Michaël Cordey, Sophia Chatelard, Daniel Widmer, Patrick Ouvrard, Lilli Herzig
{"title":"Ordinary defensive medicine: in the shadows of general practitioners' postures toward (over-)medicalisation.","authors":"Michaël Cordey, Sophia Chatelard, Daniel Widmer, Patrick Ouvrard, Lilli Herzig","doi":"10.1186/s13010-024-00160-0","DOIUrl":null,"url":null,"abstract":"<p><p>This paper draws on qualitative research using focus groups involving 38 general practitioners (GPs). It explores their attitudes and feelings about (over-)medicalisation. Our main findings were that GPs had a complex representation of (over-)medicalisation, composed of many professional, social, technological, economic and relational issues. This representation led GPs to feel uncomfortable. They felt pressure from all sides, which led them to question their social roles and responsibilities. We identified four main GP-driven proposals to deal with (over-)medicalisation: (1) focusing on the communication in doctor-patient relationships; (2) grounding practices in evidence-based medicine; (3) relying on clinical skills, experience and intuition; and (4) promoting training, leadership bodies and social movements. Drawing on these proposals, we identify and discuss five paradigms that underpin GPs' attitudes toward (over-)medicalisation: underlying social factors, preventing medicalisation, managing uncertainties, sharing medical decision-making and thinking about care as a rationale. We suggest that these paradigms constitute a defensive posture against GPs' uncomfortable feelings. All five defensive paradigms were identified in our focus groups, echoing contemporary political debates on public health. This non-exhaustive framework forms the outline of what we call ordinary defensive medicine. GPs' uncomfortable feelings are the origin of their defensive solutions and the manifestation of their vulnerability. This professional vulnerability can be shared with the patient's vulnerability. In our view, this creates an opportunity to rediscover patient-doctor relationships and examine patients' and doctors' vulnerabilities together.\"There are many cases in which-though the signs of a confusion of tongues between the patient and his doctor are painfully present-there is apparently no open controversy. Some of these cases demonstrate the working of two other, often interlinked, factors. One is the patient's increasing anxiety and despair, resulting in more and more fervently clamouring demands for help. Often the doctor's response is guilt feelings and despair that his most conscientious, most carefully devised examinations do not seem to throw real light on the patient's \"illness\", that his most erudite, most modern, most circumspect therapy does not bring real relief.\" (Balint M. The Doctor, His Patient and the Illness. New York: International Universities; 2005. [1957].)\"Theories about care put an unprecedented emphasis on vulnerability-taking up that challenge to transform what really counts in today's hospitals implies letting colleagues inside previously closely guarded professional boundaries\" (2, our translation).</p>","PeriodicalId":56062,"journal":{"name":"Philosophy Ethics and Humanities in Medicine","volume":"19 1","pages":"10"},"PeriodicalIF":1.9000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11251099/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Philosophy Ethics and Humanities in Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13010-024-00160-0","RegionNum":4,"RegionCategory":"哲学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ETHICS","Score":null,"Total":0}
引用次数: 0
Abstract
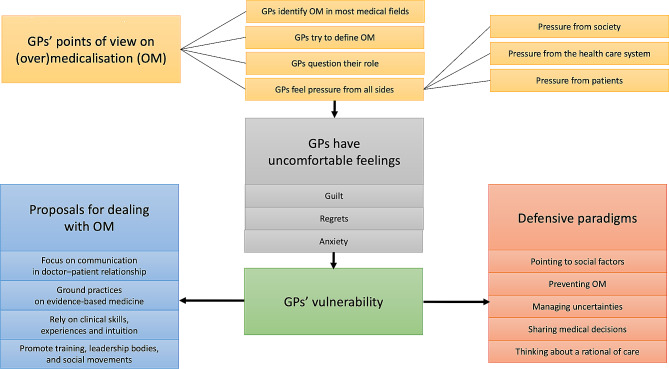
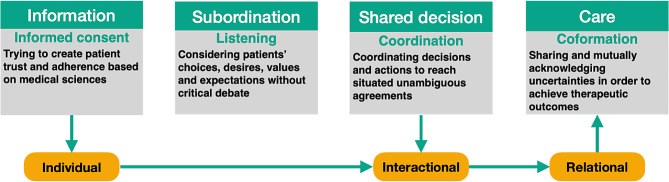
This paper draws on qualitative research using focus groups involving 38 general practitioners (GPs). It explores their attitudes and feelings about (over-)medicalisation. Our main findings were that GPs had a complex representation of (over-)medicalisation, composed of many professional, social, technological, economic and relational issues. This representation led GPs to feel uncomfortable. They felt pressure from all sides, which led them to question their social roles and responsibilities. We identified four main GP-driven proposals to deal with (over-)medicalisation: (1) focusing on the communication in doctor-patient relationships; (2) grounding practices in evidence-based medicine; (3) relying on clinical skills, experience and intuition; and (4) promoting training, leadership bodies and social movements. Drawing on these proposals, we identify and discuss five paradigms that underpin GPs' attitudes toward (over-)medicalisation: underlying social factors, preventing medicalisation, managing uncertainties, sharing medical decision-making and thinking about care as a rationale. We suggest that these paradigms constitute a defensive posture against GPs' uncomfortable feelings. All five defensive paradigms were identified in our focus groups, echoing contemporary political debates on public health. This non-exhaustive framework forms the outline of what we call ordinary defensive medicine. GPs' uncomfortable feelings are the origin of their defensive solutions and the manifestation of their vulnerability. This professional vulnerability can be shared with the patient's vulnerability. In our view, this creates an opportunity to rediscover patient-doctor relationships and examine patients' and doctors' vulnerabilities together."There are many cases in which-though the signs of a confusion of tongues between the patient and his doctor are painfully present-there is apparently no open controversy. Some of these cases demonstrate the working of two other, often interlinked, factors. One is the patient's increasing anxiety and despair, resulting in more and more fervently clamouring demands for help. Often the doctor's response is guilt feelings and despair that his most conscientious, most carefully devised examinations do not seem to throw real light on the patient's "illness", that his most erudite, most modern, most circumspect therapy does not bring real relief." (Balint M. The Doctor, His Patient and the Illness. New York: International Universities; 2005. [1957].)"Theories about care put an unprecedented emphasis on vulnerability-taking up that challenge to transform what really counts in today's hospitals implies letting colleagues inside previously closely guarded professional boundaries" (2, our translation).
期刊介绍:
Philosophy, Ethics, and Humanities in Medicine considers articles on the philosophy of medicine and biology, and on ethical aspects of clinical practice and research.
Philosophy, Ethics, and Humanities in Medicine is an open access, peer-reviewed online journal that encompasses all aspects of the philosophy of medicine and biology, and the ethical aspects of clinical practice and research. It also considers papers at the intersection of medicine and humanities, including the history of medicine, that are relevant to contemporary philosophy of medicine and bioethics.
Philosophy, Ethics, and Humanities in Medicine is the official publication of the Pellegrino Center for Clinical Bioethics at Georgetown University Medical Center.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
