Noam Goder, Lilach Zac, Nadav Nevo, Fabian Gerstenhaber, Or Goren, Barak Cohen, Idit Matot, Guy Lahat, Eran Nizri
{"title":"Thromboelastogram changes are associated with postoperative complications after cytoreductive surgery.","authors":"Noam Goder, Lilach Zac, Nadav Nevo, Fabian Gerstenhaber, Or Goren, Barak Cohen, Idit Matot, Guy Lahat, Eran Nizri","doi":"10.1515/pp-2023-0018","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) is used to treat peritoneal surface malignancies. However, surgical morbidity is high, and prediction of severe postoperative complications (SPC) is limited. We hypothesized that the changes in thromboelastogram (TEG) values following CRS could be associated with SPC.</p><p><strong>Methods: </strong>We retrospectively analyzed a cohort of CRS and HIPEC patients who had TEG measured before and after CRS. Clinical and postoperative data were retrieved from a prospectively maintained database.</p><p><strong>Results: </strong>Our 37-patient cohort was comprised of 24 men and 13 women with an age (median, [interquartile range, IQR]) 55 (47-65) years, of whom six had SPC. The ones with SPC did not differ from the others in age, sex, tumor histology or preoperative chemotherapy. The extent of surgery as measured by the peritoneal carcinomatosis index and the number of organs resected was comparable between SPC group vs. no SPC [9 (3-10.5) vs. 9 (5-14), p=1.0; 2 (0.75-2.25) vs. 2 (1-3), p=0.88, respectively]. The TEG parameters showed increased R- and K- time for the patients with SPC compared to those without (6 ± 3.89 vs. 4.05 ± 1.24, p=0.01; 1.65 ± 0.63 vs. 1.25 ± 0.4, p=0.03, respectively). The TEG values were significantly associated with SPC in the multivariable analysis (odds ratio=1.53, p=0.05).</p><p><strong>Conclusions: </strong>TEG changes are associated with SPC. Intra-operative markers of SPC could guide intraoperative decisions, such as stool diversion and postoperative triage of patients to an appropriate level of care.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"9 3","pages":"113-119"},"PeriodicalIF":2.4000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558171/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2023-0018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) is used to treat peritoneal surface malignancies. However, surgical morbidity is high, and prediction of severe postoperative complications (SPC) is limited. We hypothesized that the changes in thromboelastogram (TEG) values following CRS could be associated with SPC.
Methods: We retrospectively analyzed a cohort of CRS and HIPEC patients who had TEG measured before and after CRS. Clinical and postoperative data were retrieved from a prospectively maintained database.
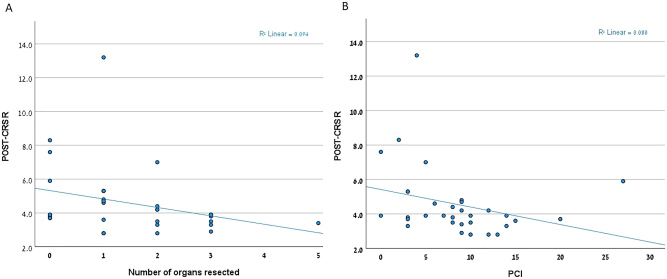
Results: Our 37-patient cohort was comprised of 24 men and 13 women with an age (median, [interquartile range, IQR]) 55 (47-65) years, of whom six had SPC. The ones with SPC did not differ from the others in age, sex, tumor histology or preoperative chemotherapy. The extent of surgery as measured by the peritoneal carcinomatosis index and the number of organs resected was comparable between SPC group vs. no SPC [9 (3-10.5) vs. 9 (5-14), p=1.0; 2 (0.75-2.25) vs. 2 (1-3), p=0.88, respectively]. The TEG parameters showed increased R- and K- time for the patients with SPC compared to those without (6 ± 3.89 vs. 4.05 ± 1.24, p=0.01; 1.65 ± 0.63 vs. 1.25 ± 0.4, p=0.03, respectively). The TEG values were significantly associated with SPC in the multivariable analysis (odds ratio=1.53, p=0.05).
Conclusions: TEG changes are associated with SPC. Intra-operative markers of SPC could guide intraoperative decisions, such as stool diversion and postoperative triage of patients to an appropriate level of care.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
