Alice Thompson, Bev James, Rotimi David, Mohamed Youseff, Nicholas Gill, Matthew Jefferies, Pradeep Bose, Gokul Kanda Swamy
{"title":"Urothelial Malignancy After Normal Hematuria Clinic Investigations: Does Non-visible Hematuria Need Reinvestigation?","authors":"Alice Thompson, Bev James, Rotimi David, Mohamed Youseff, Nicholas Gill, Matthew Jefferies, Pradeep Bose, Gokul Kanda Swamy","doi":"10.5152/tud.2024.23025","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong> Hematuria is the most common referral to Urology. Most initial evaluations are normal; however there are few medium- to long-term studies about these patients after they are discharged.</p><p><strong>Methods: </strong> This study was a retrospective observational case-control study. Patients with normal initial investigations in our hematuria clinic (HC) over a 2-year period in 2012-2013 were included. We reviewed the electronic records of patients choosing January 1, 2021, as our reference date providing a median follow-up of 99 months. The primary aim of this study was to assess the missed urothelial malignancy (UM) rate in this cohort and also the UM rate in those re-referred to the HC.</p><p><strong>Results: </strong> The study included 573 patients of whom 24.6% (141/573) were re-referred to urology during the study period. The overall missed UM cancer rate was 0.5% and 0.2% died as a result in this follow-up period. The UM cancer rate in those re-referred was 4.3% and of those re-referred with visible hematuria (VH) the UM cancer rate was 5.7%. No patients re-referred with non-visible VH (NVH) were diagnosed with UM. The only urological death during this time was due to UM.</p><p><strong>Conclusion: </strong> All urological malignancy and mortality remain very low even at mediumto long-term follow-up after an initial normal HC investigation. In this study, no patients with recurrent NVH developed UM; therefore, recurrent NVH is unlikely to need reinvestigation. The risk of UM in those re-referred with VH is low but more substantial and warrants reinvestigation, which should include computed tomography urogram imaging.</p>","PeriodicalId":101337,"journal":{"name":"Urology research & practice","volume":"50 2","pages":"102-106"},"PeriodicalIF":1.1000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11232076/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology research & practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/tud.2024.23025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Hematuria is the most common referral to Urology. Most initial evaluations are normal; however there are few medium- to long-term studies about these patients after they are discharged.
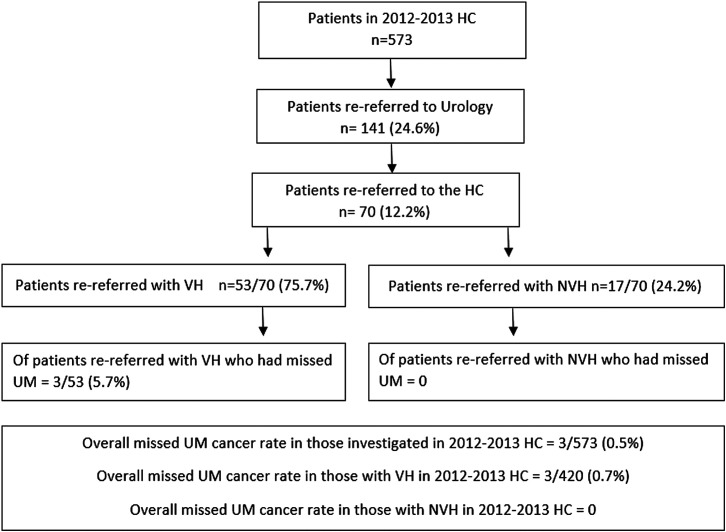
Methods: This study was a retrospective observational case-control study. Patients with normal initial investigations in our hematuria clinic (HC) over a 2-year period in 2012-2013 were included. We reviewed the electronic records of patients choosing January 1, 2021, as our reference date providing a median follow-up of 99 months. The primary aim of this study was to assess the missed urothelial malignancy (UM) rate in this cohort and also the UM rate in those re-referred to the HC.
Results: The study included 573 patients of whom 24.6% (141/573) were re-referred to urology during the study period. The overall missed UM cancer rate was 0.5% and 0.2% died as a result in this follow-up period. The UM cancer rate in those re-referred was 4.3% and of those re-referred with visible hematuria (VH) the UM cancer rate was 5.7%. No patients re-referred with non-visible VH (NVH) were diagnosed with UM. The only urological death during this time was due to UM.
Conclusion: All urological malignancy and mortality remain very low even at mediumto long-term follow-up after an initial normal HC investigation. In this study, no patients with recurrent NVH developed UM; therefore, recurrent NVH is unlikely to need reinvestigation. The risk of UM in those re-referred with VH is low but more substantial and warrants reinvestigation, which should include computed tomography urogram imaging.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
