Nicholas Weight, Saadiq Moledina, Evangelos Kontopantelis, Harriette Van Spall, Mohammed Dafaalla, Alaide Chieffo, Mario Iannaccone, Denis Chen, Muhammad Rashid, Josepa Mauri-Ferre, Jacqueline E Tamis-Holland, Mamas A Mamas
{"title":"Sex-based analysis of NSTEMI processes of care and outcomes by hospital: a nationwide cohort study.","authors":"Nicholas Weight, Saadiq Moledina, Evangelos Kontopantelis, Harriette Van Spall, Mohammed Dafaalla, Alaide Chieffo, Mario Iannaccone, Denis Chen, Muhammad Rashid, Josepa Mauri-Ferre, Jacqueline E Tamis-Holland, Mamas A Mamas","doi":"10.1093/ehjqcco/qcae011","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contemporary studies demonstrate that non-ST-segment elevation myocardial infarction (NSTEMI) processes of care vary according to sex. Little is known regarding variation in practice between geographical areas and centres.</p><p><strong>Methods: </strong>We identified 305 014 NSTEMI admissions in the United Kingdom (UK) Myocardial Ischaemia National Audit Project (MINAP), 2010-17, including female sex (110 209). Hierarchical, multivariate logistic regression models were fitted, assessing for differences in primary outcomes according to sex. Risk-standardized mortality rates (RSMR) were calculated for individual hospitals to illustrate the correlation with variables of interest. 'Heat maps' were plotted to show regional and sex-based variation in the opportunity-based quality indicator score (surrogate for optimal processes of care).</p><p><strong>Results: </strong>Women presented older (77 years vs. 69 years, P < 0.001) and were more often Caucasian (93% vs. 91%, P < 0.001). Women were less frequently managed with an invasive coronary angiogram (58% vs. 75%, P < 0.001) or percutaneous coronary intervention (35% vs. 49%, P < 0.001). In our hospital-clustered analysis, we show a positive correlation between the RSMR and the increasing proportion of women treated for NSTEMI (R2 = 0.17, P < 0.001). There was a clear negative correlation between the proportion of women who had an optimum OBQI score during their admission and RSMR (R2 = 0.22, P < 0.001), with a weaker correlation in men (R2 = 0.08, P < 0.001). Heat maps according to the Clinical Commissioning Group (CCG) demonstrate significant regional variation in the OBQI score, with women receiving poorer quality care throughout the UK.