{"title":"Computed tomography patterns and clinical outcomes of radiation pneumonitis in non-small-cell lung cancer patients.","authors":"Ji Hoon Choi, Hee Kang, Ji Su Lim, Ki-Nam Lee","doi":"10.1177/20584601241288502","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Radiation pneumonitis (RP) is not an uncommon complication in lung cancer patients undergoing radiation therapy (RT) and symptomatic RP can affect their quality of life.</p><p><strong>Purpose: </strong>To investigate the CT findings of RP in non-small cell lung cancer (NSCLC) patients and their relationship with clinical outcomes.</p><p><strong>Materials and methods: </strong>We reviewed data from 240 NSCLC patients who underwent RT between 2014 and 2022. CT findings of RP were evaluated for parenchymal abnormalities and distribution, which were then classified into three patterns: localized pneumonia (LP), cryptogenic organizing pneumonia (COP), and acute interstitial pneumonia (AIP). Clinical outcomes of RP were evaluated based on Common Terminology Criteria for Adverse Events (CTCAE) grade.</p><p><strong>Results: </strong>Of the 153 patients, 135 developed RP. The most common pattern was LP (<i>n</i> = 78), followed by COP (<i>n</i> = 30) and AIP (<i>n</i> = 25). Among the three CT patterns, CTCAE grade and days between the start of RT and the onset of RP (RT-RP days) were statistically significantly different (<i>p</i> < 0.05). The patients with AIP patterns exhibited higher CTCAE grade, and fewer RT-RP days compared to those with non-AIP patterns (<i>p</i> < 0.05). In these patients, lung-to-lung metastasis and underlying interstitial lung abnormality were observed more frequently (<i>p</i> < 0.05). Underlying pulmonary fibrosis, the AIP pattern, and higher CT extent scores were more frequently observed in higher CTCAE grade group (<i>p</i> < 0.001). In multiple regression analysis, age, bilateral distribution, RT-RP days, and CT extent score ≥3 were independent predicting factors for higher CTCAE grade.</p><p><strong>Conclusions: </strong>RP in NSCLC patients can be classified into LP, COP, and AIP patterns and they exhibit different severities in clinical outcomes.</p>","PeriodicalId":72063,"journal":{"name":"Acta radiologica open","volume":"13 10","pages":"20584601241288502"},"PeriodicalIF":1.