Austin S. Kilaru MD MSHP, Joshua M. Liao MD MSc, Erkuan Wang MA, Yueming Zhao MPH, Jingsan Zhu MS MBA, Grace Ng MD MSHP, Torrey Shirk BA, Deborah S. Cousins MSPH, Genevieve P. Kanter PhD, Said Ibrahim MD MPH MBA, Amol S. Navathe MD PhD
{"title":"Association between mandatory bundled payments and changes in socioeconomic disparities for joint replacement outcomes","authors":"Austin S. Kilaru MD MSHP, Joshua M. Liao MD MSc, Erkuan Wang MA, Yueming Zhao MPH, Jingsan Zhu MS MBA, Grace Ng MD MSHP, Torrey Shirk BA, Deborah S. Cousins MSPH, Genevieve P. Kanter PhD, Said Ibrahim MD MPH MBA, Amol S. Navathe MD PhD","doi":"10.1111/1475-6773.14369","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To determine whether mandatory participation by hospitals in bundled payments for lower extremity joint replacement (LEJR) was associated with changes in outcome disparities for patients dually eligible for Medicare and Medicaid.</p>\n </section>\n \n <section>\n \n <h3> Data Sources and Study Setting</h3>\n \n <p>We used Medicare claims data for beneficiaries undergoing LEJR in the United States between 2011 and 2017.</p>\n </section>\n \n <section>\n \n <h3> Study Design</h3>\n \n <p>We conducted a retrospective observational study using a differences-in-differences method to compare changes in outcome disparities between dual-eligible and non-dual eligible beneficiaries after hospital participation in the Comprehensive Care for Joint Replacement (CJR) program. The primary outcome was LEJR complications. Secondary outcomes included 90-day readmissions and mortality.</p>\n </section>\n \n <section>\n \n <h3> Data Extraction Methods</h3>\n \n <p>We identified hospitals in the US market areas eligible for CJR. We included beneficiaries in the intervention group who received joint replacement at hospitals in markets randomized to participate in CJR. The comparison group included patients who received joint replacement at hospitals in markets who were eligible for CJR but randomized to control.</p>\n </section>\n \n <section>\n \n <h3> Principal Findings</h3>\n \n <p>The study included 1,603,555 Medicare beneficiaries (mean age, 74.6 years, 64.3% women, 11.0% dual-eligible). Among participant hospitals, complications decreased between baseline and intervention periods from 11.0% to 10.1% for dual-eligible and 7.0% to 6.4% for non-dual-eligible beneficiaries. Among nonparticipant hospitals, complications decreased from 10.3% to 9.8% for dual-eligible and 6.7% to 6.0% for non-dual-eligible beneficiaries. In adjusted analysis, CJR participation was associated with a reduced difference in complications between dual-eligible and non-dual-eligible beneficiaries (−0.9 percentage points, 95% CI −1.6 to −0.1). The reduction in disparities was observed among hospitals without prior experience in a voluntary LEJR bundled payment model. There were no differential changes in 90-day readmissions or mortality.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Mandatory participation in a bundled payment program was associated with reduced disparities in joint replacement complications for Medicare beneficiaries with low income. To our knowledge, this is the first evidence of reduced socioeconomic disparities in outcomes under value-based payments.</p>\n </section>\n </div>","PeriodicalId":55065,"journal":{"name":"Health Services Research","volume":"59 5","pages":""},"PeriodicalIF":3.2000,"publicationDate":"2024-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1475-6773.14369","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1475-6773.14369","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
To determine whether mandatory participation by hospitals in bundled payments for lower extremity joint replacement (LEJR) was associated with changes in outcome disparities for patients dually eligible for Medicare and Medicaid.
Data Sources and Study Setting
We used Medicare claims data for beneficiaries undergoing LEJR in the United States between 2011 and 2017.
Study Design
We conducted a retrospective observational study using a differences-in-differences method to compare changes in outcome disparities between dual-eligible and non-dual eligible beneficiaries after hospital participation in the Comprehensive Care for Joint Replacement (CJR) program. The primary outcome was LEJR complications. Secondary outcomes included 90-day readmissions and mortality.
Data Extraction Methods
We identified hospitals in the US market areas eligible for CJR. We included beneficiaries in the intervention group who received joint replacement at hospitals in markets randomized to participate in CJR. The comparison group included patients who received joint replacement at hospitals in markets who were eligible for CJR but randomized to control.
Principal Findings
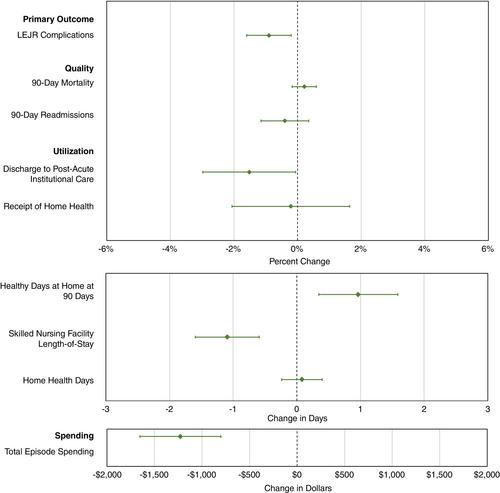
The study included 1,603,555 Medicare beneficiaries (mean age, 74.6 years, 64.3% women, 11.0% dual-eligible). Among participant hospitals, complications decreased between baseline and intervention periods from 11.0% to 10.1% for dual-eligible and 7.0% to 6.4% for non-dual-eligible beneficiaries. Among nonparticipant hospitals, complications decreased from 10.3% to 9.8% for dual-eligible and 6.7% to 6.0% for non-dual-eligible beneficiaries. In adjusted analysis, CJR participation was associated with a reduced difference in complications between dual-eligible and non-dual-eligible beneficiaries (−0.9 percentage points, 95% CI −1.6 to −0.1). The reduction in disparities was observed among hospitals without prior experience in a voluntary LEJR bundled payment model. There were no differential changes in 90-day readmissions or mortality.
Conclusions
Mandatory participation in a bundled payment program was associated with reduced disparities in joint replacement complications for Medicare beneficiaries with low income. To our knowledge, this is the first evidence of reduced socioeconomic disparities in outcomes under value-based payments.
期刊介绍:
Health Services Research (HSR) is a peer-reviewed scholarly journal that provides researchers and public and private policymakers with the latest research findings, methods, and concepts related to the financing, organization, delivery, evaluation, and outcomes of health services. Rated as one of the top journals in the fields of health policy and services and health care administration, HSR publishes outstanding articles reporting the findings of original investigations that expand knowledge and understanding of the wide-ranging field of health care and that will help to improve the health of individuals and communities.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
