Neighbourhood deprivation, distance to nearest comprehensive stroke centre and access to endovascular thrombectomy for ischemic stroke: a population-based study.
Matthew E Eagles, Reed F Beall, David Ben-Israel, John H Wong, Michael D Hill, Eldon Spackman
{"title":"Neighbourhood deprivation, distance to nearest comprehensive stroke centre and access to endovascular thrombectomy for ischemic stroke: a population-based study.","authors":"Matthew E Eagles, Reed F Beall, David Ben-Israel, John H Wong, Michael D Hill, Eldon Spackman","doi":"10.9778/cmajo.20230046","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endovascular thrombectomy (EVT) has revolutionized ischemic stroke care. We aimed to assess whether neighbourhood socioeconomic status is predictive of access to EVT after receipt of alteplase for ischemic stroke among patients living in Alberta, Canada, and whether this relation is mediated by the distance a person lives to the nearest comprehensive stroke centre (CSC).</p><p><strong>Methods: </strong>We performed a retrospective study including all people older than 18 years living in Alberta who were admitted to hospital with an ischemic stroke and who received intravenous alteplase treatment between Jan. 1, 2017, and Dec. 31, 2019. Data were obtained through administrative data sets. The primary outcome was treatment with EVT. We assigned neighbourhood deprivation quintile based on the Material and Social Deprivation Index. We used logistic regression modelling to assess for a relation between deprivation and treatment with EVT. We adjusted for age, sex, stroke severity and distance to the nearest CSC. We calculated the average causal mediation effect of distance to the nearest CSC on the relation between neighbourhood deprivation level and treatment with EVT.</p><p><strong>Results: </strong>The study cohort consisted of 1335 patients, of whom 181 (13.6%) had missing data and were excluded from the main regression analysis. Endovascular thrombectomy was performed or attempted in 314 patients (23.5%). In the primary model, patients from the most deprived neighbourhoods were less likely than those from less deprived neighbourhoods to have received EVT (adjusted odds ratio 0.43, 95% confidence interval 0.24 to 0.77). Neighbourhood deprivation level was not significantly associated with EVT when distance to the nearest CSC was included as a covariate. Mediation analysis suggested that 48% of the total effect that neighbourhood deprivation level had on the odds of receiving EVT was attributable to the distance a person lived from the nearest CSC.</p><p><strong>Interpretation: </strong>The results suggest that people from more deprived neighbourhoods in Alberta were less likely to be treated with EVT than those from less deprived neighbourhoods. Improving access to EVT for people living in remote locations may improve the equitable distribution of this treatment.</p>","PeriodicalId":93946,"journal":{"name":"CMAJ open","volume":"11 6","pages":"E1181-E1187"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10743637/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20230046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endovascular thrombectomy (EVT) has revolutionized ischemic stroke care. We aimed to assess whether neighbourhood socioeconomic status is predictive of access to EVT after receipt of alteplase for ischemic stroke among patients living in Alberta, Canada, and whether this relation is mediated by the distance a person lives to the nearest comprehensive stroke centre (CSC).
