Rafael N Miranda, Peter C Austin, Stephen E Fremes, Mamas A Mamas, Maneesh K Sud, David M J Naimark, Harindra C Wijeysundera
{"title":"Wait-times benchmarks for risk-based prioritization in transcatheter aortic valve implantation: a simulation study.","authors":"Rafael N Miranda, Peter C Austin, Stephen E Fremes, Mamas A Mamas, Maneesh K Sud, David M J Naimark, Harindra C Wijeysundera","doi":"10.1093/ehjqcco/qcae059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Demand for transcatheter aortic valve implantation (TAVI) has increased in the last decade, resulting in prolonged wait-times and undesirable health outcomes in many health systems. Risk-based prioritization and wait-times benchmarks can improve equitable access to patients.</p><p><strong>Methods and results: </strong>We used simulation models to follow-up a synthetic population of 50 000 individuals from referral to completion of TAVI. Based on their risk of adverse events, patients could be classified as 'low-', 'medium-', and 'high-risk', and shorter wait-times were assigned for the higher risk groups. We assessed the impacts of the size and wait-times for each risk group on waitlist mortality, hospitalization, and urgent TAVIs. All scenarios had the same resource constraints, allowing us to explore the trade-offs between faster access for prioritized patients and deferred access for non-prioritized groups. Increasing the proportion of patients categorized as high-risk, and providing more rapid access to the higher-risk groups achieved the greatest reductions in mortality, hospitalizations and urgent TAVIs (relative reductions of up to 29%, 23%, and 38%, respectively). However, this occurs at the expense of excessive wait-times in the non-prioritized low-risk group (up to 25 weeks). We propose wait-times of up to 3 weeks for high-risk patients and 7 weeks for medium-risk patients.</p><p><strong>Conclusion: </strong>Prioritizing higher-risk patients with faster access leads to better health outcomes, however this also results in unacceptably long wait-times for the non-prioritized groups in settings with limited capacity. Decision-makers must be aware of these implications when developing and implementing waitlist prioritization strategies.