Heart failure (HF) is a leading cause of hospitalization, and sex differences in care have been described. We assessed sex-specific clinical outcomes and healthcare resource utilization following hospitalization for HF.
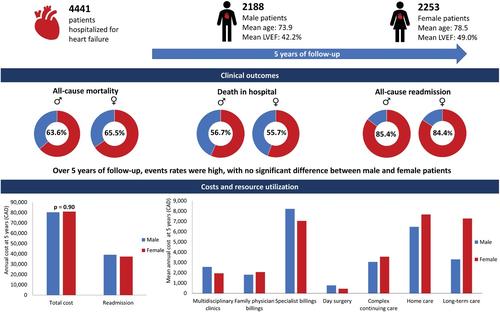
This was an exploratory analysis of patients hospitalized for HF across 10 Canadian hospitals in the Patient-Centered Care Transitions in HF (PACT-HF) cluster-randomized trial. The primary outcome was all-cause mortality. Secondary outcomes included all-cause readmissions, HF readmissions, emergency department (ED) visits, and healthcare resource utilization. Outcomes were obtained via linkages with administrative datasets. Among 4441 patients discharged alive, 50.7% were female. By 5 years, 63.6% and 65.5% of male and female patients, respectively, had died (p = 0.19); 85.4% and 84.4%, respectively, were readmitted (p = 0.35); and 72.2% and 70.9%, respectively, received ED care without hospitalization (p = 0.34). There were no sex differences in mean [SD] number of all-cause readmissions (males, 2.8 [7.8] and females, 3.0 [8.4], p = 0.54), HF readmissions (males, 0.9 [3.6] and females, 0.9 [4.5], p = 0.80), or ED visits (males, 1.8 [11.3] and females, 1.5 [6.0], p = 0.24) per person. There were no sex differences in mean [SD] annual direct healthcare cost per patient (males, $80 334 [116 762] versus females, $81 010 [112 625], p = 0.90), but males received more specialist, multidisciplinary HF clinic, haemodialysis, and day surgical care, and females received more home visits, continuing/convalescent care, and long-term care. Annualized clinical events were highest in first year following index discharge in both males and females.
Among people discharged alive after hospitalization for HF, there were no sex differences in total and annual deaths, readmissions, and ED visits, or in total direct healthcare costs. Despite similar risk profiles, males received relatively more specialist care and day surgical procedures, and females received more supportive care.
Clinical Trial Registration: ClinicalTrials.gov NCT02112227.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
