Pieter de Jager, Dionne Aleman, Nancy Baxter, Chaim Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Scott Emerson, Anna Gagliardi, Jonathan Irish, Danielle Martin, Samantha Lee, Marcy Saxe-Braithwaite, Pardis Seyedi, Julie Takata, Suting Yang, Claudia Zanchetta, David Urbach
{"title":"Social determinants of access to timely elective surgery in Ontario, Canada: a cross-sectional population level study.","authors":"Pieter de Jager, Dionne Aleman, Nancy Baxter, Chaim Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Scott Emerson, Anna Gagliardi, Jonathan Irish, Danielle Martin, Samantha Lee, Marcy Saxe-Braithwaite, Pardis Seyedi, Julie Takata, Suting Yang, Claudia Zanchetta, David Urbach","doi":"10.9778/cmajo.20230001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Equitable access to surgical care has clinical and policy implications. We assess the association between social disadvantage and wait times for elective surgical procedures in Ontario.</p><p><strong>Methods: </strong>We conducted a cross-sectional analysis using administrative data sets of adults receiving nonurgent inguinal hernia repair, cholecystectomy, hip arthroplasty, knee arthroplasty, arthroscopy, benign uterine surgery and cataract surgery from April 2013 to December 2019. We assessed the relation between exceeding target wait times and the highest versus lowest quintile of marginalization dimensions by use of generalized estimating equations logistic regression.</p><p><strong>Results: </strong>Of the 1 385 673 procedures included, 174 633 (12.6%) exceeded the target wait time. Adjusted analysis for cataract surgery found significantly increased odds of exceeding wait times for residential instability (adjusted odd ratio [OR] 1.16, 95% confidence interval [CI] 1.11-1.21) and recent immigration (adjusted OR 1.12, 95% CI 1.07-1.18). The highest deprivation quintile was associated with 18% (adjusted OR 1.18, 95% CI 1.12-1.24) and 20% (adjusted OR 1.20, 95% CI 1.12-1.28) increased odds of exceeding wait times for knee and hip arthroplasty, respectively. Residence in areas where higher proportions of residents self-identify as being part of a visible minority group was independently associated with reduced odds of exceeding target wait times for hip arthroplasty (adjusted OR 0.82, 95% CI 0.75-0.91), cholecystectomy (adjusted OR 0.68, 95% CI 0.59-0.79) and hernia repair (adjusted OR 0.65, 95% CI 0.56-0.77) with an opposite effect in benign uterine surgery (adjusted OR 1.28, 95% CI 1.17-1.40).</p><p><strong>Interpretation: </strong>Social disadvantage had a small and inconsistent impact on receiving care within wait time targets. Future research should consider these differences as they relate to resource distribution and the organization of clinical service delivery.</p>","PeriodicalId":93946,"journal":{"name":"CMAJ open","volume":"11 6","pages":"E1164-E1180"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10743664/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20230001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Equitable access to surgical care has clinical and policy implications. We assess the association between social disadvantage and wait times for elective surgical procedures in Ontario.
Methods: We conducted a cross-sectional analysis using administrative data sets of adults receiving nonurgent inguinal hernia repair, cholecystectomy, hip arthroplasty, knee arthroplasty, arthroscopy, benign uterine surgery and cataract surgery from April 2013 to December 2019. We assessed the relation between exceeding target wait times and the highest versus lowest quintile of marginalization dimensions by use of generalized estimating equations logistic regression.
