Helen Jarvis, Charlotte Berry, Jonathan Worsfold, Vanessa Hebditch, Stephen Ryder
{"title":"Increasing engagement with liver disease management across the UK: a follow-up cross-sectional survey.","authors":"Helen Jarvis, Charlotte Berry, Jonathan Worsfold, Vanessa Hebditch, Stephen Ryder","doi":"10.3399/BJGPO.2024.0142","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liver disease is an increasing cause of premature mortality. Early detection of liver disease in primary care gives opportunity to intervene and change outcomes. Engagement in liver disease care by NHS bodies responsible for primary care pathway development could drive improvements. The formation of integrated care systems (ICS) in England provides an opportunity to reassess engagement with liver disease nationally.</p><p><strong>Aim: </strong>To update the level of engagement with community chronic liver disease management among ICSs and health authorities across the UK.</p><p><strong>Design & setting: </strong>A cross-sectional follow-up survey to ICS and UK health boards.</p><p><strong>Method: </strong>Questions used for a previous survey in 2020 were adapted and sent electronically to NHS bodies responsible for health care across the UK, using a freedom of information request. Quantitative analysis was undertaken using Microsoft Excel.</p><p><strong>Results: </strong>There were 67 responses from 68 possible ICS and health board areas, representing 99% UK coverage. Twenty-seven per cent had a named individual responsible for liver disease. Monitoring of local liver disease health statistics happened in 34% of all UK areas. Comprehensive care pathways were available in <i>n</i> = 24/67 (36%) of areas, an increase from 26% in the 2020 survey. Areas with no liver pathways in place fell from 58% to 36% between the two surveys. Regional variations persist, with Wales and Scotland moving towards comprehensive coverage. Almost double the number of areas were making use of transient elastography within community pathways of care, up from 25% to 46%.</p><p><strong>Conclusion: </strong>The results of this re-survey highlight improvements, but emphasise the need to build on regional success to further reduce inequality in care commissioning.</p>","PeriodicalId":36541,"journal":{"name":"BJGP Open","volume":" ","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138023/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJGP Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3399/BJGPO.2024.0142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Liver disease is an increasing cause of premature mortality. Early detection of liver disease in primary care gives opportunity to intervene and change outcomes. Engagement in liver disease care by NHS bodies responsible for primary care pathway development could drive improvements. The formation of integrated care systems (ICS) in England provides an opportunity to reassess engagement with liver disease nationally.
Aim: To update the level of engagement with community chronic liver disease management among ICSs and health authorities across the UK.
Design & setting: A cross-sectional follow-up survey to ICS and UK health boards.
Method: Questions used for a previous survey in 2020 were adapted and sent electronically to NHS bodies responsible for health care across the UK, using a freedom of information request. Quantitative analysis was undertaken using Microsoft Excel.
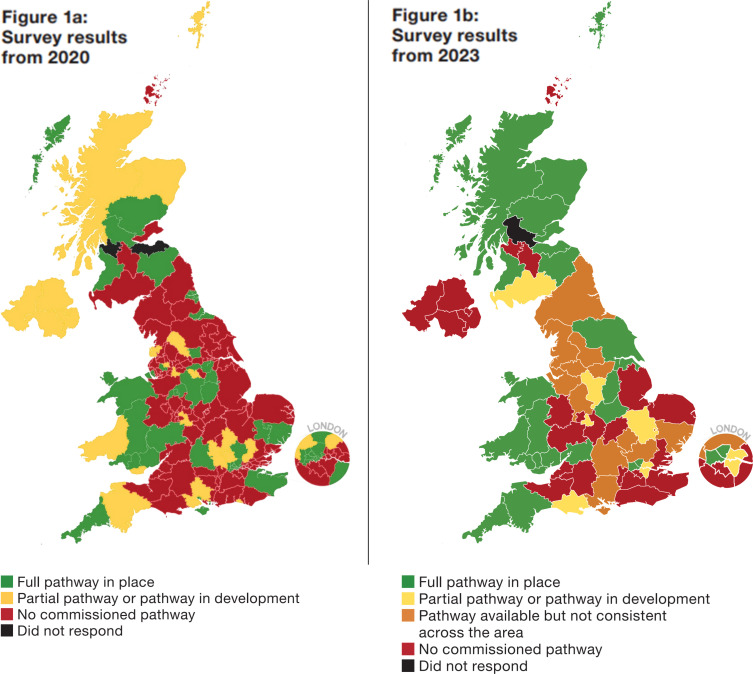
Results: There were 67 responses from 68 possible ICS and health board areas, representing 99% UK coverage. Twenty-seven per cent had a named individual responsible for liver disease. Monitoring of local liver disease health statistics happened in 34% of all UK areas. Comprehensive care pathways were available in n = 24/67 (36%) of areas, an increase from 26% in the 2020 survey. Areas with no liver pathways in place fell from 58% to 36% between the two surveys. Regional variations persist, with Wales and Scotland moving towards comprehensive coverage. Almost double the number of areas were making use of transient elastography within community pathways of care, up from 25% to 46%.
Conclusion: The results of this re-survey highlight improvements, but emphasise the need to build on regional success to further reduce inequality in care commissioning.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
