Xianying Liu, Daniel McGrath, Kelly Ohlrich, Frederick Y. Chen, Lawrence S. Lee, Michael Robich
{"title":"Hypertrophic Cardiomyopathy With Elongated Mitral Valve Leaflets: Clinical Characteristics and Surgical Results","authors":"Xianying Liu, Daniel McGrath, Kelly Ohlrich, Frederick Y. Chen, Lawrence S. Lee, Michael Robich","doi":"10.1155/2024/7078246","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Background:</b> Hypertrophic cardiomyopathy (HCM) is commonly associated with mitral valve pathology. A large majority of patients with HCM have elongated anterior and posterior mitral leaflets. There remains debate regarding the necessity and role of concomitant mitral valve surgery at the time of septal myectomy. We aimed to describe the characteristics and share our surgical experiences with this specific group of patients.</p>\n <p><b>Methods:</b> This retrospective single-center study investigates adult patients with HCM, with or without elongated mitral valve leaflets (MVLs), who underwent elective septal myectomy with or without concomitant mitral valve intervention, between January 1, 2016, and June 30, 2020. Clinical data were obtained from institutional medical records as well as the Society of Thoracic Surgeons data registry. The clinical characteristics and in-hospital surgical outcomes were compared between patients with an elongated MVL and those without.</p>\n <p><b>Results:</b> In total, 379 patients underwent septal myectomy, and 22 patients with intrinsic mitral valve disease were excluded. In addition, 23 patients were excluded due to missing data. Of the remaining 334 patients, 131 (39.2%) had elongated MVL and concomitant MVL plication. Patients with elongated MVL had higher rates of preoperative mitral valve systolic anterior motion (SAM) (94.7% vs. 86.7%, <i>p</i> = 0.019) and higher preoperative provoked left ventricular outflow tract gradient (LVOTG) (134.5 mmHg versus 125.3 mmHg, <i>p</i> = 0.046). Post septal myectomy and mitral valve plication, they had lower rates of postoperative residual mitral regurgitation (3.8% vs. 12.8%, <i>p</i> = 0.006), comparable rates of residual SAM (28.2% vs. 31.5%, <i>p</i> = 0.524), postoperative provoked LVOTG (15.4 mmHg vs. 14.0 mmHg, <i>p</i> = 0.317), 30-day major adverse cardiopulmonary events (2.3% vs. 3.9%, <i>p</i> = 0.409), and mortality (0% vs. 1.0%, <i>p</i> = 0.255).</p>\n <p><b>Conclusions:</b> Elongated MVLs contribute more significantly to dynamic LVOT obstruction, as evidenced during provocative testing. Concomitant mitral valve intervention during septal myectomy can be performed safely and may provide an effective strategy to resolve SAM and stress-induced LVOTG.</p>\n </div>","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"2024 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/7078246","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/7078246","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hypertrophic cardiomyopathy (HCM) is commonly associated with mitral valve pathology. A large majority of patients with HCM have elongated anterior and posterior mitral leaflets. There remains debate regarding the necessity and role of concomitant mitral valve surgery at the time of septal myectomy. We aimed to describe the characteristics and share our surgical experiences with this specific group of patients.
Methods: This retrospective single-center study investigates adult patients with HCM, with or without elongated mitral valve leaflets (MVLs), who underwent elective septal myectomy with or without concomitant mitral valve intervention, between January 1, 2016, and June 30, 2020. Clinical data were obtained from institutional medical records as well as the Society of Thoracic Surgeons data registry. The clinical characteristics and in-hospital surgical outcomes were compared between patients with an elongated MVL and those without.
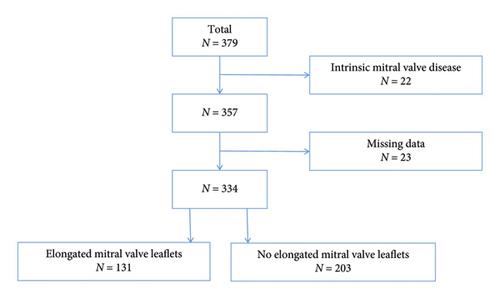
Results: In total, 379 patients underwent septal myectomy, and 22 patients with intrinsic mitral valve disease were excluded. In addition, 23 patients were excluded due to missing data. Of the remaining 334 patients, 131 (39.2%) had elongated MVL and concomitant MVL plication. Patients with elongated MVL had higher rates of preoperative mitral valve systolic anterior motion (SAM) (94.7% vs. 86.7%, p = 0.019) and higher preoperative provoked left ventricular outflow tract gradient (LVOTG) (134.5 mmHg versus 125.3 mmHg, p = 0.046). Post septal myectomy and mitral valve plication, they had lower rates of postoperative residual mitral regurgitation (3.8% vs. 12.8%, p = 0.006), comparable rates of residual SAM (28.2% vs. 31.5%, p = 0.524), postoperative provoked LVOTG (15.4 mmHg vs. 14.0 mmHg, p = 0.317), 30-day major adverse cardiopulmonary events (2.3% vs. 3.9%, p = 0.409), and mortality (0% vs. 1.0%, p = 0.255).
Conclusions: Elongated MVLs contribute more significantly to dynamic LVOT obstruction, as evidenced during provocative testing. Concomitant mitral valve intervention during septal myectomy can be performed safely and may provide an effective strategy to resolve SAM and stress-induced LVOTG.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