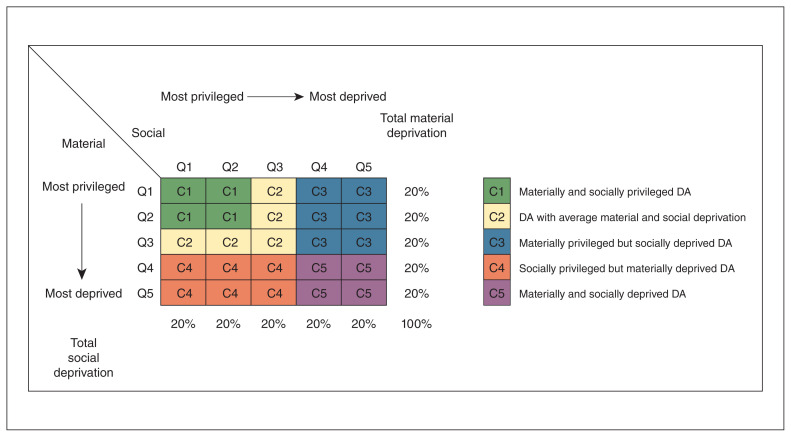
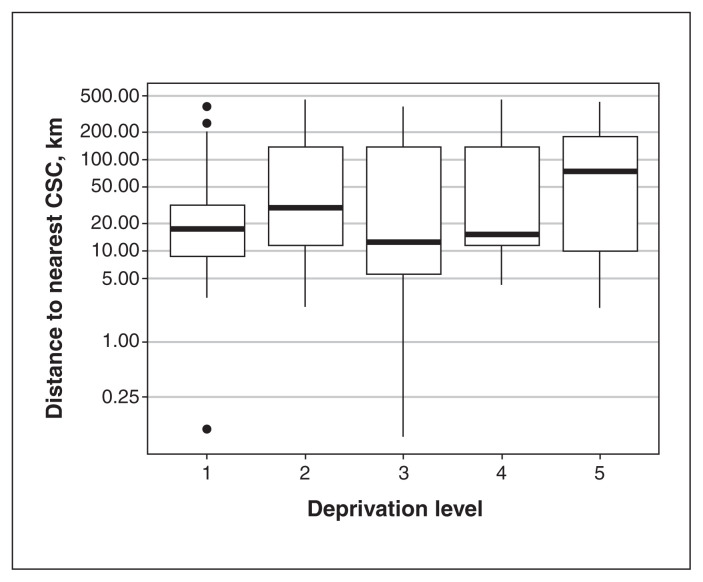
Methods: We performed a retrospective study including all people older than 18 years living in Alberta who were admitted to hospital with an ischemic stroke and who received intravenous alteplase treatment between Jan. 1, 2017, and Dec. 31, 2019. Data were obtained through administrative data sets. The primary outcome was treatment with EVT. We assigned neighbourhood deprivation quintile based on the Material and Social Deprivation Index. We used logistic regression modelling to assess for a relation between deprivation and treatment with EVT. We adjusted for age, sex, stroke severity and distance to the nearest CSC. We calculated the average causal mediation effect of distance to the nearest CSC on the relation between neighbourhood deprivation level and treatment with EVT.
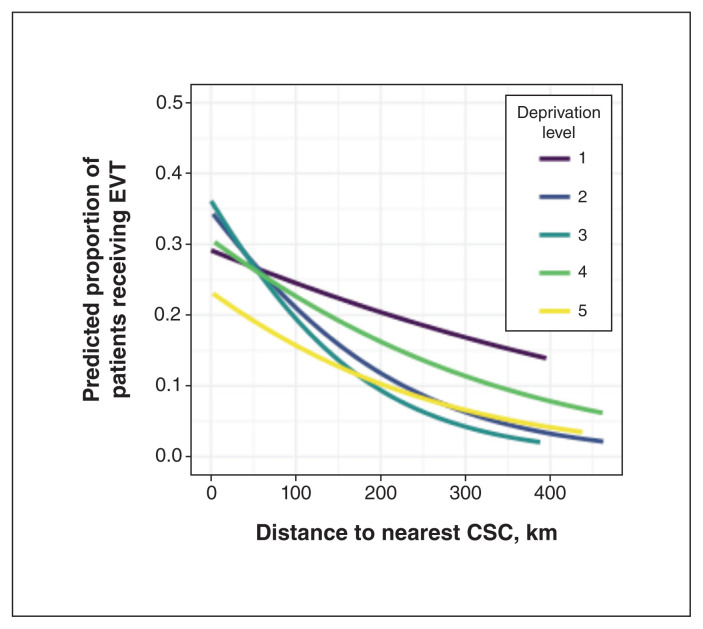
Results: The study cohort consisted of 1335 patients, of whom 181 (13.6%) had missing data and were excluded from the main regression analysis. Endovascular thrombectomy was performed or attempted in 314 patients (23.5%). In the primary model, patients from the most deprived neighbourhoods were less likely than those from less deprived neighbourhoods to have received EVT (adjusted odds ratio 0.43, 95% confidence interval 0.24 to 0.77). Neighbourhood deprivation level was not significantly associated with EVT when distance to the nearest CSC was included as a covariate. Mediation analysis suggested that 48% of the total effect that neighbourhood deprivation level had on the odds of receiving EVT was attributable to the distance a person lived from the nearest CSC.
Interpretation: The results suggest that people from more deprived neighbourhoods in Alberta were less likely to be treated with EVT than those from less deprived neighbourhoods. Improving access to EVT for people living in remote locations may improve the equitable distribution of this treatment.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
