A Retrospective Cohort Study Comparing Different Cannulation Strategies in Type A Aortic Dissection Surgery: 20-year Single-Center Experience in a Referral Center.
Nicolas Nunez-Ordonez, Julian Senociain, Juan Pablo Umaña, Andres Felipe Amado-Olivares, Carlos Andrés Villa, Carlos Obando, Jaime Camacho
{"title":"A Retrospective Cohort Study Comparing Different Cannulation Strategies in Type A Aortic Dissection Surgery: 20-year Single-Center Experience in a Referral Center.","authors":"Nicolas Nunez-Ordonez, Julian Senociain, Juan Pablo Umaña, Andres Felipe Amado-Olivares, Carlos Andrés Villa, Carlos Obando, Jaime Camacho","doi":"10.1055/s-0045-1802993","DOIUrl":null,"url":null,"abstract":"<p><p>Type A aortic dissection as a highly lethal disease continues being a great challenge for cardiac surgeons worldwide. There are still unanswered questions regarding intraoperative decisions and their impact on the surgical outcomes. The aim of this study is to compare postoperative outcomes according to site of cannulation in patients with acute Type A aortic dissection (ATAAD).This was a retrospective cohort study. We included all ATAAD procedures from January 2002 to November 2023. We defined groups according to site of cannulation (aorta, axillary, femoral, innominate). Data from pre-, intra-, and postoperative variables were collected. Our main outcomes were spinal cord injury (SCI), stroke rate, and in-hospital mortality. Between-group comparisons were performed using standard statistical tests and post hoc tests adjusting for multiple comparisons were performed.We identified 127 ATAAD procedures. Reoperation for bleeding was significantly higher in the femoral cannulation group (75%, <i>p</i> = 0.0006). There were no statistically significant differences in acute kidney injury rate (<i>p</i> = 0.012), SCI rate (<i>p</i> = 0.78), or in-hospital mortality (<i>p</i> = 0.75). Our data suggest that there is a lower stroke rate in the axillary cannulation group (3.6%, <i>p</i> = 0.4), which did not reach statistical significance.Choosing an adequate cannulation site is a critical step in TAAD surgery. In our series, axillary and innominate cannulation were the preferred methods with relatively low complication rates.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"80-85"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11961217/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1802993","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
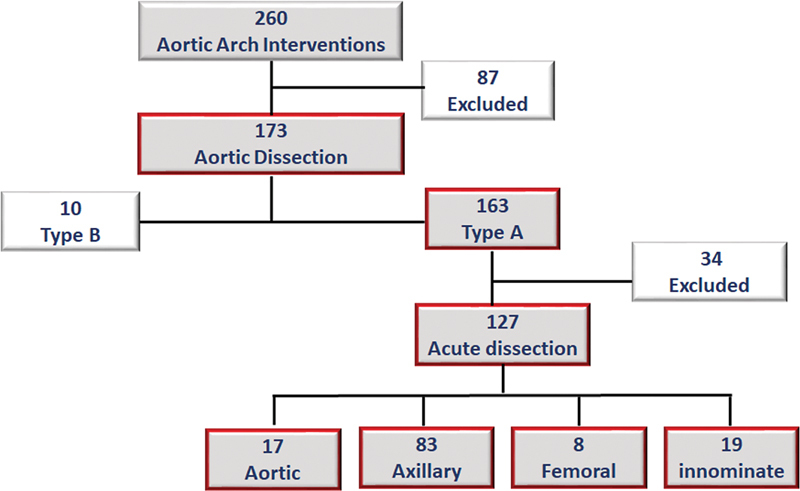
Type A aortic dissection as a highly lethal disease continues being a great challenge for cardiac surgeons worldwide. There are still unanswered questions regarding intraoperative decisions and their impact on the surgical outcomes. The aim of this study is to compare postoperative outcomes according to site of cannulation in patients with acute Type A aortic dissection (ATAAD).This was a retrospective cohort study. We included all ATAAD procedures from January 2002 to November 2023. We defined groups according to site of cannulation (aorta, axillary, femoral, innominate). Data from pre-, intra-, and postoperative variables were collected. Our main outcomes were spinal cord injury (SCI), stroke rate, and in-hospital mortality. Between-group comparisons were performed using standard statistical tests and post hoc tests adjusting for multiple comparisons were performed.We identified 127 ATAAD procedures. Reoperation for bleeding was significantly higher in the femoral cannulation group (75%, p = 0.0006). There were no statistically significant differences in acute kidney injury rate (p = 0.012), SCI rate (p = 0.78), or in-hospital mortality (p = 0.75). Our data suggest that there is a lower stroke rate in the axillary cannulation group (3.6%, p = 0.4), which did not reach statistical significance.Choosing an adequate cannulation site is a critical step in TAAD surgery. In our series, axillary and innominate cannulation were the preferred methods with relatively low complication rates.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
