction: Exercise has long been viewed as a potential intervention to combat the declines seen with both sarcopenia and cachexia. Previous studies have shown that 4 weeks of high-intensity interval training improves cardiorespiratory fitness in patients with malignancy, but not all. The underlying physiological response to exercise is not fully understood, but alterations to mitochondrial respiration are thought to play a part. Animal models have demonstrated that mitochondrial function is as a potential causative component of sarcopenia and cachexia, with translational studies less clear.
We hypothesized that malignancy reduced the ability for skeletal muscle mitochondrial function to be altered by an exercise intervention.
Methods: This study was approved by an NHS research ethics committee (IRAS ID: 275264). Male patients awaiting surgery with curative intent for colorectal and prostate cancer, and healthy controls were recruited. Muscle biopsies of vastus lateralis were taken before and after 4-weeks home-based exercise (3×/week). Mitochondrial oxidative phosphorylation (OXPHOS) was analysed using high-resolution respirometry (Oroboros Instruments).
Results: To date there have been 7 healthy volunteers (Age: 68.8 (6.5)) and 12 cancer patients (Age: 65.6 (6.8)) completing the intervention.
Cancer patients had significantly lower maximal coupled (55.62 pmol/(s*mg) vs. 81.38 pmol/(s*mg), P = 0.001) and uncoupled (57.96 pmol/(s*mg) vs. 98.88 pmol/(s*mg), P = 0.006) OXPHOS capacity compared to healthy controls at baseline. Post exercise training there was no significant difference in maximal coupled (55.62 pmol/(s*mg) vs. 75.02 pmol/(s*mg), P > 0.05) and uncoupled (71.38 pmol/(s*mg) vs. 95.26 pmol/(s*mg), P = 0.16) OXPHOS capacity between the two cohorts.
Conclusions: Our study demonstrates that the OXPHOS capacity of skeletal muscle mitochondria is impaired within the cancer cohort studied, this supports the previous animal studies suggesting its role in cancer cachexia.
A short homebased unsupervised exercise programme appears to attenuate the declines in OXPHOS function seen in the cancer cohort. Further work is needed to optimize an exercise intervention, and to assess the impact of varying malignancy type and stage upon mitochondrial function.
7-13
Association between sarcopenia and urinary dysfunction in patients with dysphagia
Hidetaka Wakabayashi1, Shingo Kakehi1, Shinta Nishioka2 and Ryo Momosaki3
1Department of Rehabilitation Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan;2Department of Clinical Nutrition and Food Service, Nagasaki Rehabilitation Hospital, Nagasaki, Japan;3Department of Rehabilitation Medicine, Mie University Graduate School of Medicine, Mie, Japan
Introduction: To investigate the association between sarcopenia and urinary dysfunction in patients with dysphagia.
Methods: A cross-sectional study was conducted on 460 patients registered in the Japanese Sarcopenic Dysphagia Database with no missing data on urinary dysfunction and sarcopenia. Urinary dysfunction was defined as either urinary incontinence or urethral catheter use. Sarcopenia was diagnosed according to the AWGS2019 criteria. The association between urinary dysfunction and sarcopenia, calf circumference, and handgrip strength was assessed in univariate and multivariate analyses. Logistic regression analyses were adjusted for age, sex, facility type (acute care or non-acute care), Charlson co-morbidity index (CCI), and Barthel index.
Results: The mean age was 80.8 ± 10.5 years, with 229 men and 231 women. Two hundred two were in acute care hospitals and 258 in other settings. Sarcopenia was present in 404 (88%) patients. Fifty-four (12%) patients had urinary incontinence and 83 (18%) patients had urethral catheters, resulting in 137 (30%) patients with urinary dysfunction. Median handgrip strength was 12 kg (interquartile range: 6 kg, 19 kg). Median calf circumference was 28 cm (25 cm, 31 cm). Median Food Intake Level Scale (FILS) score was 7 (3, 8). Median Barthel index score was 25 (5, 50). Median CCI was 2 (1, 4). Univariate analysis showed no significant association between sarcopenia and urinary dysfunction (P = 0.440). In contrast, calf circumference (with urinary dysfunction: 27.4 cm, without urinary dysfunction: 28.5 cm, P = 0.006) and handgrip strength (with urinary dysfunction: 9.7 kg, without urinary dysfunction: 14.4 kg, P < 0.001) were significantly associated with urinary dysfunction. Logistic regression analysis showed that sarcopenia (odds ratio: 0.921, 95% confidence interval: 0.435, 1.950) and calf circumference (odds ratio: 0.990, 95% confidence interval: 0.933, 1.050) were not independently associated with urinary dysfunction. On the other hand, handgrip strength was independently associated with urinary dysfunction (odds ratio: 0.968, 95% confidence interval: 0.938, 0.998), with a cut-off value of 10.85 kg (sensitivity 0.598, specificity 0.562, AUC 0.644) in the ROC curve.
Conclusions: Sarcopenia was not significantly associated with urinary dysfunction; however, handgrip strength was significantly associated with urinary dysfunction. The handgrip strength of the patients in this study was significantly lower than the cut-off value for the diagnosis of sarcopenia in the AWGS 2019 criteria. This suggests that lower handgrip strength in patients with sarcopenia may be associated with urinary dysfunction.
期刊介绍:
The Journal of Cachexia, Sarcopenia, and Muscle is a prestigious, peer-reviewed international publication committed to disseminating research and clinical insights pertaining to cachexia, sarcopenia, body composition, and the physiological and pathophysiological alterations occurring throughout the lifespan and in various illnesses across the spectrum of life sciences. This journal serves as a valuable resource for physicians, biochemists, biologists, dieticians, pharmacologists, and students alike.
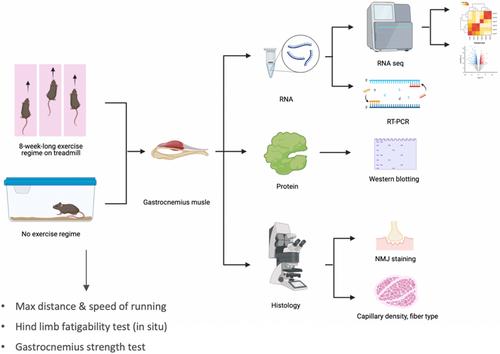


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
