Fernando Duarte, João Neves Silva, Carina Ramos, Colin Hopper
{"title":"Anatomic and functional masseter muscle adaptation following orthognathic surgery-MRI analysis in 3 years of follow-up.","authors":"Fernando Duarte, João Neves Silva, Carina Ramos, Colin Hopper","doi":"10.1186/s40902-024-00437-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Orthodontic and surgical technical advances in recent years have resulted in treatment opportunities for a whole range of craniofacial skeletal disorders either in the adolescent or adult patient. In the growing child, these can include myofunctional orthodontic appliance therapy or distraction osteogenesis procedures, while in the adult, the mainstay approach revolves around orthognathic surgery. The literature agrees that for a change in craniofacial morphology to remain stable, the muscles acting upon the facial skeleton must be capable of adaptation in their structure and, therefore, their function. Failure of the muscles to adapt to the change in their length or orientation will place undesirable forces on the muscle attachments leading to potential instability of the skeleton. Adaptation can occur through various processes including those within the neuromuscular feedback mechanism, through changes within muscle structure or through altered muscle physiology, and through changes at the muscle/bone interface. It is now accepted that because there is no single method of assessing masticatory function, several measures should be taken, and whenever possible, simultaneously.</p><p><strong>Methods: </strong>This investigation was designed to apply several, newly developed and more sophisticated methods of measuring muscle structure and function to a situation where adaptation of muscle is pivotal to the success of a therapeutic approach. Patients attending the combined orthodontic/orthognathic surgery clinic at the Clitrofa - Centro Médico, Dentário e Cirúrgico, in Trofa, Portugal, were screened. Ten patients scheduled for a bimaxillary osteotomy involving a combination of maxillary Le Fort I impaction procedure coupled with a sagittal split advancement of the mandible were selected to form the study group. The patients have MRI of the masseter muscle to evaluate the masseter muscle volume and fibre orientation changes. This exam was taken before surgery (T0), 6 to 12 months after surgery (T1), and 3 years after surgery (T2), by two independent observers, according to the protocol jointly developed between the Eastman Dental Institute - University of London and the MRI Centre - Department of Radiology at John Radcliffe Hospital - University of Oxford.</p><p><strong>Results: </strong>Significant differences (p < 0.05) have been identified between Time 0 (pre-op) and Time 1 (6-12 months post-op) regarding the masseter area (mm<sup>2</sup>). The differences against Time 0 (pre-op) seem to disappear at Time 2 (3 years post-op).</p><p><strong>Conclusions: </strong>MRI therefore seems to be a valid tool for measuring differences in the masseter muscle area and volume associated with high-severity occlusal deformities, although showing not to be as efficient in detecting the same differences in cases of low-severity occlusal deformities.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"46 1","pages":"26"},"PeriodicalIF":2.8000,"publicationDate":"2024-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11258114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-024-00437-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Orthodontic and surgical technical advances in recent years have resulted in treatment opportunities for a whole range of craniofacial skeletal disorders either in the adolescent or adult patient. In the growing child, these can include myofunctional orthodontic appliance therapy or distraction osteogenesis procedures, while in the adult, the mainstay approach revolves around orthognathic surgery. The literature agrees that for a change in craniofacial morphology to remain stable, the muscles acting upon the facial skeleton must be capable of adaptation in their structure and, therefore, their function. Failure of the muscles to adapt to the change in their length or orientation will place undesirable forces on the muscle attachments leading to potential instability of the skeleton. Adaptation can occur through various processes including those within the neuromuscular feedback mechanism, through changes within muscle structure or through altered muscle physiology, and through changes at the muscle/bone interface. It is now accepted that because there is no single method of assessing masticatory function, several measures should be taken, and whenever possible, simultaneously.
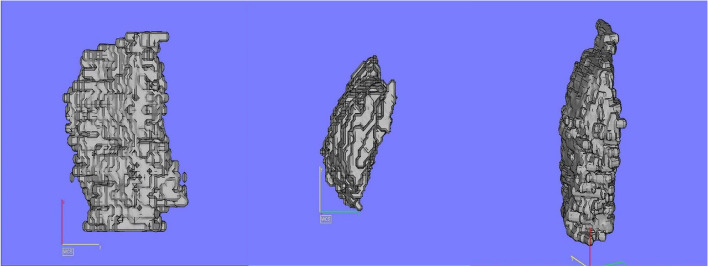
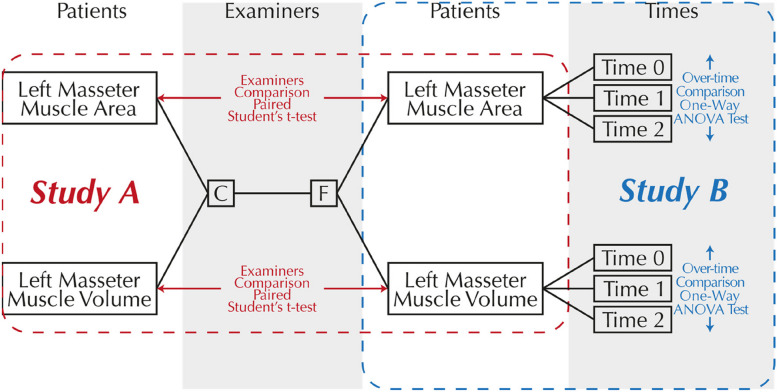
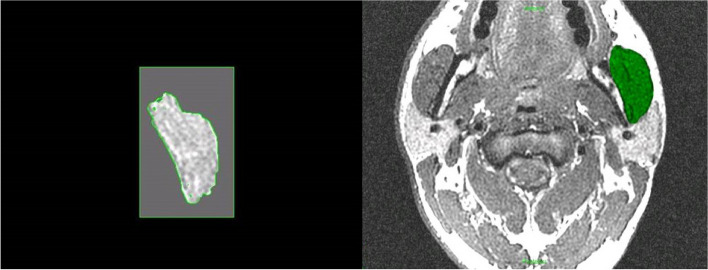
Methods: This investigation was designed to apply several, newly developed and more sophisticated methods of measuring muscle structure and function to a situation where adaptation of muscle is pivotal to the success of a therapeutic approach. Patients attending the combined orthodontic/orthognathic surgery clinic at the Clitrofa - Centro Médico, Dentário e Cirúrgico, in Trofa, Portugal, were screened. Ten patients scheduled for a bimaxillary osteotomy involving a combination of maxillary Le Fort I impaction procedure coupled with a sagittal split advancement of the mandible were selected to form the study group. The patients have MRI of the masseter muscle to evaluate the masseter muscle volume and fibre orientation changes. This exam was taken before surgery (T0), 6 to 12 months after surgery (T1), and 3 years after surgery (T2), by two independent observers, according to the protocol jointly developed between the Eastman Dental Institute - University of London and the MRI Centre - Department of Radiology at John Radcliffe Hospital - University of Oxford.
Results: Significant differences (p < 0.05) have been identified between Time 0 (pre-op) and Time 1 (6-12 months post-op) regarding the masseter area (mm2). The differences against Time 0 (pre-op) seem to disappear at Time 2 (3 years post-op).
Conclusions: MRI therefore seems to be a valid tool for measuring differences in the masseter muscle area and volume associated with high-severity occlusal deformities, although showing not to be as efficient in detecting the same differences in cases of low-severity occlusal deformities.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