</p><p><strong>Conclusion: </strong>There was a significant variation in the management of patients with NSTEMI according to sex, with widespread geographical variation. Structural changes are required to enable improved care for women.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"750-762"},"PeriodicalIF":4.6000,"publicationDate":"2024-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656063/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae011","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Contemporary studies demonstrate that non-ST-segment elevation myocardial infarction (NSTEMI) processes of care vary according to sex. Little is known regarding variation in practice between geographical areas and centres.
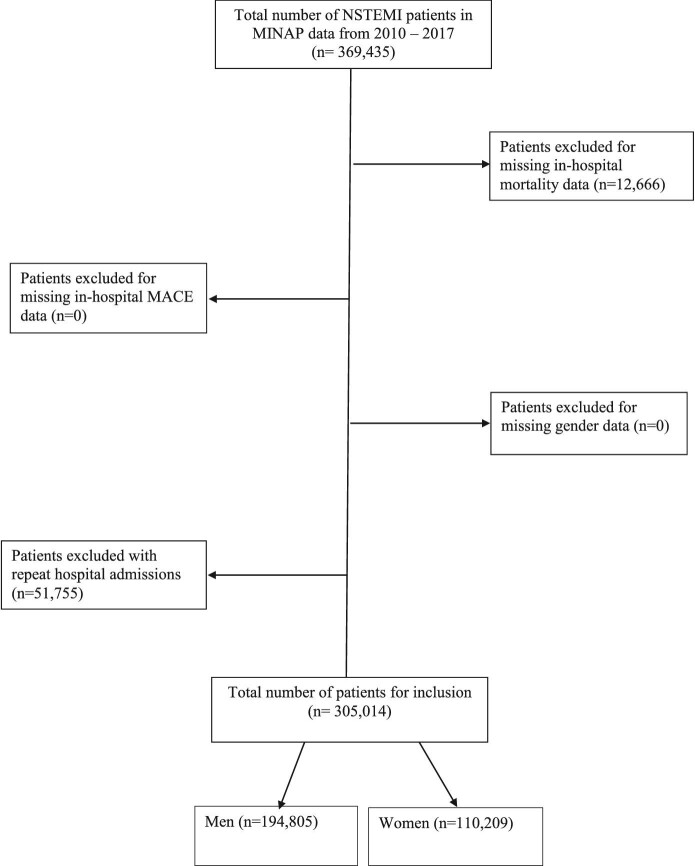
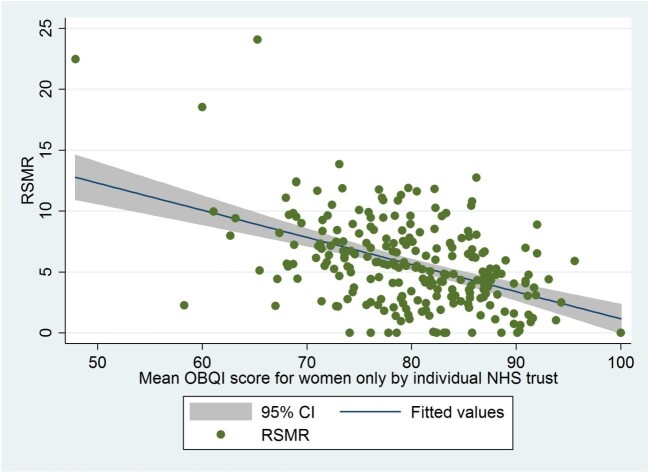
Methods: We identified 305 014 NSTEMI admissions in the United Kingdom (UK) Myocardial Ischaemia National Audit Project (MINAP), 2010-17, including female sex (110 209). Hierarchical, multivariate logistic regression models were fitted, assessing for differences in primary outcomes according to sex. Risk-standardized mortality rates (RSMR) were calculated for individual hospitals to illustrate the correlation with variables of interest. 'Heat maps' were plotted to show regional and sex-based variation in the opportunity-based quality indicator score (surrogate for optimal processes of care).
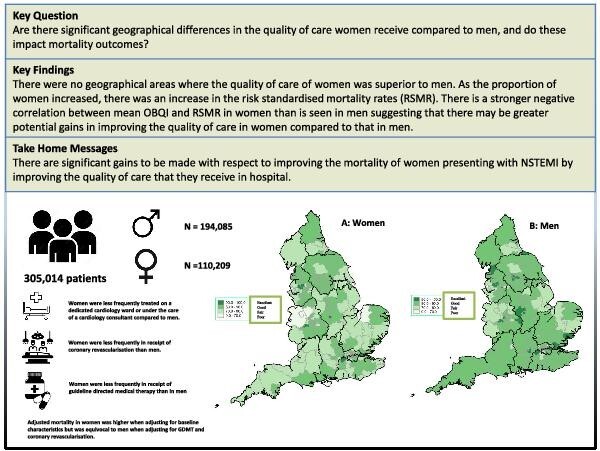
Results: Women presented older (77 years vs. 69 years, P < 0.001) and were more often Caucasian (93% vs. 91%, P < 0.001). Women were less frequently managed with an invasive coronary angiogram (58% vs. 75%, P < 0.001) or percutaneous coronary intervention (35% vs. 49%, P < 0.001). In our hospital-clustered analysis, we show a positive correlation between the RSMR and the increasing proportion of women treated for NSTEMI (R2 = 0.17, P < 0.001). There was a clear negative correlation between the proportion of women who had an optimum OBQI score during their admission and RSMR (R2 = 0.22, P < 0.001), with a weaker correlation in men (R2 = 0.08, P < 0.001). Heat maps according to the Clinical Commissioning Group (CCG) demonstrate significant regional variation in the OBQI score, with women receiving poorer quality care throughout the UK.
Conclusion: There was a significant variation in the management of patients with NSTEMI according to sex, with widespread geographical variation. Structural changes are required to enable improved care for women.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
