{"title":"MHC class II genotypes are independent predictors of anti-PD1 immunotherapy response in melanoma","authors":"Arne Claeys, Jimmy Van den Eynden","doi":"10.1038/s43856-024-00612-w","DOIUrl":null,"url":null,"abstract":"Immune checkpoint blockade is a highly successful anti-cancer immunotherapy. Both CTLA4 and PD1 checkpoint blockers are clinically available for melanoma treatment, with anti-PD1 therapy reaching response rates of 35-40%. These responses, which are mediated via neoantigen presentation by the polymorphic MHC complex, are hard to predict and the tumor mutation burden is currently one of the few available biomarkers. While MHC genotypes are expected to determine therapy responses, association studies have remained largely elusive. We developed an overall MHC genotype binding score (MGBS), indicative of a patient’s MHC class I (MHC-I) and class II (MHC-II) neoantigen binding capacity and solely based on the germline MHC-I (MGBS-I) and MHC-II (MGBS-II) genotypes. These scores were then correlated to survival and clinical responses following anti-PD1 immunotherapy in a previously published dataset of 144 melanoma patients. We demonstrate that MGBS scores are TMB-independent predictors of anti-PD1 immunotherapy responses in melanoma. Opposite outcomes were found for both MHC classes, with high MGBS-I and MGBS-II predicting good and bad outcomes, respectively. Interestingly, high MGBS-II is mainly associated with treatment response failure in a subgroup of anti-CTLA4 pretreated patients. Our results suggest that MGBS, calculated solely from the MHC genotype, has clinical potential as a non-invasive and tumor-independent biomarker to guide anti-cancer immunotherapy in melanoma. Many cancer patients are successfully treated with immunotherapy, which boosts the immune system to eliminate cancer cells. While this therapy is successful in around half of skin cancer melanoma patients, it is currently hard to determine in advance which patients respond well. Immune cells react to tumor proteins that are presented at the cancer cell surface by molecules called MHC. These are unique for every patient. We aimed to determine whether the ability of MHC to bind to tumor proteins determines how well therapy works and developed a new way to quantify this interaction. Surprisingly, less ability for tumor proteins to bind to the unconventional class II MHC resulted in better clinical outcome in patients with melanoma. Our results provide new understanding of tumor-immune interaction and the new method may help determine which patients with melanoma will respond to therapy. Claeys and Van den Eynden demonstrate that the genotype-specific binding properties of the Major Histocompatibility Complex (MHC) can predict outcome in melanoma patients treated with immunotherapy. Their results suggest an immunomodulatory role of non-canonical MHC-II presentable neoantigens.","PeriodicalId":72646,"journal":{"name":"Communications medicine","volume":" ","pages":"1-8"},"PeriodicalIF":5.4000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11443121/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Communications medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.nature.com/articles/s43856-024-00612-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
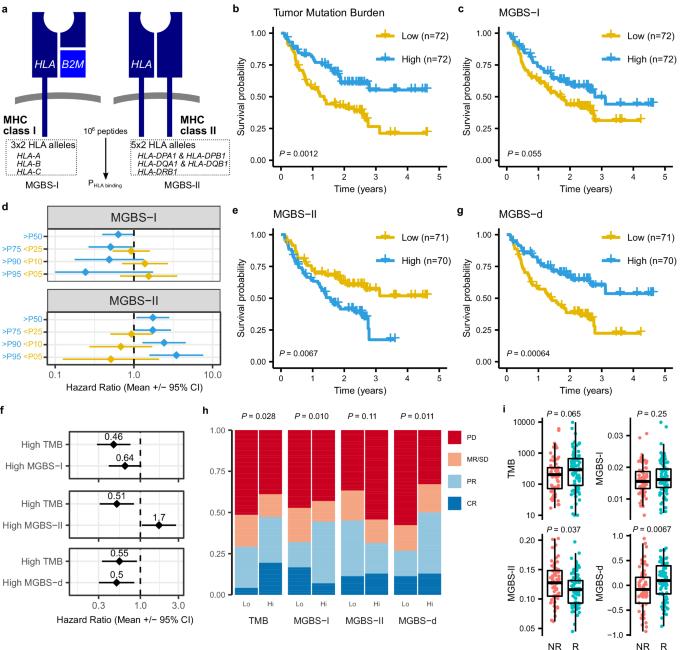
Immune checkpoint blockade is a highly successful anti-cancer immunotherapy. Both CTLA4 and PD1 checkpoint blockers are clinically available for melanoma treatment, with anti-PD1 therapy reaching response rates of 35-40%. These responses, which are mediated via neoantigen presentation by the polymorphic MHC complex, are hard to predict and the tumor mutation burden is currently one of the few available biomarkers. While MHC genotypes are expected to determine therapy responses, association studies have remained largely elusive. We developed an overall MHC genotype binding score (MGBS), indicative of a patient’s MHC class I (MHC-I) and class II (MHC-II) neoantigen binding capacity and solely based on the germline MHC-I (MGBS-I) and MHC-II (MGBS-II) genotypes. These scores were then correlated to survival and clinical responses following anti-PD1 immunotherapy in a previously published dataset of 144 melanoma patients. We demonstrate that MGBS scores are TMB-independent predictors of anti-PD1 immunotherapy responses in melanoma. Opposite outcomes were found for both MHC classes, with high MGBS-I and MGBS-II predicting good and bad outcomes, respectively. Interestingly, high MGBS-II is mainly associated with treatment response failure in a subgroup of anti-CTLA4 pretreated patients. Our results suggest that MGBS, calculated solely from the MHC genotype, has clinical potential as a non-invasive and tumor-independent biomarker to guide anti-cancer immunotherapy in melanoma. Many cancer patients are successfully treated with immunotherapy, which boosts the immune system to eliminate cancer cells. While this therapy is successful in around half of skin cancer melanoma patients, it is currently hard to determine in advance which patients respond well. Immune cells react to tumor proteins that are presented at the cancer cell surface by molecules called MHC. These are unique for every patient. We aimed to determine whether the ability of MHC to bind to tumor proteins determines how well therapy works and developed a new way to quantify this interaction. Surprisingly, less ability for tumor proteins to bind to the unconventional class II MHC resulted in better clinical outcome in patients with melanoma. Our results provide new understanding of tumor-immune interaction and the new method may help determine which patients with melanoma will respond to therapy. Claeys and Van den Eynden demonstrate that the genotype-specific binding properties of the Major Histocompatibility Complex (MHC) can predict outcome in melanoma patients treated with immunotherapy. Their results suggest an immunomodulatory role of non-canonical MHC-II presentable neoantigens.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
