Three cases of autoinflammatory disease with novel NLRC4 mutations, and the first mutation reported in the CARD domain of NLRC4 associated with autoinflammatory infantile enterocolitis (AIFEC).
Kosar Asna Ashari, Nima Parvaneh, Kayvan Mirnia, Mehri Ayati, Maryam Saeedi, Farhad Salehzadeh, Mohammad Shahrooei, Razieh Sangsari, Pejman Rohani, Vahid Ziaee
{"title":"Three cases of autoinflammatory disease with novel NLRC4 mutations, and the first mutation reported in the CARD domain of NLRC4 associated with autoinflammatory infantile enterocolitis (AIFEC).","authors":"Kosar Asna Ashari, Nima Parvaneh, Kayvan Mirnia, Mehri Ayati, Maryam Saeedi, Farhad Salehzadeh, Mohammad Shahrooei, Razieh Sangsari, Pejman Rohani, Vahid Ziaee","doi":"10.1186/s12969-024-01020-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gain of function (GOF) mutations in NOD-like receptor family CARD-containing 4 protein (NLRC4) gene induce a wide spectrum of autoinflammatory phenotypes. Currently, we categorize them into four groups: familial cold autoinflammatory syndrome (FCAS)4, autoinflammatory infantile enterocolitis (AIFEC), NLRC4-macrophage associated syndrome (MAS), and neonatal-onset multisystem inflammatory disease (NOMID). The rarity and complexity of the disease necessitate the description of new cases and a reexamination of our understanding of the condition.</p><p><strong>Case presentations: </strong>We present three patients with NLRC4-GOF mutations and AIFEC phenotypes. The first patient is an infant girl with periodic fever, seizure, high inflammatory markers, and an episode of macrophage associated syndrome (MAS). History of recurrent fever episodes since childhood was reported in mother and maternal grandmother. A heterozygous mutation was found in CARD domain of NLRC4: c.A91C: p.Asn31His. The second patient is an adolescent boy with periodic fever, diarrhea, aphthous stomatitis, seizure, and central nervous system (CNS) vasculitis. A heterozygous mutation was found in NLRC4 gene: c.1202T > C. p. Val401Ala. The third patient is a child with chronic diarrhea and elevated inflammatory markers. We found a heterozygous mutation in NLRC4 gene: c.390delG: p.S132Afs*21. All mutations have been reported for the first time as NLRC4 mutations associated with autoinflammation. We introduced novel mutations in the CARD domain and between CARD and NBD domain in the first and third cases, respectively. All three children are under remission following treatment.</p><p><strong>Conclusions: </strong>NLRC4-GOF mutations can be associated with autoinflammation with diverse symptoms. Given the rarity of the disease and the possibility of new mutations being identified, the existence of a phenotype/genotype correlation has yet to be thoroughly investigated. The variety in manifestations and severity spectrum mandates a variety of treatments. Adalimumab has shown favorable outcomes in our AIFEC cases.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"22 1","pages":"90"},"PeriodicalIF":2.3000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487858/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-024-01020-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Gain of function (GOF) mutations in NOD-like receptor family CARD-containing 4 protein (NLRC4) gene induce a wide spectrum of autoinflammatory phenotypes. Currently, we categorize them into four groups: familial cold autoinflammatory syndrome (FCAS)4, autoinflammatory infantile enterocolitis (AIFEC), NLRC4-macrophage associated syndrome (MAS), and neonatal-onset multisystem inflammatory disease (NOMID). The rarity and complexity of the disease necessitate the description of new cases and a reexamination of our understanding of the condition.
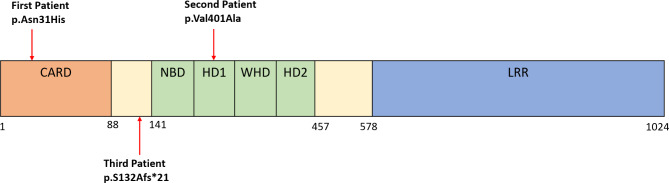
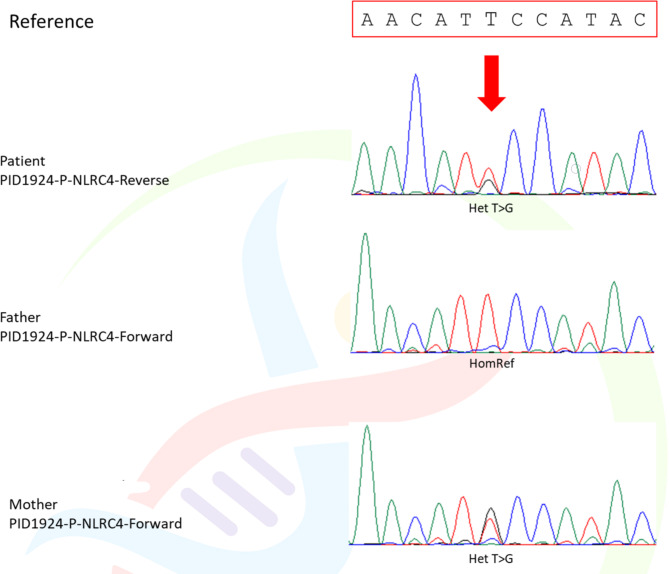
Case presentations: We present three patients with NLRC4-GOF mutations and AIFEC phenotypes. The first patient is an infant girl with periodic fever, seizure, high inflammatory markers, and an episode of macrophage associated syndrome (MAS). History of recurrent fever episodes since childhood was reported in mother and maternal grandmother. A heterozygous mutation was found in CARD domain of NLRC4: c.A91C: p.Asn31His. The second patient is an adolescent boy with periodic fever, diarrhea, aphthous stomatitis, seizure, and central nervous system (CNS) vasculitis. A heterozygous mutation was found in NLRC4 gene: c.1202T > C. p. Val401Ala. The third patient is a child with chronic diarrhea and elevated inflammatory markers. We found a heterozygous mutation in NLRC4 gene: c.390delG: p.S132Afs*21. All mutations have been reported for the first time as NLRC4 mutations associated with autoinflammation. We introduced novel mutations in the CARD domain and between CARD and NBD domain in the first and third cases, respectively. All three children are under remission following treatment.
Conclusions: NLRC4-GOF mutations can be associated with autoinflammation with diverse symptoms. Given the rarity of the disease and the possibility of new mutations being identified, the existence of a phenotype/genotype correlation has yet to be thoroughly investigated. The variety in manifestations and severity spectrum mandates a variety of treatments. Adalimumab has shown favorable outcomes in our AIFEC cases.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
