{"title":"Preoperative biomarkers associated with delayed neurocognitive recovery","authors":"Mariana Thedim, Duygu Aydin, Gerhard Schneider, Rajesh Kumar, Matthias Kreuzer, Susana Vacas","doi":"10.1007/s10877-024-01218-2","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Abstract</h3><p>To identify baseline biomarkers of delayed neurocognitive recovery (dNCR) using monitors commonly used in anesthesia. In this sub-study of observational prospective cohorts, we evaluated adult patients submitted to general anesthesia in a tertiary academic center in the United States. Electroencephalographic (EEG) features and cerebral oximetry were assessed in the perioperative period. The primary outcome was dNCR, defined as a decrease of 2 scores in the global Montreal Cognitive Assessment (MoCA) between the baseline and postoperative period. Forty-six adults (median [IQR] age, 65 [15]; 57% females; 65% American Society of Anesthesiologists (ASA) 3 were analyzed. Thirty-one patients developed dNCR (67%). Baseline higher EEG power in the lower alpha band (AUC = 0.73 (95% CI 0.48–0.93)) and lower alpha peak frequency (AUC = 0.83 (95% CI 0.48–1)), as well as lower cerebral oximetry (68 [5] vs 72 [3], <i>p</i> = 0.011) were associated with dNCR. Higher EEG power in the lower alpha band, lower alpha peak frequency, and lower cerebral oximetry values can be surrogates of baseline brain vulnerability.</p><h3 data-test=\"abstract-sub-heading\">Graphical abstract</h3>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":"10 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01218-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
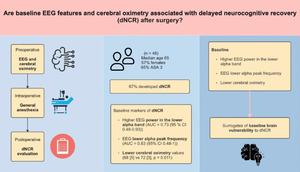
To identify baseline biomarkers of delayed neurocognitive recovery (dNCR) using monitors commonly used in anesthesia. In this sub-study of observational prospective cohorts, we evaluated adult patients submitted to general anesthesia in a tertiary academic center in the United States. Electroencephalographic (EEG) features and cerebral oximetry were assessed in the perioperative period. The primary outcome was dNCR, defined as a decrease of 2 scores in the global Montreal Cognitive Assessment (MoCA) between the baseline and postoperative period. Forty-six adults (median [IQR] age, 65 [15]; 57% females; 65% American Society of Anesthesiologists (ASA) 3 were analyzed. Thirty-one patients developed dNCR (67%). Baseline higher EEG power in the lower alpha band (AUC = 0.73 (95% CI 0.48–0.93)) and lower alpha peak frequency (AUC = 0.83 (95% CI 0.48–1)), as well as lower cerebral oximetry (68 [5] vs 72 [3], p = 0.011) were associated with dNCR. Higher EEG power in the lower alpha band, lower alpha peak frequency, and lower cerebral oximetry values can be surrogates of baseline brain vulnerability.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