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459547/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta radiologica open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20584601241288502","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Radiation pneumonitis (RP) is not an uncommon complication in lung cancer patients undergoing radiation therapy (RT) and symptomatic RP can affect their quality of life.
Purpose: To investigate the CT findings of RP in non-small cell lung cancer (NSCLC) patients and their relationship with clinical outcomes.
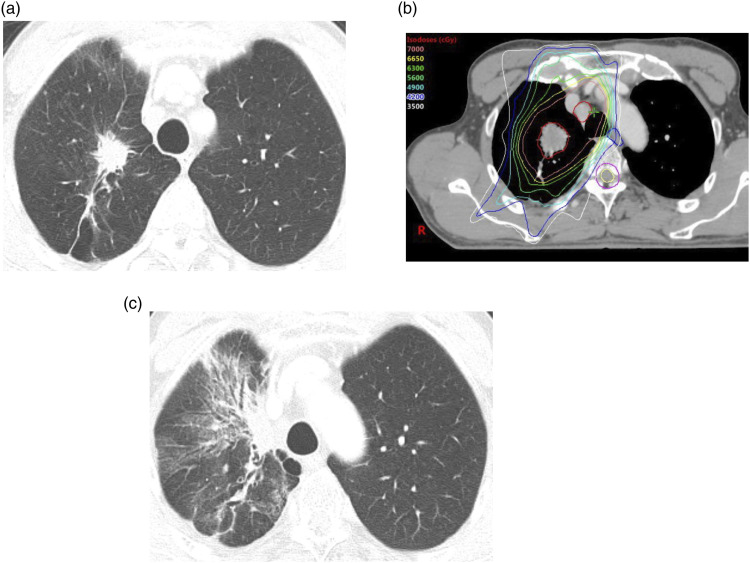
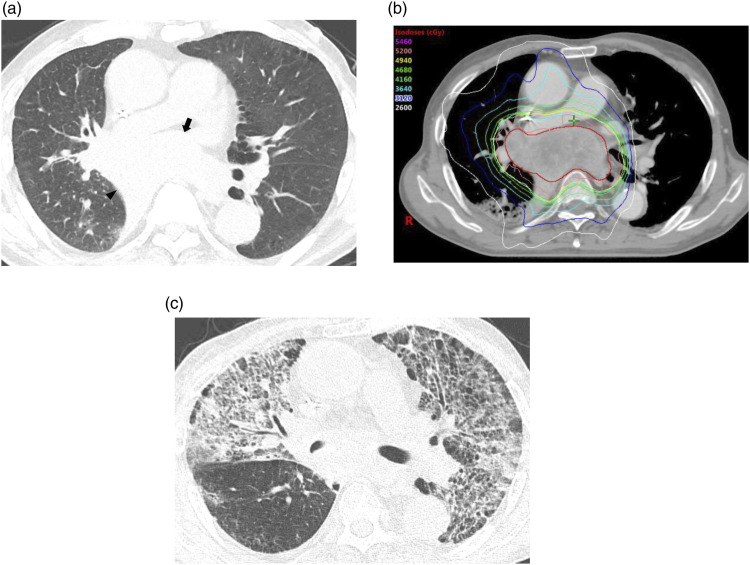
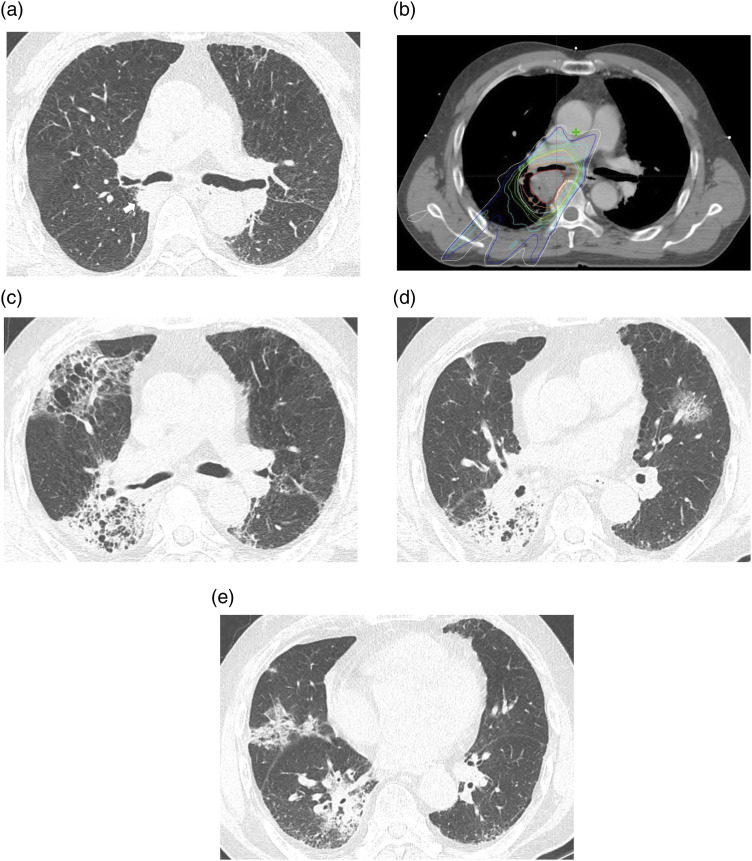
Materials and methods: We reviewed data from 240 NSCLC patients who underwent RT between 2014 and 2022. CT findings of RP were evaluated for parenchymal abnormalities and distribution, which were then classified into three patterns: localized pneumonia (LP), cryptogenic organizing pneumonia (COP), and acute interstitial pneumonia (AIP). Clinical outcomes of RP were evaluated based on Common Terminology Criteria for Adverse Events (CTCAE) grade.
Results: Of the 153 patients, 135 developed RP. The most common pattern was LP (n = 78), followed by COP (n = 30) and AIP (n = 25). Among the three CT patterns, CTCAE grade and days between the start of RT and the onset of RP (RT-RP days) were statistically significantly different (p < 0.05). The patients with AIP patterns exhibited higher CTCAE grade, and fewer RT-RP days compared to those with non-AIP patterns (p < 0.05). In these patients, lung-to-lung metastasis and underlying interstitial lung abnormality were observed more frequently (p < 0.05). Underlying pulmonary fibrosis, the AIP pattern, and higher CT extent scores were more frequently observed in higher CTCAE grade group (p < 0.001). In multiple regression analysis, age, bilateral distribution, RT-RP days, and CT extent score ≥3 were independent predicting factors for higher CTCAE grade.
Conclusions: RP in NSCLC patients can be classified into LP, COP, and AIP patterns and they exhibit different severities in clinical outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