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"10-18"},"PeriodicalIF":4.6000,"publicationDate":"2025-01-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11736150/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae059","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Demand for transcatheter aortic valve implantation (TAVI) has increased in the last decade, resulting in prolonged wait-times and undesirable health outcomes in many health systems. Risk-based prioritization and wait-times benchmarks can improve equitable access to patients.
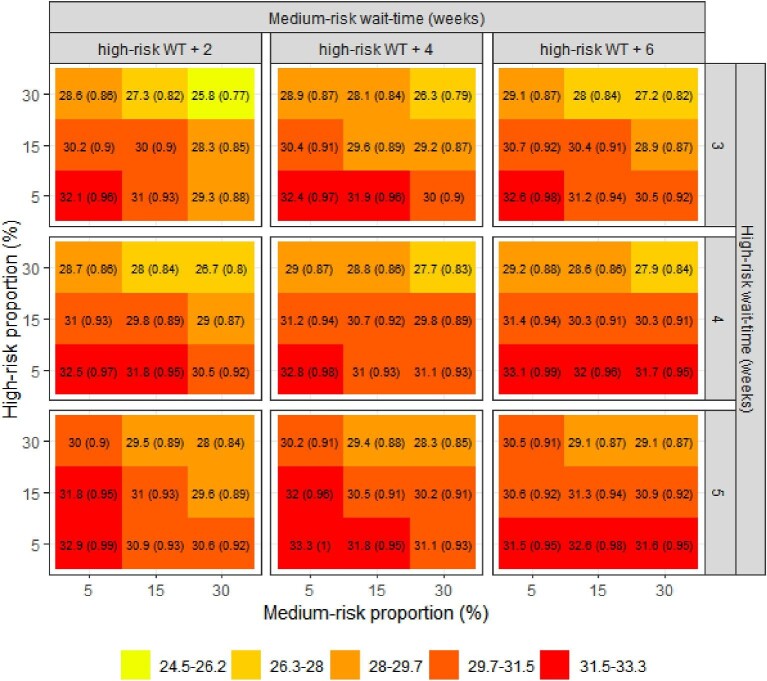
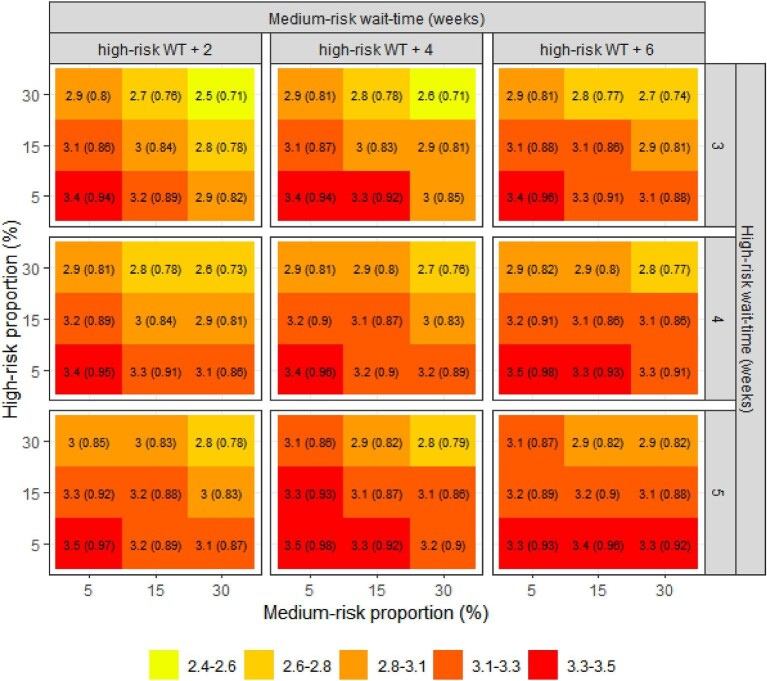
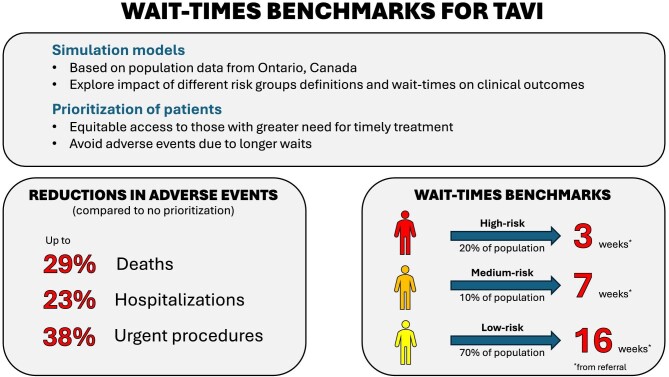
Methods and results: We used simulation models to follow-up a synthetic population of 50 000 individuals from referral to completion of TAVI. Based on their risk of adverse events, patients could be classified as 'low-', 'medium-', and 'high-risk', and shorter wait-times were assigned for the higher risk groups. We assessed the impacts of the size and wait-times for each risk group on waitlist mortality, hospitalization, and urgent TAVIs. All scenarios had the same resource constraints, allowing us to explore the trade-offs between faster access for prioritized patients and deferred access for non-prioritized groups. Increasing the proportion of patients categorized as high-risk, and providing more rapid access to the higher-risk groups achieved the greatest reductions in mortality, hospitalizations and urgent TAVIs (relative reductions of up to 29%, 23%, and 38%, respectively). However, this occurs at the expense of excessive wait-times in the non-prioritized low-risk group (up to 25 weeks). We propose wait-times of up to 3 weeks for high-risk patients and 7 weeks for medium-risk patients.
Conclusion: Prioritizing higher-risk patients with faster access leads to better health outcomes, however this also results in unacceptably long wait-times for the non-prioritized groups in settings with limited capacity. Decision-makers must be aware of these implications when developing and implementing waitlist prioritization strategies.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
