Finding sensitive clinical outcome measures has become crucial in natural history studies and therapeutic trials of neuromuscular disorders. Here, we focus on 1-year longitudinal data from quantitative magnetic resonance imaging (MRI) and phosphorus magnetic resonance spectroscopy (31P MRS) in a placebo-controlled study of sirolimus for inclusion body myositis (IBM), also examining their links to functional, strength, and clinical parameters in lower limb muscles.
Quantitative MRI and 31P MRS data were collected at 3 T from a single site, involving 44 patients (22 on placebo, 22 on sirolimus) at baseline and year-1, and 21 healthy controls. Assessments included fat fraction (FF), contractile cross-sectional area (cCSA), and water T2 in global leg and thigh segments, muscle groups, individual muscles, as well as 31P MRS indices in quadriceps or triceps surae. Analyses covered patient-control comparisons, annual change assessments via standard t-tests and linear mixed models, calculation of standardized response means (SRM), and exploration of correlations between MRI, 31P MRS, functional, strength, and clinical parameters.
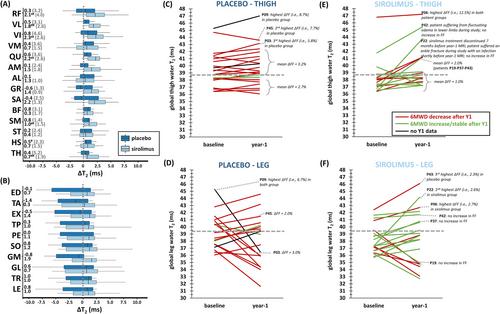
The quadriceps and gastrocnemius medialis muscles had the highest FF values, displaying notable heterogeneity and asymmetry, particularly in the quadriceps. In the placebo group, the median 1-year FF increase in the quadriceps was 3.2% (P < 0.001), whereas in the sirolimus group, it was 0.7% (P = 0.033). Both groups experienced a significant decrease in cCSA in the quadriceps after 1 year (P < 0.001), with median changes of 12.6% for the placebo group and 5.5% for the sirolimus group. Differences in FF and cCSA changes between the two groups were significant (P < 0.001). SRM values for FF and cCSA were 1.3 and 1.4 in the placebo group and 0.5 and 0.8 in the sirolimus group, respectively. Water T2 values were highest in the quadriceps muscles of both groups, significantly exceeding control values in both groups (P < 0.001) and were higher in the placebo group than in the sirolimus group. After treatment, water T2 increased significantly only in the sirolimus group's quadriceps (P < 0.01). Multiple 31P MRS indices were abnormal in patients compared to controls and remained unchanged after treatment. Significant correlations were identified between baseline water T2 and FF at baseline and the change in FF (P < 0.001). Additionally, significant correlations were observed between FF, cCSA, water T2, and functional and strength outcome measures.
This study has demonstrated that quantitative MRI/31P MRS can discern measurable differences between placebo and sirolimus-treated IBM patients, offering promise for future therapeutic trials in idiopathic inflammatory myopathies such as IBM.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
