{"title":"Aortic annular enlargement with Y-incision/rectangular patch.","authors":"Bo Yang","doi":"10.21037/acs-2023-aae-0151","DOIUrl":null,"url":null,"abstract":"<p><p>The Y-incision/rectangular patch aortic annular enlargement (Y-incision AAE) is our go-to technique for aortic annular/root enlargement at the University of Michigan for its simplicity and effectiveness. A complete aortotomy is used for first-time surgical aortic valve replacements (SAVRs), and a partial aortotomy is frequently used in reoperative SAVR. The Y-incision is made through the left-non commissure, underneath the aortic annulus to the left and right fibrous trigones. A rectangular patch is sewn to the aorto-mitral curtain from the left fibrous trigone to the right fibrous trigone and transitioned to the aortic annulus on both sides. The enlarged aortic annulus/root is sized with the valve-shape end of the sizer, and the largest size that can touch all three nadirs of the aortic annulus with one strut facing the left-right commissure is chosen. The non-pledgetted valve sutures are placed in a non-everting suture fashion on the aortic annulus, and inside-outside-inside on the patch. The sutures at the nadir of the non-coronary sinus and left coronary sinus are tied first. The proximal ascending aorta is enlarged with a posterior longitudinal aortotomy, and the distal end of the patch is trimmed to a triangular shape to facilitate the closure of the aortotomy with the \"Roof\" technique. In the 142 consecutives cases, the median size of prosthetic valve used was 29 and upsizing was 3-4 valve sizes. Outcomes included one death, one stroke, two pacemaker implantations for complete heart block including one case of aortic valve endocarditis with Gerbode fistula, and no reoperation for post-operative bleeding. The median aortic valve mean gradient was 7 mmHg and aortic valve area was 2.4 cm<sup>2</sup> two years after SAVR. The median left ventricular mass index regression was 41% in 12-24 months in patients with moderate/severe aortic stenosis.</p>","PeriodicalId":8067,"journal":{"name":"Annals of cardiothoracic surgery","volume":"13 3","pages":"294-302"},"PeriodicalIF":3.1000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11148751/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of cardiothoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/acs-2023-aae-0151","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
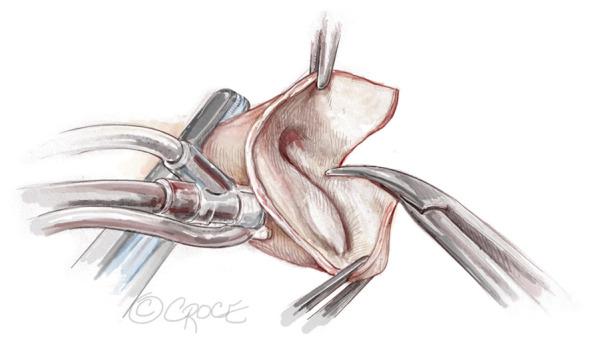
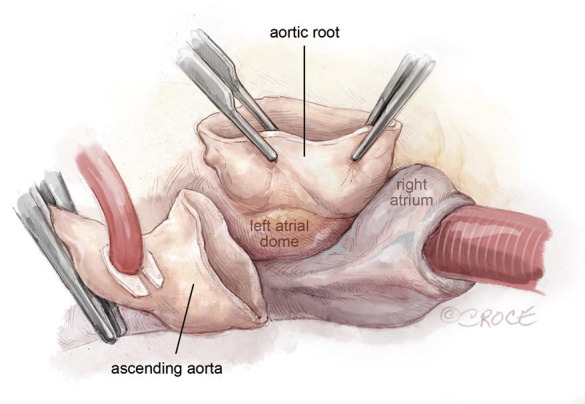
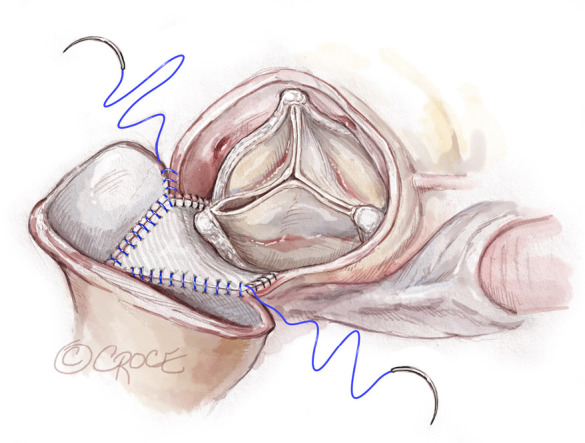
The Y-incision/rectangular patch aortic annular enlargement (Y-incision AAE) is our go-to technique for aortic annular/root enlargement at the University of Michigan for its simplicity and effectiveness. A complete aortotomy is used for first-time surgical aortic valve replacements (SAVRs), and a partial aortotomy is frequently used in reoperative SAVR. The Y-incision is made through the left-non commissure, underneath the aortic annulus to the left and right fibrous trigones. A rectangular patch is sewn to the aorto-mitral curtain from the left fibrous trigone to the right fibrous trigone and transitioned to the aortic annulus on both sides. The enlarged aortic annulus/root is sized with the valve-shape end of the sizer, and the largest size that can touch all three nadirs of the aortic annulus with one strut facing the left-right commissure is chosen. The non-pledgetted valve sutures are placed in a non-everting suture fashion on the aortic annulus, and inside-outside-inside on the patch. The sutures at the nadir of the non-coronary sinus and left coronary sinus are tied first. The proximal ascending aorta is enlarged with a posterior longitudinal aortotomy, and the distal end of the patch is trimmed to a triangular shape to facilitate the closure of the aortotomy with the "Roof" technique. In the 142 consecutives cases, the median size of prosthetic valve used was 29 and upsizing was 3-4 valve sizes. Outcomes included one death, one stroke, two pacemaker implantations for complete heart block including one case of aortic valve endocarditis with Gerbode fistula, and no reoperation for post-operative bleeding. The median aortic valve mean gradient was 7 mmHg and aortic valve area was 2.4 cm2 two years after SAVR. The median left ventricular mass index regression was 41% in 12-24 months in patients with moderate/severe aortic stenosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