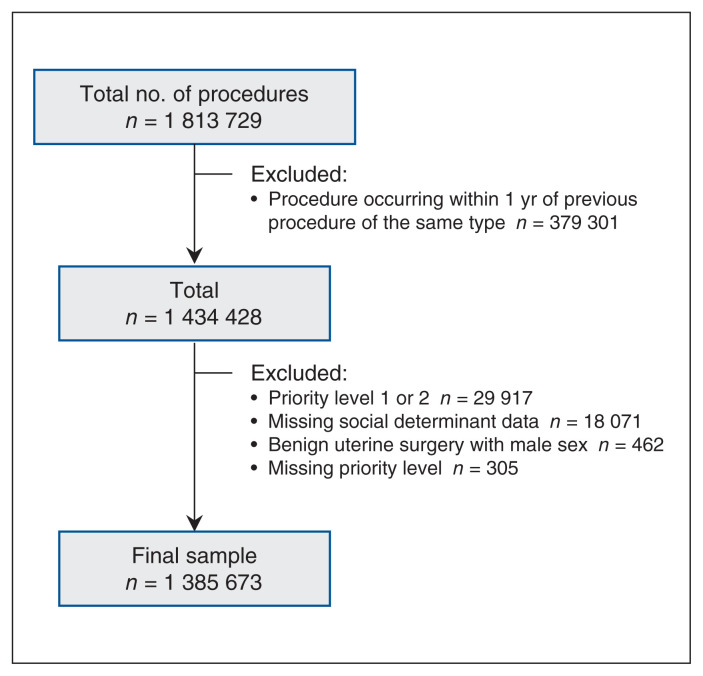
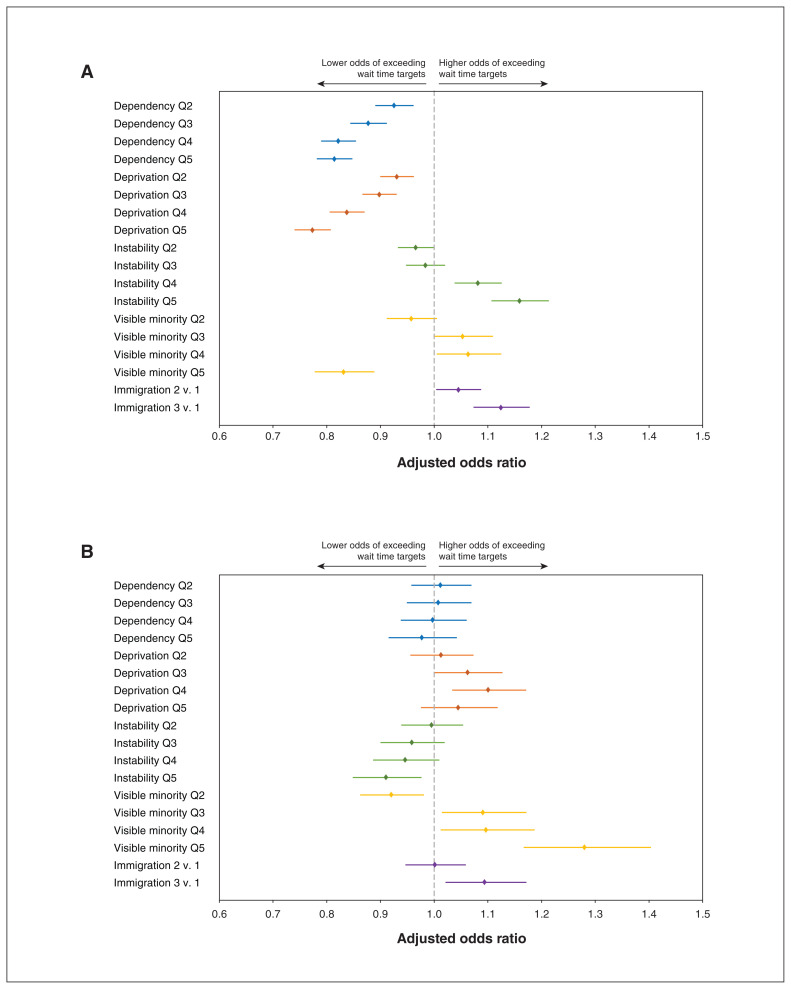
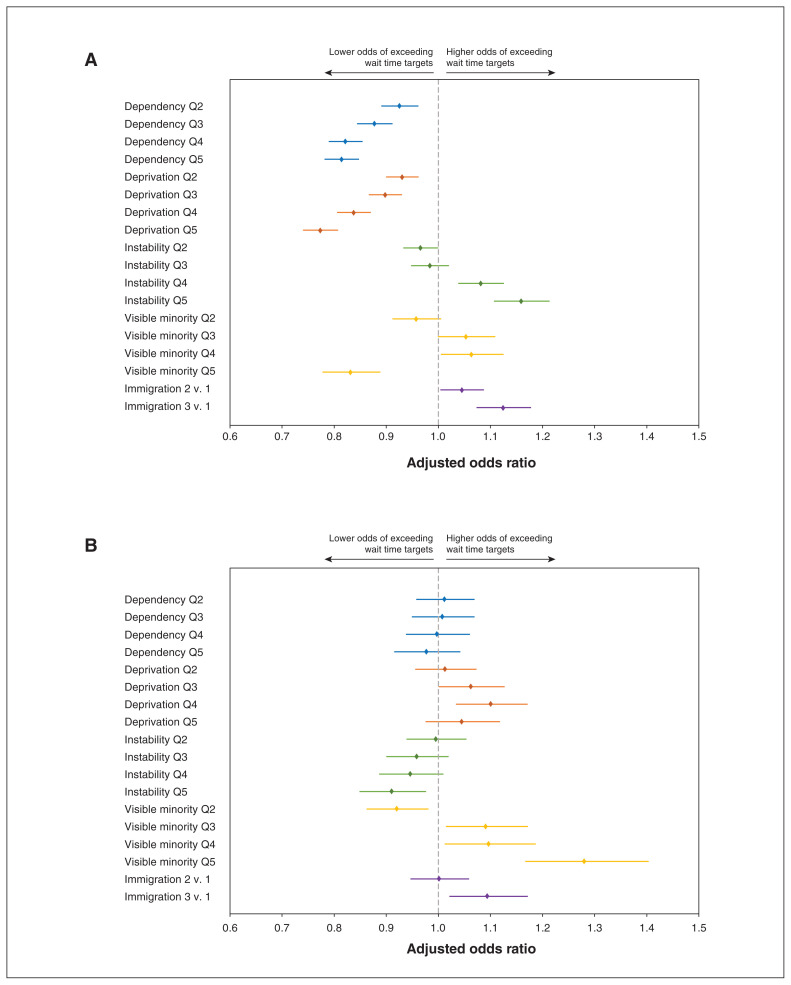
Results: Of the 1 385 673 procedures included, 174 633 (12.6%) exceeded the target wait time. Adjusted analysis for cataract surgery found significantly increased odds of exceeding wait times for residential instability (adjusted odd ratio [OR] 1.16, 95% confidence interval [CI] 1.11-1.21) and recent immigration (adjusted OR 1.12, 95% CI 1.07-1.18). The highest deprivation quintile was associated with 18% (adjusted OR 1.18, 95% CI 1.12-1.24) and 20% (adjusted OR 1.20, 95% CI 1.12-1.28) increased odds of exceeding wait times for knee and hip arthroplasty, respectively. Residence in areas where higher proportions of residents self-identify as being part of a visible minority group was independently associated with reduced odds of exceeding target wait times for hip arthroplasty (adjusted OR 0.82, 95% CI 0.75-0.91), cholecystectomy (adjusted OR 0.68, 95% CI 0.59-0.79) and hernia repair (adjusted OR 0.65, 95% CI 0.56-0.77) with an opposite effect in benign uterine surgery (adjusted OR 1.28, 95% CI 1.17-1.40).
Interpretation: Social disadvantage had a small and inconsistent impact on receiving care within wait time targets. Future research should consider these differences as they relate to resource distribution and the organization of clinical service delivery.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
