Cäcilia Jäger, Matthias Niemann, Gideon Hönger, Caroline Wehmeier, Helmut Hopfer, Thomas Menter, Patrizia Amico, Michael Dickenmann, Stefan Schaub
{"title":"Combined Molecular Mismatch Approaches to Predict Immunological Events Within the First Year After Renal Transplantation","authors":"Cäcilia Jäger, Matthias Niemann, Gideon Hönger, Caroline Wehmeier, Helmut Hopfer, Thomas Menter, Patrizia Amico, Michael Dickenmann, Stefan Schaub","doi":"10.1111/tan.15748","DOIUrl":null,"url":null,"abstract":"<p>Several molecular mismatch assessment approaches exist, but data on their combined use are limited. In this study, we aimed to define distinct risk groups for rejection based on the combination of three molecular mismatch assessment approaches (i.e., eplet mismatch count, the number of highly immunogenic eplets and PIRCHE-II score) in 439 consecutive immunological standard risk transplantations. For each molecular mismatch assessment approach, ROC analyses were used to define cut-offs for prediction of (sub) clinical rejection according to Banff 2019 classification within the first year post-transplant as a reference. If all three scores were below the cut-off, the patient was assigned to the low-risk group (19% of patients); if all three scores were above the cut-off, the patient was assigned to the high-risk group (21% of patients). The one-year incidence of (sub) clinical rejection was 12% in the low-risk group and 33% in the high-risk group (<i>p</i> = 0.003). Internal validation of the assigned risk groups for prediction of other outcomes revealed a high consistency: clinical rejection (6% vs. 24%; <i>p</i> = 0.004), ATG-treated rejection (1% vs. 16%; <i>p</i> < 0.001) and development of de novo HLA-DSA at 5 years post-transplant (6% vs. 25%; <i>p</i> = 0.003). The molecular mismatch risk group was an independent predictor for (sub) clinical rejection (high-risk vs. low-risk: hazard ratio 3.11 [95%-CI 1.50–6.45]; <i>p</i> = 0.002). We conclude that combining molecular mismatch approaches allows us to distinguish low- and high-risk groups among standard renal allograft recipients. Independent validation in other patient populations and different ethnicities is required.</p>","PeriodicalId":13172,"journal":{"name":"HLA","volume":"104 5","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2024-11-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/tan.15748","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HLA","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/tan.15748","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
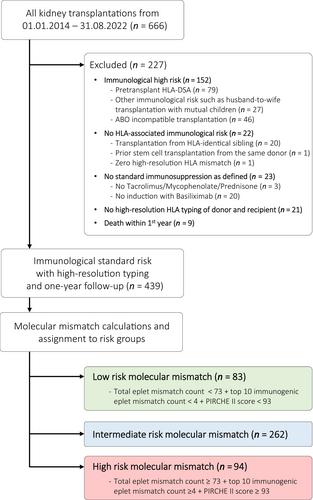
Several molecular mismatch assessment approaches exist, but data on their combined use are limited. In this study, we aimed to define distinct risk groups for rejection based on the combination of three molecular mismatch assessment approaches (i.e., eplet mismatch count, the number of highly immunogenic eplets and PIRCHE-II score) in 439 consecutive immunological standard risk transplantations. For each molecular mismatch assessment approach, ROC analyses were used to define cut-offs for prediction of (sub) clinical rejection according to Banff 2019 classification within the first year post-transplant as a reference. If all three scores were below the cut-off, the patient was assigned to the low-risk group (19% of patients); if all three scores were above the cut-off, the patient was assigned to the high-risk group (21% of patients). The one-year incidence of (sub) clinical rejection was 12% in the low-risk group and 33% in the high-risk group (p = 0.003). Internal validation of the assigned risk groups for prediction of other outcomes revealed a high consistency: clinical rejection (6% vs. 24%; p = 0.004), ATG-treated rejection (1% vs. 16%; p < 0.001) and development of de novo HLA-DSA at 5 years post-transplant (6% vs. 25%; p = 0.003). The molecular mismatch risk group was an independent predictor for (sub) clinical rejection (high-risk vs. low-risk: hazard ratio 3.11 [95%-CI 1.50–6.45]; p = 0.002). We conclude that combining molecular mismatch approaches allows us to distinguish low- and high-risk groups among standard renal allograft recipients. Independent validation in other patient populations and different ethnicities is required.
期刊介绍:
HLA, the journal, publishes articles on various aspects of immunogenetics. These include the immunogenetics of cell surface antigens, the ontogeny and phylogeny of the immune system, the immunogenetics of cell interactions, the functional aspects of cell surface molecules and their natural ligands, and the role of tissue antigens in immune reactions. Additionally, the journal covers experimental and clinical transplantation, the relationships between normal tissue antigens and tumor-associated antigens, the genetic control of immune response and disease susceptibility, and the biochemistry and molecular biology of alloantigens and leukocyte differentiation. Manuscripts on molecules expressed on lymphoid cells, myeloid cells, platelets, and non-lineage-restricted antigens are welcomed. Lastly, the journal focuses on the immunogenetics of histocompatibility antigens in both humans and experimental animals, including their tissue distribution, regulation, and expression in normal and malignant cells, as well as the use of antigens as markers for disease.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
