Hana M Broulikova, Jacqueline Wallage, Luca Roggeveen, Lucas Fleuren, Tingjie Guo, Paul W G Elbers, Judith E Bosmans
{"title":"Cost-effectiveness of data driven personalised antibiotic dosing in critically ill patients with sepsis or septic shock.","authors":"Hana M Broulikova, Jacqueline Wallage, Luca Roggeveen, Lucas Fleuren, Tingjie Guo, Paul W G Elbers, Judith E Bosmans","doi":"10.1007/s10877-024-01257-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study provides an economic evaluation of bedside, data-driven, and model-informed precision dosing of antibiotics in comparison with usual care among critically ill patients with sepsis or septic shock.</p><p><strong>Methods: </strong>This economic evaluation was conducted alongside an AutoKinetics randomized controlled trial. Effect measures included quality-adjusted life years (QALYs), mortality and pharmacokinetic target attainment. Costs were measured from a societal perspective. Missing data was multiply imputed, and bootstrapping was used to estimate statistical uncertainty. Differences in effects and costs were estimated using bivariate regression and used to calculate incremental cost-effectiveness ratios.</p><p><strong>Results: </strong>Patients in the intervention group had higher costs (€42,684 vs. 39,475), lower mortality (42% vs. 49%), more QALYs (0.184 vs. 0.153), and higher pharmacokinetic target attainment (69% vs. 48%). Only the difference for target attainment was found statistically significant. An additional €18,129, €55,576, and €123,493 needs to be invested to attain the targeted plasma levels for one more patient, to save one life and gain one QALY, respectively. The probability of cost-effectiveness for all effect outcomes is below 60% for most acceptable willingness-to-pay thresholds.</p><p><strong>Conclusions: </strong>Data-driven personalised antibiotic dosing in critically ill patients as implemented in the AutoKinetics trial cannot be recommended for implementation as a cost-effective intervention.</p><p><strong>Trial registration: </strong>The trial was prospectively registered at Netherlands Trial Register (NTR), NL6501/NTR6689 on 25 August 2017 and at the European Clinical Trials Database (EudraCT), 2017-002478-37 on 6 November 2017.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"937-946"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474602/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01257-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study provides an economic evaluation of bedside, data-driven, and model-informed precision dosing of antibiotics in comparison with usual care among critically ill patients with sepsis or septic shock.
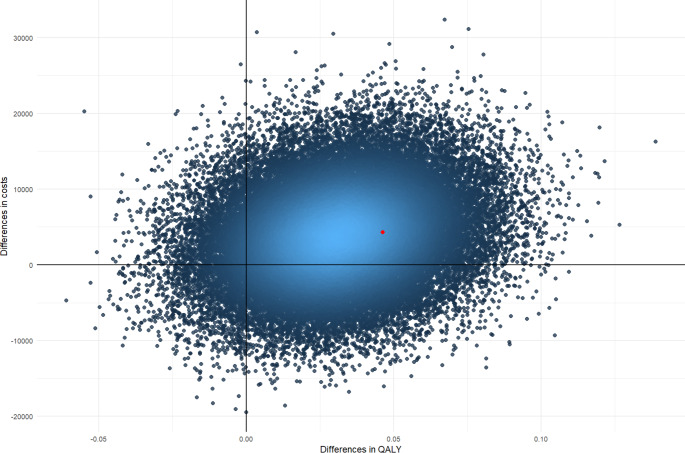
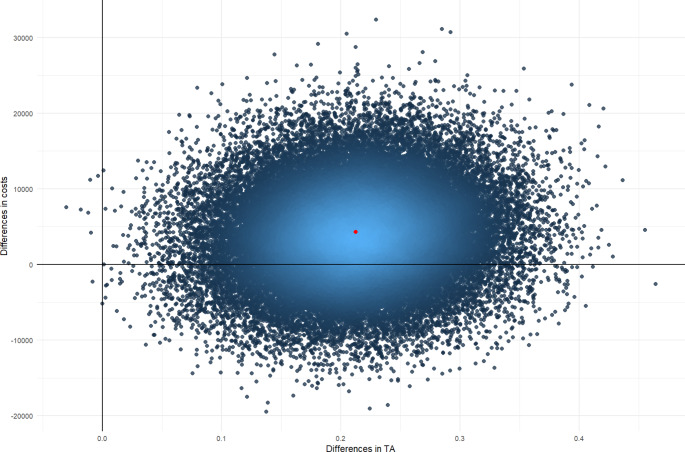
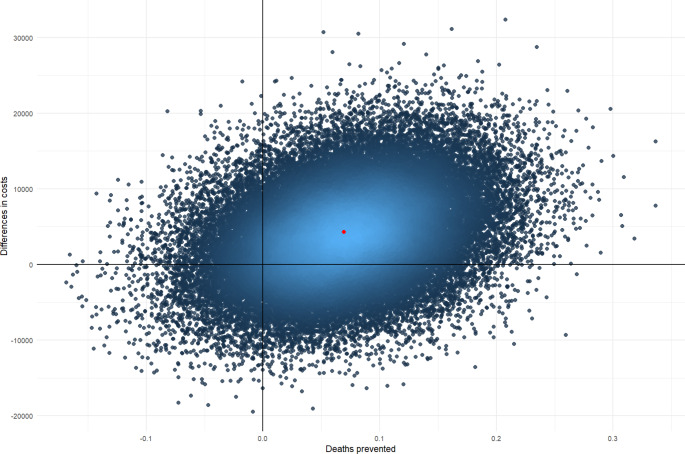
Methods: This economic evaluation was conducted alongside an AutoKinetics randomized controlled trial. Effect measures included quality-adjusted life years (QALYs), mortality and pharmacokinetic target attainment. Costs were measured from a societal perspective. Missing data was multiply imputed, and bootstrapping was used to estimate statistical uncertainty. Differences in effects and costs were estimated using bivariate regression and used to calculate incremental cost-effectiveness ratios.
Results: Patients in the intervention group had higher costs (€42,684 vs. 39,475), lower mortality (42% vs. 49%), more QALYs (0.184 vs. 0.153), and higher pharmacokinetic target attainment (69% vs. 48%). Only the difference for target attainment was found statistically significant. An additional €18,129, €55,576, and €123,493 needs to be invested to attain the targeted plasma levels for one more patient, to save one life and gain one QALY, respectively. The probability of cost-effectiveness for all effect outcomes is below 60% for most acceptable willingness-to-pay thresholds.
Conclusions: Data-driven personalised antibiotic dosing in critically ill patients as implemented in the AutoKinetics trial cannot be recommended for implementation as a cost-effective intervention.
Trial registration: The trial was prospectively registered at Netherlands Trial Register (NTR), NL6501/NTR6689 on 25 August 2017 and at the European Clinical Trials Database (EudraCT), 2017-002478-37 on 6 November 2017.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
