Lytfi Krasniqi, Jordi Sanchez Dahl, Christian Greve Jensen, Poul Erik Mortensen, Axel Brandes, Oke Gerke, Emil Johannes Ravn, Viktor Poulsen, Lars Peter Schødt Riber
{"title":"Long-Term Survival of Mitroflow and Perimount Aortic Valve Replacements","authors":"Lytfi Krasniqi, Jordi Sanchez Dahl, Christian Greve Jensen, Poul Erik Mortensen, Axel Brandes, Oke Gerke, Emil Johannes Ravn, Viktor Poulsen, Lars Peter Schødt Riber","doi":"10.1155/2024/6712990","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Objectives:</b> The American College of Cardiology (ACC) guidelines recommend the same imaging frequency for all bioprosthetic valves, but some have demonstrated poor durability. We aimed to assess mortality differences between small (19–21 mm) and large (23–29 mm) in Mitroflow and Carpentier-Edwards Perimount aortic valves.</p>\n <p><b>Methods</b>: A retrospective observational study was conducted by all patients undergoing isolated surgical aortic valve replacement with Mitroflow or Perimount in Western Denmark between 1999 and 2014 and followed until January 2024. The primary endpoint was all-cause mortality. Secondary endpoints were cardiovascular mortality and sudden cardiac death. A propensity score-matched analysis was performed.</p>\n <p><b>Results:</b> A total of 1150 patients were analyzed, with 496 (43%) receiving Mitroflow valves and 654 (57%) receiving Perimount valves. In the Mitroflow group, 108 (22%) had a valve size of 19–21 mm, and 388 (78%) in the size range of 23–29 mm. In the Perimount group, the distribution was 99 (15%) and 555 (85%), respectively. The compromised survival of Mitroflow valves was attributed to the valve type, regardless of the valve sizes. Larger Mitroflow valves exhibited the same compromised late mortality as smaller valves, 66.7% vs 61.5%, respectively (<i>p</i> = 0.95). The same pattern of mortality was observed in the matched population, with Perimount demonstrating significant lower risk of mortality.</p>\n <p><b>Conclusion:</b> Mitroflow valves were associated with a poorer prognosis compared to Perimount valves. Additionally, larger Mitroflow valves were not associated with an improved prognosis compared to smaller valve sizes. EuroSCORE2 had a significant impact on patient survival.</p>\n </div>","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"2024 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/6712990","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/6712990","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The American College of Cardiology (ACC) guidelines recommend the same imaging frequency for all bioprosthetic valves, but some have demonstrated poor durability. We aimed to assess mortality differences between small (19–21 mm) and large (23–29 mm) in Mitroflow and Carpentier-Edwards Perimount aortic valves.
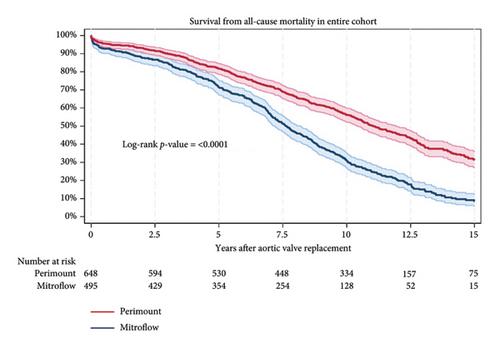
Methods: A retrospective observational study was conducted by all patients undergoing isolated surgical aortic valve replacement with Mitroflow or Perimount in Western Denmark between 1999 and 2014 and followed until January 2024. The primary endpoint was all-cause mortality. Secondary endpoints were cardiovascular mortality and sudden cardiac death. A propensity score-matched analysis was performed.
Results: A total of 1150 patients were analyzed, with 496 (43%) receiving Mitroflow valves and 654 (57%) receiving Perimount valves. In the Mitroflow group, 108 (22%) had a valve size of 19–21 mm, and 388 (78%) in the size range of 23–29 mm. In the Perimount group, the distribution was 99 (15%) and 555 (85%), respectively. The compromised survival of Mitroflow valves was attributed to the valve type, regardless of the valve sizes. Larger Mitroflow valves exhibited the same compromised late mortality as smaller valves, 66.7% vs 61.5%, respectively (p = 0.95). The same pattern of mortality was observed in the matched population, with Perimount demonstrating significant lower risk of mortality.
Conclusion: Mitroflow valves were associated with a poorer prognosis compared to Perimount valves. Additionally, larger Mitroflow valves were not associated with an improved prognosis compared to smaller valve sizes. EuroSCORE2 had a significant impact on patient survival.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
