{"title":"Challenges in nasal reconstruction for facial clefts Tessier 3 bilateral and Tessier 0: a staged surgical approach case report.","authors":"Arif Tri Prasetyo","doi":"10.1186/s40902-025-00461-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Craniofacial anomalies, particularly Tessier facial clefts, present significant surgical and functional challenges. Bilateral Tessier 3 and Tessier 0 clefts are extremely rare, often requiring complex reconstructive strategies. These clefts result in severe nasal deformities, including absent nasal septum, hypertelorism, and malpositioned alae nasi, affecting both appearance and function. Due to the lack of standardized approaches in such cases, this report highlights a staged surgical reconstruction aimed at restoring nasal structure and improving facial harmony, with a 12-month follow-up showing stable nasal contour and functional airway restoration.</p><p><strong>Case presentation: </strong>A 16-year-old female presented with bilateral Tessier 3 and Tessier 0 clefts, exhibiting hypertelorism, a wide nasal dorsum, cranial displacement of the alae nasi, and an absent nasal septum. The patient underwent staged reconstruction. The first stage repositioned the alae nasi and created a functional nasal airway. In the second stage, costal cartilage was used to construct an L-shaped septal extension graft and dorsal onlay graft to restore nasal contour and stability. A subsequent procedure refined the nasal dorsum and approximated the alae nasi. Although orbital box osteotomy was planned to correct hypertelorism, the patient declined further intervention.</p><p><strong>Conclusion: </strong>This case highlights the effectiveness of a staged reconstructive approach in addressing rare craniofacial anomalies. Twelve-month postoperative follow-up confirmed the stability of nasal contour, functional airway patency, and satisfactory facial symmetry. The decision to forgo orbital box osteotomy emphasizes the role of patient-centered care in craniofacial surgery. This case provides valuable insights for optimizing reconstructive techniques in complex facial clefts.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"47 1","pages":"7"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11914444/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-025-00461-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Craniofacial anomalies, particularly Tessier facial clefts, present significant surgical and functional challenges. Bilateral Tessier 3 and Tessier 0 clefts are extremely rare, often requiring complex reconstructive strategies. These clefts result in severe nasal deformities, including absent nasal septum, hypertelorism, and malpositioned alae nasi, affecting both appearance and function. Due to the lack of standardized approaches in such cases, this report highlights a staged surgical reconstruction aimed at restoring nasal structure and improving facial harmony, with a 12-month follow-up showing stable nasal contour and functional airway restoration.
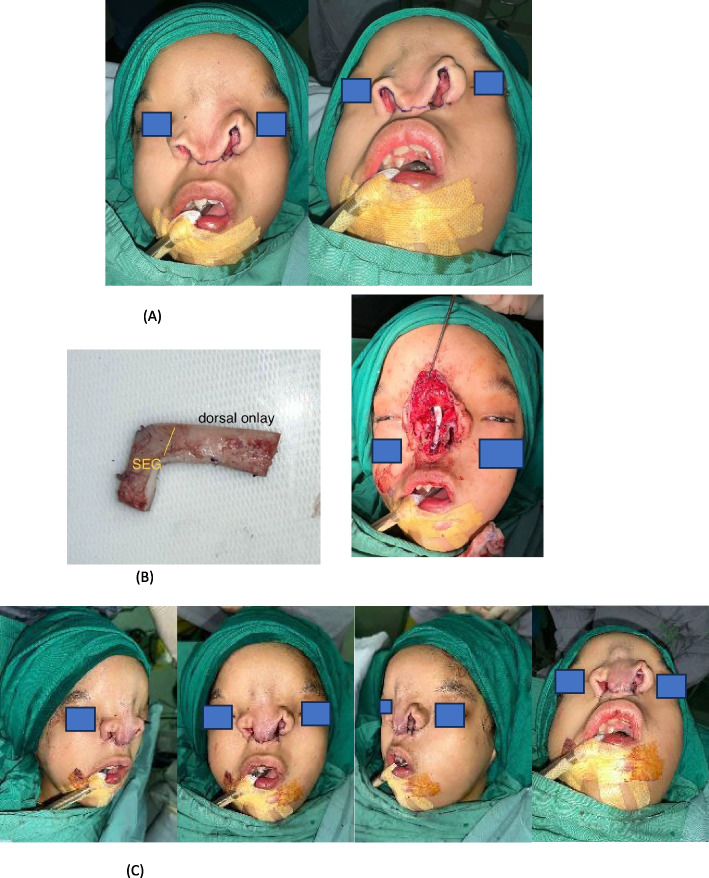
Case presentation: A 16-year-old female presented with bilateral Tessier 3 and Tessier 0 clefts, exhibiting hypertelorism, a wide nasal dorsum, cranial displacement of the alae nasi, and an absent nasal septum. The patient underwent staged reconstruction. The first stage repositioned the alae nasi and created a functional nasal airway. In the second stage, costal cartilage was used to construct an L-shaped septal extension graft and dorsal onlay graft to restore nasal contour and stability. A subsequent procedure refined the nasal dorsum and approximated the alae nasi. Although orbital box osteotomy was planned to correct hypertelorism, the patient declined further intervention.
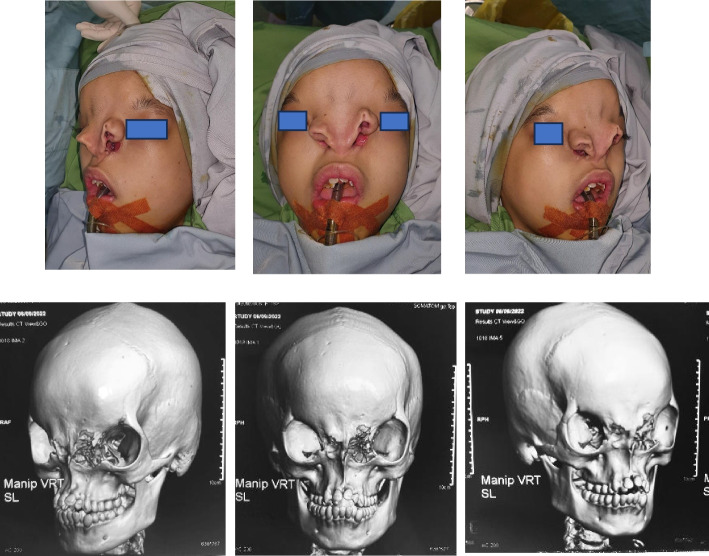
Conclusion: This case highlights the effectiveness of a staged reconstructive approach in addressing rare craniofacial anomalies. Twelve-month postoperative follow-up confirmed the stability of nasal contour, functional airway patency, and satisfactory facial symmetry. The decision to forgo orbital box osteotomy emphasizes the role of patient-centered care in craniofacial surgery. This case provides valuable insights for optimizing reconstructive techniques in complex facial clefts.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
