{"title":"Systematic assessment of early brain injury severity at admission with aneurysmal subarachnoid hemorrhage.","authors":"Sheri Tuzi, Beate Kranawetter, Dorothee Mielke, Veit Rohde, Vesna Malinova","doi":"10.1007/s10143-024-03081-w","DOIUrl":null,"url":null,"abstract":"<p><p>Early brain injury (EBI) after aneurysmal subarachnoid hemorrhage (aSAH) has been increasingly recognized as a risk factor for delayed cerebral ischemia (DCI). While several clinical and radiological EBI biomarkers have been identified, no tool for systematic assessment of EBI severity has been established so far. This study aimed to develop an EBI grading system based on clinical signs and neuroimaging for estimation of EBI severity at admission. This is a retrospective observational study assessing imaging parameters (intracranial blood amount, global cerebral edema (GCE)), and clinical signs (persistent loss of consciousness [LOC]) representative for EBI. The intracranial blood amount was semi-quantitatively assessed. One point was added for GCE and LOC, respectively. All points were summed up resulting in an EBI grading ranging from 1 to 5. The estimated EBI severity was correlated with progressive GCE requiring decompressive hemicraniectomy (DHC), DCI-associated infarction, and outcome according to the modified Rankin scale (mRS) at 3-month-follow up. A consecutive cohort including 324 aSAH-patients with a mean age of 55.9 years, was analyzed. The probability of developing progressive GCE was 9% for EBI grade 1, 28% for EBI grade 2, 43% for EBI grade 3, 61% for EBI grade 4, and 89% for EBI grade 5. The EBI grading correlated significantly with the need for DHC (r = 0.25, p < 0.0001), delayed infarction (r = 0.30, p < 0.0001), and outcome (r = 0.31, p < 0.0001). An EBI grading based on clinical and imaging parameters allowed an early systematic estimation of EBI severity with a higher EBI grade associated not only with a progressive GCE but also with DCI and poor outcome.</p>","PeriodicalId":19184,"journal":{"name":"Neurosurgical Review","volume":"47 1","pages":"838"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11549151/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgical Review","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10143-024-03081-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
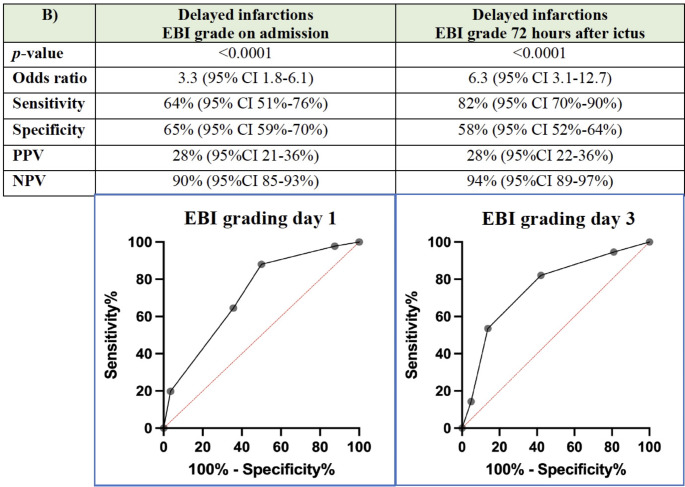
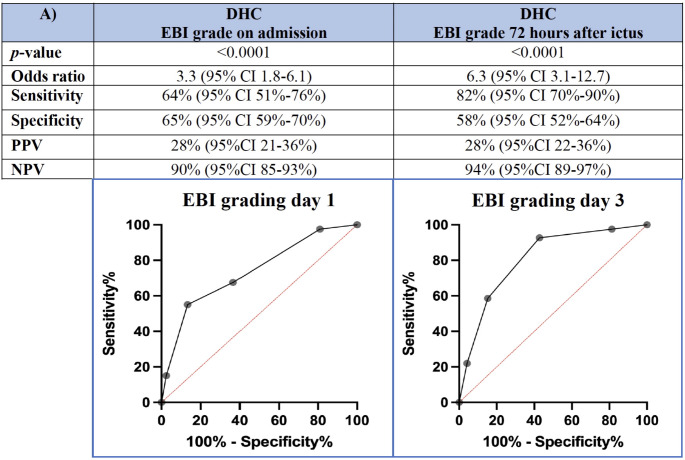
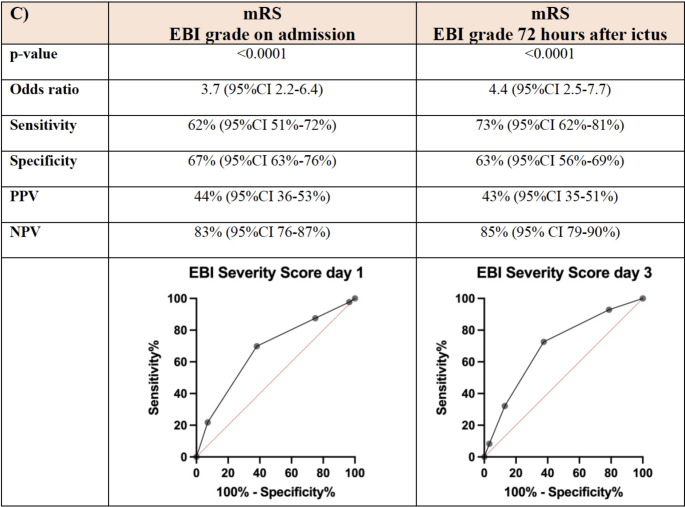
Early brain injury (EBI) after aneurysmal subarachnoid hemorrhage (aSAH) has been increasingly recognized as a risk factor for delayed cerebral ischemia (DCI). While several clinical and radiological EBI biomarkers have been identified, no tool for systematic assessment of EBI severity has been established so far. This study aimed to develop an EBI grading system based on clinical signs and neuroimaging for estimation of EBI severity at admission. This is a retrospective observational study assessing imaging parameters (intracranial blood amount, global cerebral edema (GCE)), and clinical signs (persistent loss of consciousness [LOC]) representative for EBI. The intracranial blood amount was semi-quantitatively assessed. One point was added for GCE and LOC, respectively. All points were summed up resulting in an EBI grading ranging from 1 to 5. The estimated EBI severity was correlated with progressive GCE requiring decompressive hemicraniectomy (DHC), DCI-associated infarction, and outcome according to the modified Rankin scale (mRS) at 3-month-follow up. A consecutive cohort including 324 aSAH-patients with a mean age of 55.9 years, was analyzed. The probability of developing progressive GCE was 9% for EBI grade 1, 28% for EBI grade 2, 43% for EBI grade 3, 61% for EBI grade 4, and 89% for EBI grade 5. The EBI grading correlated significantly with the need for DHC (r = 0.25, p < 0.0001), delayed infarction (r = 0.30, p < 0.0001), and outcome (r = 0.31, p < 0.0001). An EBI grading based on clinical and imaging parameters allowed an early systematic estimation of EBI severity with a higher EBI grade associated not only with a progressive GCE but also with DCI and poor outcome.
期刊介绍:
The goal of Neurosurgical Review is to provide a forum for comprehensive reviews on current issues in neurosurgery. Each issue contains up to three reviews, reflecting all important aspects of one topic (a disease or a surgical approach). Comments by a panel of experts within the same issue complete the topic. By providing comprehensive coverage of one topic per issue, Neurosurgical Review combines the topicality of professional journals with the indepth treatment of a monograph. Original papers of high quality are also welcome.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
