{"title":"Innominate Artery Translocation with Hemiarch Replacement Strategy for Acute Type A Aortic Dissection: a Single-Center Study.","authors":"Amarit Phothikun, Nutthayuth Kanokkavinvong, Weerachai Nawarawong, Noppon Taksaudom, Surin Woragidpoonpol","doi":"10.1055/s-0044-1795129","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.</p><p><strong>Methods: </strong> Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.</p><p><strong>Results: </strong> The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.</p><p><strong>Conclusion: </strong> Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"60-69"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879489/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1795129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
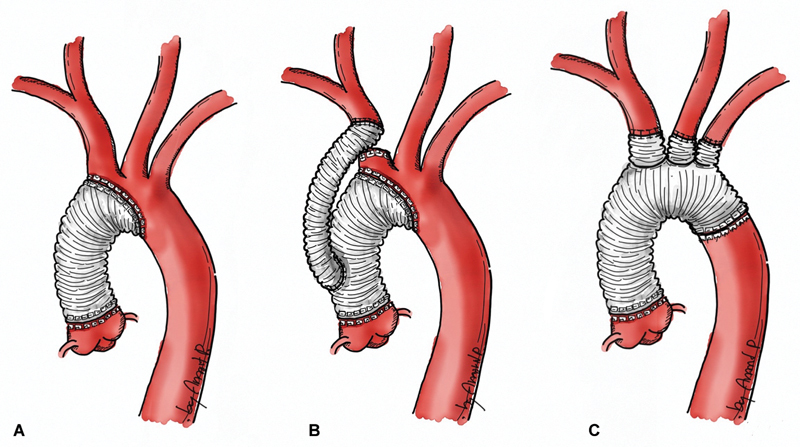
Background: Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.
Methods: Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.
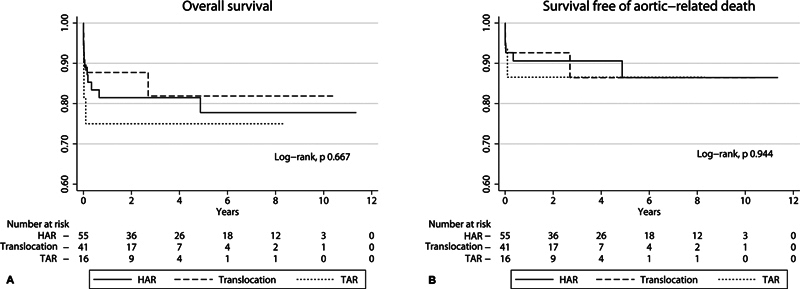
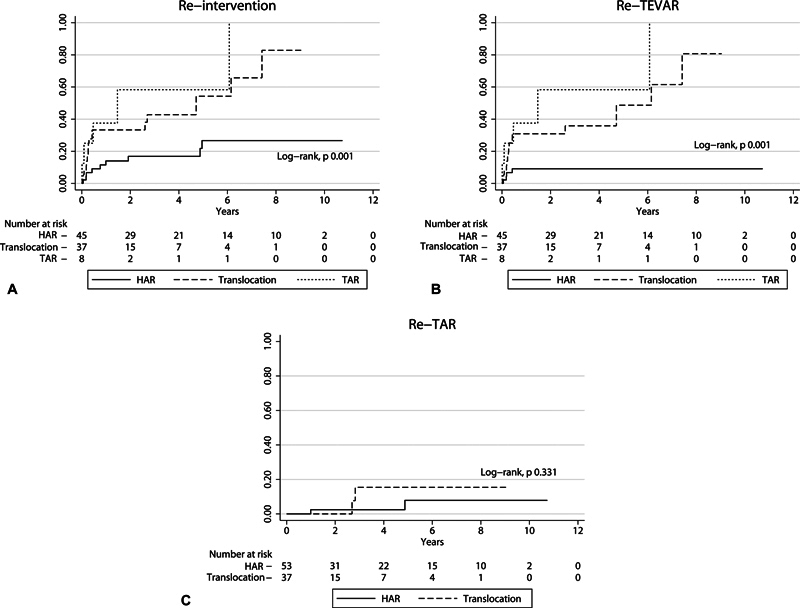
Results: The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.
Conclusion: Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
