Andrzej Głowniak, Anna Drelich-Zbroja, Adam Tarkowski, Paweł Marzęda, Katarzyna Wojewoda, Katarzyna Wysokińska, Anna Wysocka, Monika Miazga, Anna Jaroszyńska, Krzysztof Kaczmarek, Andrzej Jaroszyński, Michał Orczykowski
{"title":"Silent cerebral ischemic lesions in ablation-naïve patients with non-valvular atrial fibrillation: Does the pulmonary vein anatomy matter?","authors":"Andrzej Głowniak, Anna Drelich-Zbroja, Adam Tarkowski, Paweł Marzęda, Katarzyna Wojewoda, Katarzyna Wysokińska, Anna Wysocka, Monika Miazga, Anna Jaroszyńska, Krzysztof Kaczmarek, Andrzej Jaroszyński, Michał Orczykowski","doi":"10.5603/cj.99142","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Silent cerebral ischemic lesions (SCILs) detected by magnetic resonance imaging (MRI) can precede symptomatic stroke, the risk of which is increased five-fold in atrial fibrillation (AF) patients. In our study, we aimed to evaluate the initial incidence of SCILs in the population of patients referred for ablation due to symptomatic AF and to identify possible risk factors.</p><p><strong>Methods: </strong>A total of 110 patients, with a mean age (SD) of 59.9 (9.4) years, referred for ablation, were included in the study. In all patients, MRI was performed before the procedure to evaluate the incidence of SCILs in the ablation-naïve patients.</p><p><strong>Results: </strong>MRI revealed preexisting SCIL in 81/110 patients (73.6%). Notably, SCILs were found in all patients with CHA₂DS₂-VASc score ≥ 4. In univariable analysis, age (p < 0.001), CHA₂DS₂-VASc score (p = 0.001), hypertension (p = 0.01), and anticoagulation duration (p = 0.023) were identified as significant risk factors for SCILs, while the presence of anatomical variants of left-sided common pulmonary veins trunk (LCPV) had negative prognostic value (p = 0.026). Multivariable logistic regression analysis identified age (p < 0.001) as the risk factor of preexisting SCILs, whereas the presence of LCPV trunk was associated with significantly lower (p = 0.005) SCILs incidence.</p><p><strong>Conclusions: </strong>Silent cerebral ischemic lesions detected in MRI are frequent in the population of patients with non-valvular AF. The incidence of SCILs is higher in patients with long history of arrhythmia and higher CHA₂DS₂-VASc score. The relationship between the anatomy of pulmonary veins and the incidence of SCILs needs further investigation.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"35-42"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11870011/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.99142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
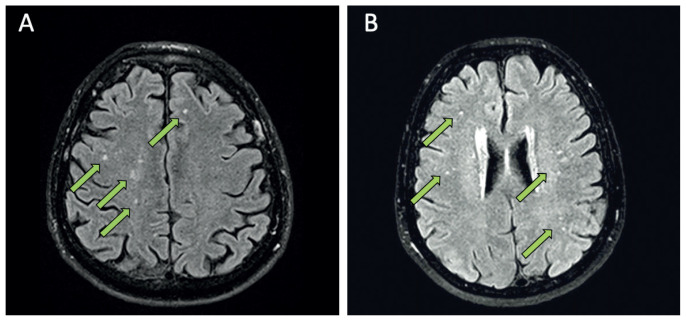
Background: Silent cerebral ischemic lesions (SCILs) detected by magnetic resonance imaging (MRI) can precede symptomatic stroke, the risk of which is increased five-fold in atrial fibrillation (AF) patients. In our study, we aimed to evaluate the initial incidence of SCILs in the population of patients referred for ablation due to symptomatic AF and to identify possible risk factors.
Methods: A total of 110 patients, with a mean age (SD) of 59.9 (9.4) years, referred for ablation, were included in the study. In all patients, MRI was performed before the procedure to evaluate the incidence of SCILs in the ablation-naïve patients.
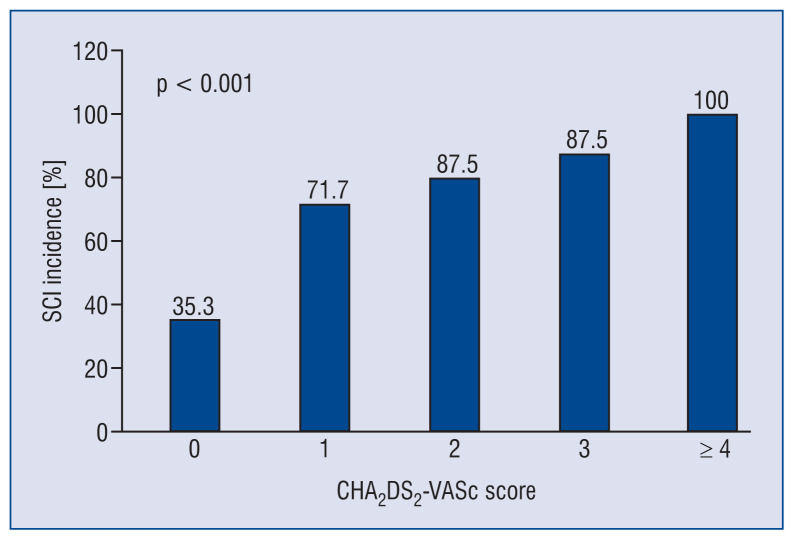
Results: MRI revealed preexisting SCIL in 81/110 patients (73.6%). Notably, SCILs were found in all patients with CHA₂DS₂-VASc score ≥ 4. In univariable analysis, age (p < 0.001), CHA₂DS₂-VASc score (p = 0.001), hypertension (p = 0.01), and anticoagulation duration (p = 0.023) were identified as significant risk factors for SCILs, while the presence of anatomical variants of left-sided common pulmonary veins trunk (LCPV) had negative prognostic value (p = 0.026). Multivariable logistic regression analysis identified age (p < 0.001) as the risk factor of preexisting SCILs, whereas the presence of LCPV trunk was associated with significantly lower (p = 0.005) SCILs incidence.
Conclusions: Silent cerebral ischemic lesions detected in MRI are frequent in the population of patients with non-valvular AF. The incidence of SCILs is higher in patients with long history of arrhythmia and higher CHA₂DS₂-VASc score. The relationship between the anatomy of pulmonary veins and the incidence of SCILs needs further investigation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
