{"title":"Close Contact Transillumination Light Guides Surgeon to Vaginal Point Aa: Pharus Method for Robot-Assisted Sacrocolpopexy","authors":"Akiko Yoshida Ueno, Takayuki Sato, Michiya Kobayashi, Shinya Wakatsuki, Takaomi Namba, Kazutoshi Hayashi","doi":"10.1111/ases.13412","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>In robot-assisted sacrocolpopexy (RSC) for patients with cystocele, accurate identification of the vaginal point Aa from the serosal side is crucial for surgical mesh placement in the appropriate position. We developed a novel Pharus method for exactly locating the point Aa for RSC.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In the Pharus method, the tip of a rigid endoscope was placed directly on the vaginal point Aa. In a preliminary experiment, we observed LED lights with different wavelengths of 450–870 nm using the Firefly imaging system to evaluate which wavelengths of light were captured by the Firefly mode. In a clinical study, the Pharus method was employed in four patients with Stage II or more advanced cystocele undergoing RSC. For comparison, a near-infrared fluorescence method by indocyanine green (ICG) tattooing at the point Aa was also performed. The visibility of each method was evaluated under Firefly-mode imaging.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In the preliminary experiment, visible LED lights with wavelengths ≤ 720 nm, and near-infrared LED lights with wavelengths ≥ 830 nm were detected by the Firefly mode. In RSC using the Pharus method, the point Aa of each patient was clearly highlighted as a green spot from the serosal side by the endoscopic white light penetrating the vaginal wall with a thickness of 3.3–4.6 mm. Compared with the ICG tattooing method, the Pharus method showed superior visibility in all patients.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The transillumination light effectively guided the surgeon to the vaginal point Aa, which can be likened to the Latin word “pharus,” meaning lighthouse.</p>\n </section>\n </div>","PeriodicalId":47019,"journal":{"name":"Asian Journal of Endoscopic Surgery","volume":"18 1","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2024-11-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ases.13412","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Journal of Endoscopic Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ases.13412","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
In robot-assisted sacrocolpopexy (RSC) for patients with cystocele, accurate identification of the vaginal point Aa from the serosal side is crucial for surgical mesh placement in the appropriate position. We developed a novel Pharus method for exactly locating the point Aa for RSC.
Methods
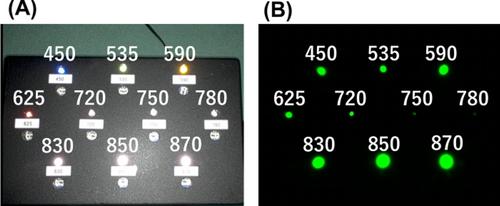
In the Pharus method, the tip of a rigid endoscope was placed directly on the vaginal point Aa. In a preliminary experiment, we observed LED lights with different wavelengths of 450–870 nm using the Firefly imaging system to evaluate which wavelengths of light were captured by the Firefly mode. In a clinical study, the Pharus method was employed in four patients with Stage II or more advanced cystocele undergoing RSC. For comparison, a near-infrared fluorescence method by indocyanine green (ICG) tattooing at the point Aa was also performed. The visibility of each method was evaluated under Firefly-mode imaging.
Results
In the preliminary experiment, visible LED lights with wavelengths ≤ 720 nm, and near-infrared LED lights with wavelengths ≥ 830 nm were detected by the Firefly mode. In RSC using the Pharus method, the point Aa of each patient was clearly highlighted as a green spot from the serosal side by the endoscopic white light penetrating the vaginal wall with a thickness of 3.3–4.6 mm. Compared with the ICG tattooing method, the Pharus method showed superior visibility in all patients.
Conclusion
The transillumination light effectively guided the surgeon to the vaginal point Aa, which can be likened to the Latin word “pharus,” meaning lighthouse.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
